










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkApoyo militar al establecimiento de reservas estratégicas europeas de recursos sanitarios frente a las pandemias
Military support for the establishment of European strategic reserves of strategic medical stockpiles against pandemics
Moderador / Chair: coronel Far. Francisco Javier Alfaro Matos. España. Spain
Relator / Rapporteur: teniente coronel Far. René Pita Pita. España. Spain
Conferencias / Conferences:
Costs for a Hospital stay in patients with COVID-19. Ms Floria Mariana. Rumanía. Romania
Controlling SARS-CoV-2 spread in a veteran Nursing Home: contingency plan implementation and monitoring. Coronel Med. Maria Lopes Salazar. Portugal.
Portuguese Military program to Nursing Homes. Coronel Med. Maria Lopes Salazar. Portugal.
The Spanish National Strategic medicines and medical devices reserve management model. Teniente coronel Far. María del Pilar Puente Águeda. España. Spain.
Building up stocks of medical countermeasures against pandemics: the place of the French Military Health Service in the response mechanism of the armed forces and the nation. Coronel Med. Laurence Calvo. Francia. France.
A responsive medical capability building. Lessons learned from the COVID-19 crisis. Coronel Med. Antoine Luft. Francia. France.

Costes de una estancia hospitalaria en pacientes con la COVID-19. Ms Floria Mariana. Rumanía / Costs for a hospital stay in patients with COVID-19
Moraru A. C.1, Galatanu D.1, 2, Grumeza A.1, 2, Gorea_Bocinca C.1, Floria M.1, 2
Background
Profiles of COVID-19 patients have many potential applications. Besides determining risk factors, influencing treatment protocols, setting priorities for eventual vaccination distribution, or inspiring further research, planning and budgeting for use of healthcare resources and services is very important. Material and methods. The national protocol for the treatment of COVID-19 infection was applied. Inpatient COVID-19 hospitalizations costs were analyzed regardless of ICD-10 procedure codes. Results. In our hospital during the first three waves of COVID-19 pandemia was hospitalized 241 patients with/without comorbidities: 43% with moderate and 21% with severe forms; age of 59.92±7.8 years, 46 % men, 26 % military personnel, 11.57±3 days of hospitalization. COVID-19 manifestations were: 69 % respiratory (18 % with severe pneumonia), 3.3 % with cardiac (2.9 % with pulmonary embolism, diagnosed by angioCT), 28 % digestive and 33 % psychiatric (most common anxiety). The average estimated costs were about 3000E/patient, without significantly differences depending on disease severity. Equipment costs were 2 times higher than for drugs and 4 times than for laboratory tests. Conclusion. In a small military hospital that cared for predominantly moderate forms of COVID-19 infection, the costs for equipment were much higher than for drugs.
Control de la propagación del SARS-CoV-2 en una residencia de veteranos: implementación y seguimiento del plan de contingencia. Coronel Med. Maria Lopes Salazar. Portugal / Controlling SARS-CoV-2 spread in a veteran nursing home: contingency plan implementation and monitoring
Salazar M.1, Fernandes D., Laureano F., Castro J.
Nursing homes are major hotspots of SARS-CoV-2 dissemination and account for a significant site-related infection and mortality of COVID-19 pandemics. We implemented and monitored a COVID-19 contingency plan in a Portuguese veteran nursing home hosting 90 residents and 153 staff members and located in Runa, a rural area. Over 85 % of residents were over 79 years of age, and less than 40 % scored as independent in the Barthel scale. The majority of staff (62 %) was classified as having close contact with residents.
A cross-sectional screening in April 2020 uncovered three RT-PCR positive tests for SARS-CoV-2 among all residents while no staff member was found positive. After these initial infections, the staff was offered a training program focused on control -measures and a contingency plan was implemented to control infection spreading. Exposure to the virus was monitored by longitudinal serological testing performed in May, July and November 2020 in all residents and in 80% of the staff members. Only three anti-SARS-CoV-2 IgG positive cases were found in May. Eventually these three residents became sero-negative by November while only one new case of anti-SARS-CoV-2 IgG positivity was found in November.
