










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
The contents of the inguinal hernia sac may vary from intraperitoneal fat, small or large bowel, bladder, ovaries, and appendix [1]. An Amyand's hernia is a rare type of hernia, characterized by the presence of the appendix, either inflamed or normal, in the inguinal hernia sac. When symptoms do appear, they mimic an incarcerated hernia [2]. The incidence of occurrence of an inflamed or perforated incarcerated appendix in Amyand's hernia is 0.1% of all cases of appendicitis [3]. Amyand's hernia typically presents on the right side. On physical examination, there is tenderness and swelling in the inguinal or inguinoscrotal region [4]. It is clinically difficult to differentiate Amyand's hernia from an inguinal hernia due to their similar presentations. An Amyand's hernia is a diagnostic challenge due to its rarity and diagnosis is often incidental, on imaging or intra-operatively [5, 6, 7]. Imaging tests such as ultrasound (US) and computed tomography (CT) aid in distinguishing the pathologies [5, 7, 8]. Computed tomography (CT) allows direct visualization of the appendix inside the inguinal canal and it helps make an accurate diagnosis [5]. Fernando et al. classified the Amyand's hernia according to the degree of inflammation of the appendix in three types: (A) intact appendix without signs of inflammation; (B) appendix with signs of inflammation; and (C) perforated appendix [9]. Type A accounting for nearly 90% of all cases [9]. Types B and C mandate appendectomy.
This report aims to describe a case of an appendix with signs of inflammation in the inguinal hernia sac, that is rare and difficult to diagnose the condition and highlights the importance of early CT scanning in reaching the exact and early diagnosis of Amyand's hernia.
CASE REPORT
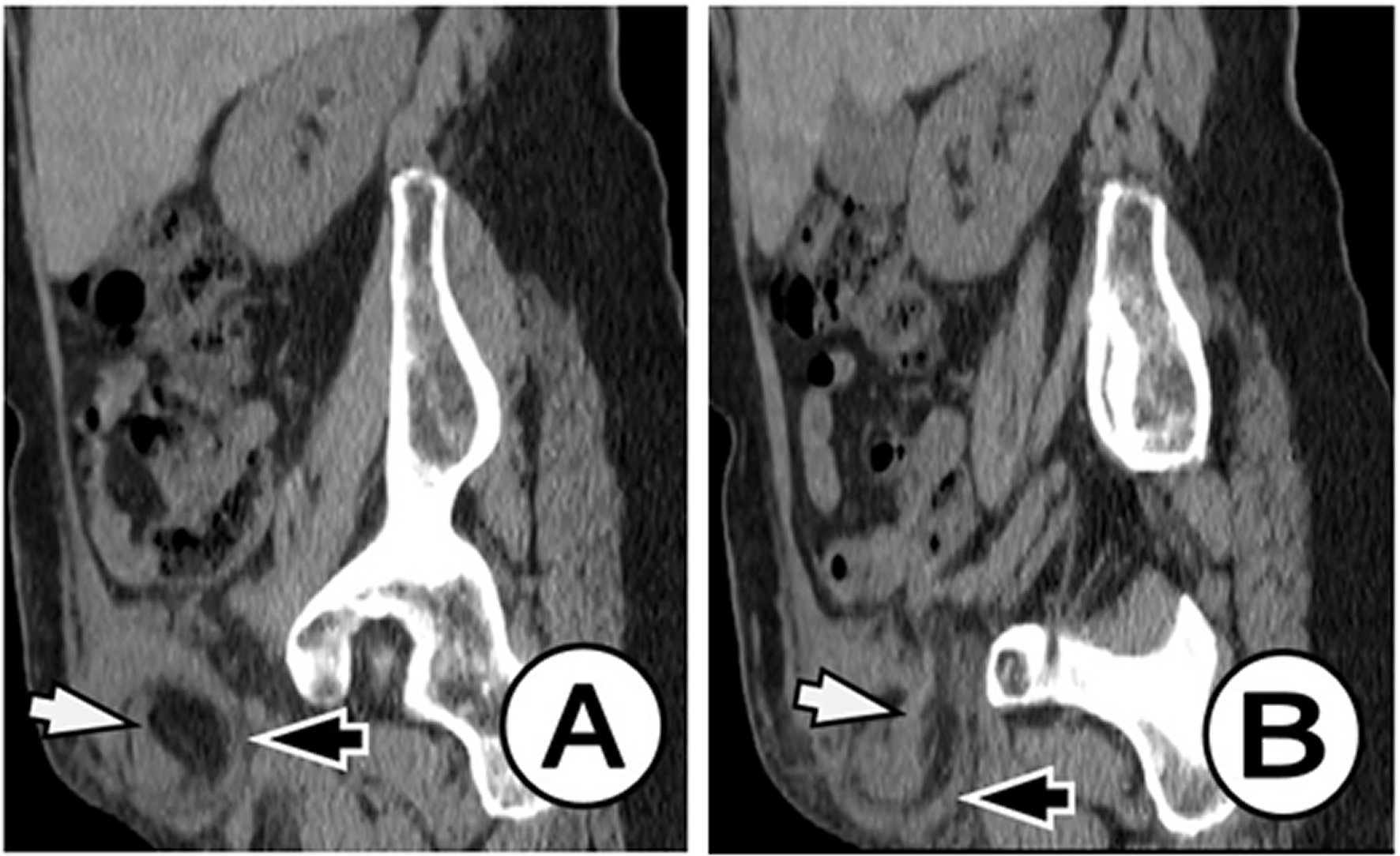
We present a rare case of a 69-year-old female patient with a history of intermittent pain in the right inguinal region which was examined at the emergency surgical clinic. On physical examination, the patient was an elderly woman who was not pale, afebrile, and she had a right-sided inguinal swelling and painful sensitivity. A routine lab test was performed and it showed an increase in