










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkREC: Interventional Cardiology
versão On-line ISSN 2604-7276versão impressa ISSN 2604-7306
REC Interv Cardiol ES vol.5 no.1 Madrid Jan./Mar. 2023 Epub 18-Mar-2024
https://dx.doi.org/10.24875/recic.m22000309
IMAGES IN CARDIOLOGY
Rescate de torsión de endoprótesis mediante doble capa de CP stent
Bail-out double-layer CP stent implantation due to severe endoprosthesis kinking
Bail-out double-layer CP stent implantation due to severe endoprosthesis kinking
aSección de Cardiología Intervencionista, Hospital Universitario de Cruces, Baracaldo, Vizcaya, España
bServicio de Cirugía Cardiaca, Hospital Universitario de Cruces, Baracaldo, Vizcaya, España
This is the case of a 53-year-old man with aortic stenosis, ascending aortic aneurysm, and type B aortic dissection treated with Bentall procedure where a 40 mm uncovered self-expanding stent-graft (AMDS, JOTEC GmbH, Germany) was anastomosed to the aortic graft distal border with the intent to collapse the entry (figure 1A). The patient's written informed consent was obtained to run the tests and publish the case.
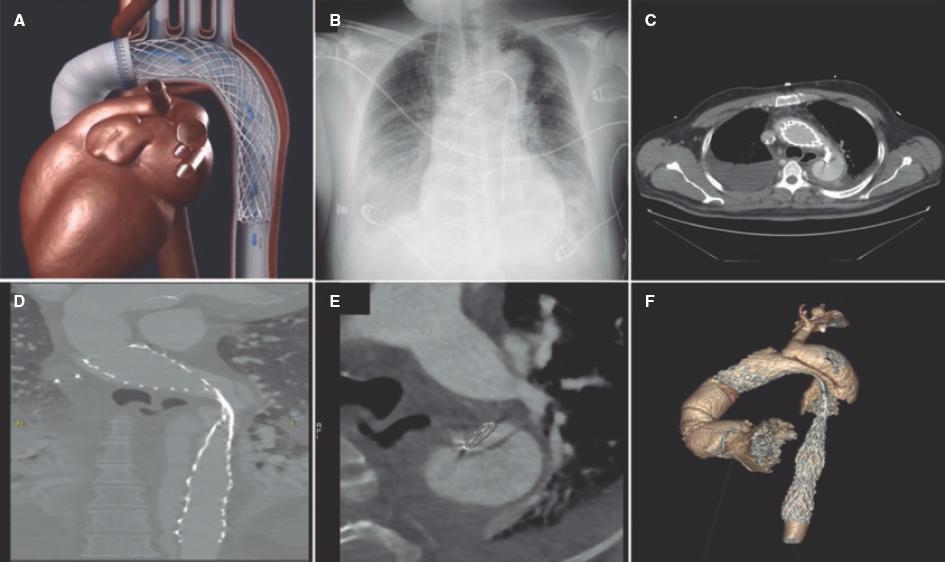
The follow-up radiographic monitoring revealed significant stent-graft kinking while the dissection entry remained opened (figure 1B,F).
Given the high risk involved in the reintervention, endovascular treatment was decided. Under intravascular echocardiography guidance a hydrophilic guidewire was used to cross the stent-graft lumen. Afterwards, the guidewire was exchanged for a different one with stronger support to proceed with dilatations using semi-compliant balloons with significant recoil being reported after balloon deflation (figure 2A,C).
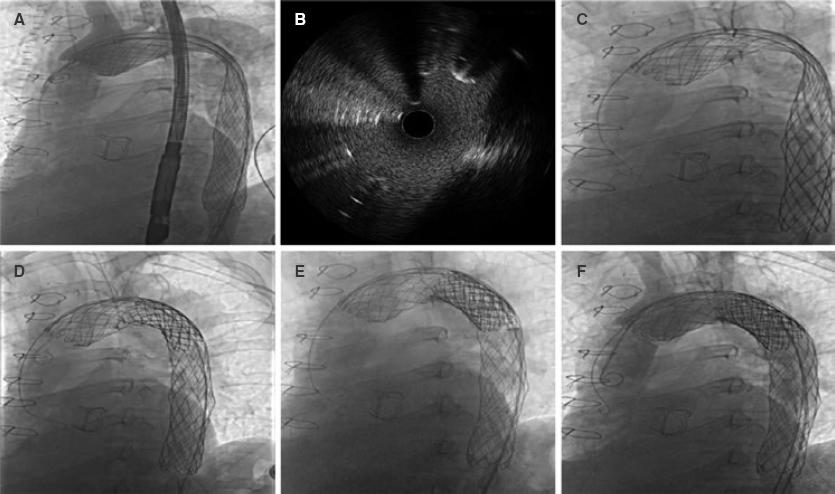
To achieve greater radial strength, we decided to implant a double-layer stent. An uncovered stent to expand the stent-graft was implanted followed by 1 covered expandable polytetrafluoroethylene (e-PTFE) stent to seal the dissection entry. An 18 Fr DrySeal sheath (Gore Inc, United States) was used to implant 2 60 mm 10-zig CP stents (NuMED Inc, United States), 1 covered and the other one not. Both stents were mounted on a 26 mm × 50 mm BIB balloon (NuMED Inc., United States). A 30 mm × 60 mm Crystal balloon (BALT, Germany) was used for postdilatation (figure 2D,E). The control computed tomography scan confirmed the dissection entry complete seal with persistent distal false lumen (figure 3A,D).

Received: February 28, 2022; Accepted: May 30, 2022
 Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