Overall, in this six-month monitoring period the cumulative anti-SARS-CoV-2 IgG prevalence was under 2.4 %. This result indicates that exposure to the virus was highly contained during this period strongly suggesting that strict implementation of infection control measures effectively minimized the risk of COVID-19 infection spreading in this veteran nursing home.
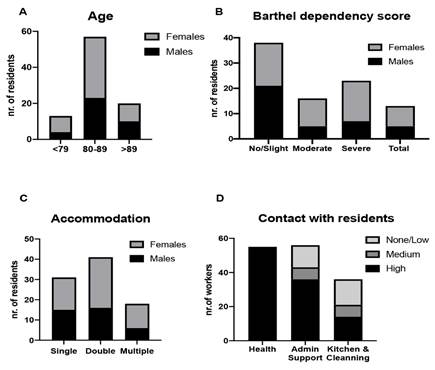
Figure. Characterization of nursing home residents and staff members. Age stratification (A), dependency score using Barthel scale (B) type of accommodation (single, double or multiple bedroom) (C) and are represented for the entire resident group by stratified by gender. Degree of contact of staff members with residents was ascertained in 3 different functional groups (healthcare, admin, and support services, Kitchen and cleaning staff) (D).
Programa militar portugués para residencias de ancianos. Coronel Med. Maria Lopes Salazar. Portugal / Portuguese Military Training Program to Nursing Homes’ Staff
Salazar M., Pereira J., Farinha L., Fernandes H., Martins J., Castro J.
Nursing homes are major hotspots of SARS-CoV2 dissemination and account for a significant site-related infection and mortality of COVID-19 patients. The European Centre for Disease Control estimated a 66% mortality rate of COVID-19 cases from nursing home residents.
Portugal registered around 30 % of its country’s COVID-19 deaths, from nursing home residents. At the beginning of our second wave, in October 2020, the government launched a new distress call to the military to prevent outbreaks in these institutions by training their staff in CBRN methods, continuing the previous support of disinfecting buildings, helping to contact tracing and providing beds at military hospitals.
The PRT Armed Forces Health System put up a two-step COVID-19 Training Program to all nursing home staff (2700 institutions). The first step was visiting nursing homes to present a lecture on COVID-19 prevention methods. The second step was a four-day online training program using Microsoft Teams® software, ran by health-related military personnel (doctors, nurses, pharmacists, …), about COVID-19 prevention measures (COVID-19 general preventive rules; staff/residents and food/laundry circuits; use of PPE and cleaning/disinfection products & protocols). This support was extended to home support services and temporary homing facilities.
During this eight-month period, the PRT Armed Forces were able to reach 90 % of all nursing homes and maintain the 4 themed-based online sessions, four days a week. We ran a total of 120 sessions, repeatedly from October 2020 until June 2021. After the online sessions, the institutions’ health personnel had the chance to pose questions about specific local problems. A quality survey was also implemented, showing that the staff considered these sessions very useful, having a very grateful feeling of companionship and support by governmental institutions.
El modelo de gestión de la Reserva Nacional Estratégica de medicamentos y productos sanitarios / The Spanish National Strategic Medicines and Medical Devices Reserve Management Model
Teniente coronel Far. Puente Águeda M.P1. España
Stockpiling medicines and medical devices for emergencies and disasters is legally entrusted to the Spanish Ministry of Health. The Spanish Ministry of Defence has collaborated with Health -Authorities in the manufacture and storage of strategic medicines for some time. The Spanish Medicines Agency and the Military Medical Directorate are the Governmental Entities who lead these official agreements. During the COVID-19 pandemic, the Spanish Government decided to establish an interdepartmental Commission to create and sustain the strategic national levels for healthcare material (medicines, medical devices, personal protective equipment and other products).