WBC and CRP. After the clinical examination, a diagnosis of right inguinal hernia was made. She was sent to the Radiology Department for further evaluation, performing a CT scan of the abdomen and a small pelvis diagnosing inflamed appendix. The inflamed appendix was herniated in the inguinal hernia sac as observed in Figures 1 and 2. As a result, CT diagnosis of Amyand's hernia with acute appendicitis was established. Pathological changes in the parenchymal abdominal and retroperitoneal organs were not seen. Small bowel loops were free, without signs of ileus. Free fluid in the abdomen were not observed. The laparotomy was performed in which the inflamed appendix was removed, and the inguinal hernia was resolved. The patient was discharged on the seventh day after the operation in good general condition. Two control examinations were performed, the first fifteen days after the operation, and the second two months later, during which no complications were observed in the patient and he is in good general condition.
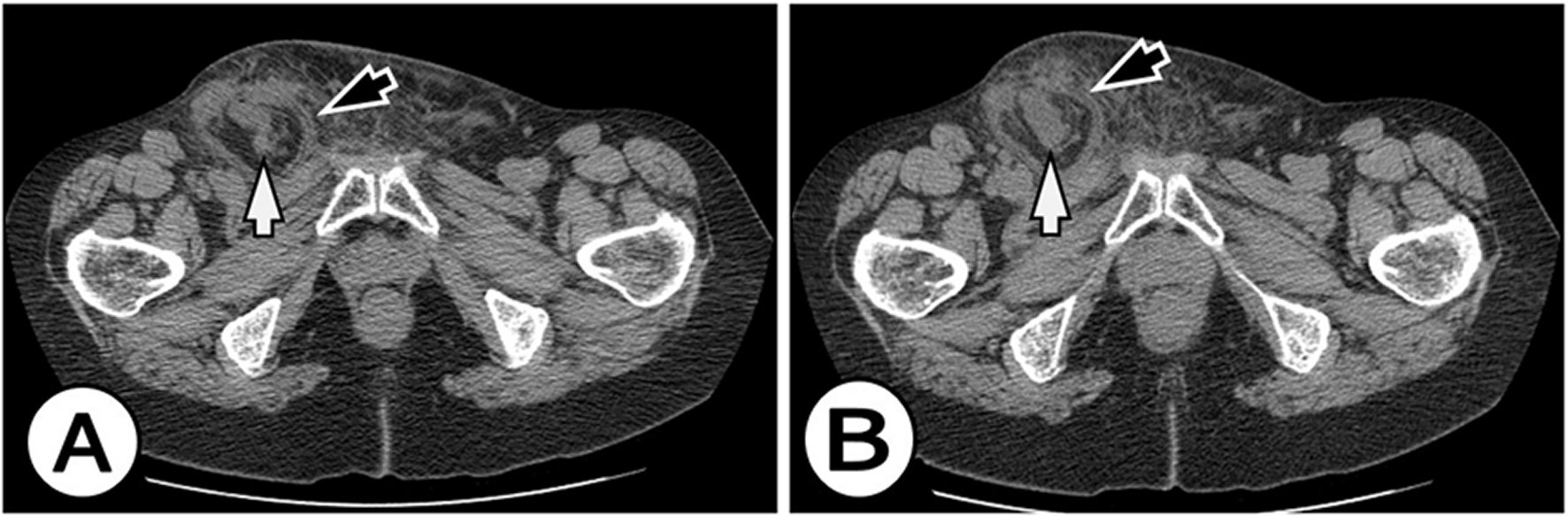
Figure 1. Axial CT scan at the level of inguinal regions shows an inflamed appendix (white arrow) extends into the small right inguinal hernia (black arrow). There were no signs of obstruction or strangulation.
DISCUSSION
An Amyand's hernia is a rare type of hernia, characterized by the presence of the appendix, either inflamed or normal, in the inguinal hernia sac. Claudius Amyand was the first who described and treated this condition in 1735 [12]. Amyand's hernia occurs more often in males than females in approximately 1% of all inguinal hernias [13]. The appendix may remain perfectly normal but if the diagnosis is a delay, it could become inflamed with subsequent perforation and abscess. Clinical signs and symptoms strongly depends on the situation of the vermiform appendix. Physical examination will usually reveal swelling in the right groin, pain, and tenderness [14]. Clinical symptoms can be misleading and more often resemble those of a strangulated inguinal hernia than the classic signs and symptoms of appendicitis [15]. Only imaging can verify the contents of an incarcerated inguinal hernia and the approach varies upon those findings. It is generally accepted that surgical treatment includes a hernia repair with or without concomitant appendectomy.
Ultrasound is an excellent technique to evaluate the inguinal region and used to detect all types of inguinal hernias, including Amyand's hernia. The US is the initial diagnostic modality of choice in the pediatric population [8]. The US is safe and cheap but remains operator-dependent. Computed tomography of the abdomen increases the specificity of detection and diagnostic accuracy of Amyand's hernia to almost 90% [14].
When diagnosis remains unclear, surgery can both be diagnostic and therapeutic. There is no standard protocol for the management of Amyand's hernia. Important determinants for appropriate surgery include the presence of an inflamed appendix, contamination of the surgical field, patient age, and anatomic features [16]. A normal appendix can be returned to the peritoneal cavity or appendectomy can be performed. Treatment depends on the surgeon's personal choice. Removing a healthy appendix is subject to a medical debate, which has not reached a consensus yet [17]. Hernioplasty without appendectomy is a favored option in patients with a normal appendix [10, 18]. In our case report, appendectomy with partial omentectomy followed by mesh repair is performed without any post-operative complications, with broad-spectrum antibiotic cover. In cases of appendicitis, perform appendectomy mast followed by herniorrhaphy [10, 16].
The decision to perform appendectomy and type of hernia repair depends on the intraoperative finding, guided by the Losanoff and Basson's criteria [19]. Appendectomy through the hernia orifice is reserve for Amyand's hernia types 1 and 2, while types 3 and 4 warrants an exploratory laparotomy due to the risk of peritoneal contamination.
In this case, the decision to proceed with an appendectomy followed by the mesh-free repair of Amyand's hernia is base on Losanoff and Bosson's criteria for Type 2 Amyand's hernia [19].
CONCLUSIONS
Amyand's hernia is rare and difficult to diagnose a condition, which represents a surgical emergency, commonly occasionally found in a diagnostic or surgical procedure. Computer tomography helps make an accurate and timely diagnosis of Amyand's hernia, thus avoiding complications from delayed surgery.