The Ministry of Health is in charge of defining the composition of this stockpile in order to support the reserves of the Spanish -Autonomous Communities because it has the most accurate information about the risks and the required resources. Spanish legislation has had the process of centralized procurement of medicines and medical devices in place for some time. This procedure is intended to promote the economies of scale and interoperability within the National Health System. This joint procurement is also led and coordinated by the Spanish Ministry of Health. The pharmaceutical storage and transport capabilities of the Ministry of Defence are a guarantee of quality, safety, and commitment. In addition, this procedure is a return on public investment and provides a benefit for Spanish Society. Both Ministries collaborate closely to develop the models for efficient management of the reserve. It will be necessary to carry out a continuous inventory rotation by making possible its consumption. The evolution of the reserve levels will need to be continuously updated to align with Spain’s health situation.
Nowadays, at the beginning of post-just-in-time era, the Military Pharmacy has an important role to play in the storage and transport of medical material, which are capabilities of strategic interest for National Security. This model, where the Spanish Government supports the Autonomous Communities with its strategic stockpile, could be extrapolated to the European Union and its Member States. A European Military Health Service in defence of the Health of the Europeans.
Creación de reservas de contramedidas sanitarias frente a pandemias: el lugar del Servicio Miliar Sanitario de las Fuerzas Armadas y la nación. Coronel Med Laurence Calvo. Francia / Building up stocks of medical countermeasures against pandemics: the place of the French Military Health Service in the response mechanism of the armed forces and the nation
Calvo L.1
One of the main lessons learned from the COVID-19 pandemic highlights the need to build up strategic stocks. The nature of these stocks, the quantities of each product, their strategic or non-strategic nature, and their financing, are determined by different factors. Among these, various aspects are unavoidable: the size of the stocks, the financial aspects, underpinned by availability in the event of a major crisis, industrial production control, and national sovereignty, including the availability of raw materials.
The French Military Health Service’s thinking in this area is led by the General Directorate, CBRNe branch, in coordination, with the medical supply chain, including users, military hospitals, and forces medicine. It is driven by the absolute necessity to cover the needs of the armed forces first, and foremost, but also for the -Ministry of the Armed Forces to participate in the nation’s resilience effort
Lecciones aprendidas de la crisis de la COVID-19. Coronel Med. Antoine Luft. Francia / A responsive medical capability building. Lessons learned from the COVID-19 crisis
Capability building is a long-term endeavour. Given equipment complexity, the process of preparing for the next challenge can endure for several years. However, equipment alone is unlikely to surmount future challenges entirely and often requires frequent adjustments to be fully effective. In a crisis situation, the organisation is under stress and often is also caught by surprise. The impact of this surprise can be reduced by scenario planning and anticipation. This goes some way to enabling a level of tailored response planning thus lessening the challenge of capability building under pressure.
This happened during the Malian security crisis in 2013. Deploying an operational medical support system was not a major problem. In contrast, the Ebola crisis in 2015 required a reactive approach in order to deploy a medical treatment facility for -caregivers in just a few months.
The COVID-19 crisis is on a different scale. In a few days, it was necessary to develop and produce operational medical units responding to specific requirements not covered by existing capabilities.
The Service de Santé des Armées (SSA) relied on its autonomous and reactive medical equipment procurement capability, which was a major advantage. However, this capability may be facing difficulties associated with a general context of shortage induced by resource competition and the disruption of supply chains. For this reason, having a strategic equipment storage policy is essential.
In this way the SSA benefited from the medical capabilities necessary for its routine operations and to fulfill its operational mission. However, reactive capability development and engineering was required to capitalise on these resources and to produce appropriate capabilities for the COVID-19 crisis.
Once the initial response had been delivered, it was necessary to consider the longer term challenge. The Armed Forces had to constantly measure their resources and reinforce the public health system as needed while preserving their ability to fulfill their missions.
In response to the challenge the SSA capitalised on its equipment stocks and skills, deploying a high-capacity ICU under time pressure, strengthening ICU capabilities in operational areas and reinforcing the French military’s strategic airlift capability for critical patients.
