










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Coronavirus disease 2019 (COVID-19) is a new infectious disease which generate the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), that spreading rapidly around the world [1]. Most people will develop mild to moderate respiratory illness but old age people or patients with special medical condition such as diabetes, chronic respiratory disease or cardiovascular disease may develop serious symptoms leading to death [2, 3]. This pandemic affected the world socially, economically and the health care system including the overload on medical facilities and hospitals as well as the medical staff who are at a high risk [4]. Therefore, the need of an effective way to control this pandemic is a must, such as hand washing, face mask, social distance or vaccine [5].
Typically, vaccines need years of research and testing before reaching the clinic, but in 2020 scientists tried to produce safe and effective SARS-CoV-2 vaccines in record time. As the last update in 12th August, 2021 researchers were testing 99 vaccines in clinical trials on human and 33 have reached the final stages of testing and more than 75 preclinical vaccines are under active investigation in animals [6].
The world first mass vaccination program started in December 2020 with at least 13 different vaccines [7]. SARS-CoV-2 vaccines have various categories such as inactivated virus vaccines, subunit vaccines, vector vaccines, and nucleic acid vaccines, with efficacy arranged from 50% up to 95%. The most common vaccine mechanism used around the world has been made from companies such as Pfizer/BioNtech Comirnaty and Moderna COVID-19 vaccine, which are mRNA-based vaccines with efficacy 95% and 94.5%, respectively, AstraZeneca/AZD1222 and Janssen/Ad26.COV2.S vaccines are Adenovirus Vector vaccine with efficacy 70% and 76.7-85.4%, respectively. Finally, the Sinopharm COVID-19 vaccine (BBIBP-CorV) and Sinovac-CoronaVac are Inactivated virus vaccine with efficacy of 79% and 50-91%, respectively [8, 9]. Two doses are needed for full vaccination from the most vaccines listed by World Health Organization (WHO) as Moderna and Pfizer-BioNTech., while in Johnson & Johnson's a single dose only is enough [7, 10].
A vaccine's efficacy is the performance in a controlled clinical trial, while vaccine effectiveness is a measure of how well vaccines work in the real world conditions [11], especially with some factors that may affect the effectiveness of the vaccine including clinical trial on specific people who may develop a different response to the vaccine or the mutations in the virus genome, or the correct storage and handling of the vaccine [12]. COVID-19 vaccines will not be 100% effective, but the evaluations observed a reduced number of infections the infection, critical cases and death from the SARS-CoV-2 infection [12, 13]. The aim of this study is to assess the correlation and the effectiveness of SARS-CoV-2 vaccine with COVID-19 disease outcome worldwide.
MATERIALS AND METHODS
The data on COVID-19 cases for 138 countries post vaccination on 17 August 2021 collected from Worldmeter website (www.worldmeter.info). The website listed numbers of cases, total cases, active cases, recovery cases, deaths cases and critical case. The data for pre-vaccination for 86 countries on 13 April 2020 collected previously from (www.worldmeter.info) which was previously published [14]. All the results were expressed in percentage from the total cases to avoid the increased number of infected people among the countries after more than one year of pandemic.
The percentage of vaccinated people data in each country was obtained from Statistics and Research Coronavirus (COVID-19) Vaccinations (https://ourworldindata.org/covid-vaccinations) [15]. Countries were divided into four groups: group 1 (0-24 %), group 2 (25-49%), group 3 (50-74) and group 4 (75-100%) of vaccination. In addition, 2 groups were defined: first is the full dose vaccination which is the percentage of vaccinated people received two doses and completed the vaccination program and second is the total dose vaccination which is the percentage of vaccinated people who completed the vaccination program plus people received single dose only. Three different types of SARS-CoV-2 vaccine mechanism was used in these study: mRNA, vector Adenovirus and inactivated virus, made from different companies such as Moderna, Johnson&Johnson, AstraZeneca, Pfzer/BioNTech, Sinopharm, Sinovac, Sputnik V, CanSino, Covaxin, and COVIran, among 138 countries. There was no country used the inactive virus, being the 138 countries divided into 6 groups: group 1 used the mRNA only, group 2 used adenovirus vector only, group3 used mRNA, adenovirus vector and inactive virus, group 4 used mRNA and adenovirus vector, group 5 used mRNA and inactive virus and group 6 used inactive virus and adenovirus vector, (https://ourworldindata.org/covid-vaccinations),
The statistical analyses were performed with SPSS software version 16.0. The Paired T-test was used for the comparison between COVID-19 disease outcome pre and post-vaccination. Spearman Correlation coefficient was used for the relationship between full and total SARS-CoV-2 vaccine with COVID-19 disease outcome. Receiver operating characteristic curve (ROC curve), Area Under the Curve (AUC) and Mann Whitney test were used to assess the sensitivity and specificity of the vaccine efficiency and the impact of vaccine on severity of COVID-19 dieses. Kruskal Wallis test was used to compare the percentage of vaccine distribution in four groups among countries with COVID-19 disease outcome. Countries without enough date were excluded from the statistical analysis.
RESULTS
The correlation between total and full SARS-CoV-2 vaccine with the percentage of COVID-19 cases outcome in 138 countries at 17 August 2021 were evaluated. The results showed a significant negative correlation of total vaccine with percentage of death from COVID-19 (rs = -0.345, p = 0.005), percentage of critical cases (rs = -0.201, p = 0.018) and was insignificant negative correlation with active cases (rs = -0.143, p = 0.095). However, a significantly positive correlation with recovered cases was observed (rs = 0.189, p = 0.027). Similar results were obtained with full vaccination, observing a significant negative correlation of full vaccine with percentage of death from COVID-19 (rs = -0.326, p = 0.0005), percentage of critical cases (rs= -0.278, p = 0.001) In addition, the results showed a significant negative correlation of full vaccination with active cases (rs = -0.208, p = 0.015) and significantly positive correlation with recovered cases (rs = 0.248, p = 0.003).
79 countries received less than the mean percentage of vaccinated people (28%) and 59 countries higher than the mean percentage of vaccinated people (28%). The mean percentage of vaccine was used to assess the significant impact of vaccine on the percentage of death, active, critical and recovery cases. There were a significantly higher number of deaths, active and critical cases rate in countries with less than 28% of vaccinated people compared with countries with more than 28% of vaccinated people (p = 0.0005, p = 0.041 and p = 0.003, respectively). The recovery cases rate was significantly higher in countries with more than 28% of vaccinated people compared with countries with less than 28% of vaccinated people (p = 0.009) (Table 1).
Table 1. The mean percentage of COVID-19 disease outcome among countries sorted by 28% of vaccination
Data is expressed as mean ± standard error.
Data from 36 countries of vaccine type distribution was available on (https://ourworldindata.org/covid-vaccinations) [15]. Therefore, the correlation between the distribution of SARS-CoV-2 vaccine types in these countries and severity of COVID-19 disease outcome assessed with spearman's correlation test and the results showed a significant negative correlation of mRNA vaccine type with percentage of death cases (rs = -0.345, p = 0.039) and insignificant negative correlation with percentage of recovery cases (rs = -0.181, p = 0.29). There was observed a significant positive correlation with percentage of active cases (rs = 0.332, p = 0.048) and insignificant correlation with percentage of critical cases (rs = 0.023, p = 0.89).
The correlation between vector adenovirus vaccine of SARS-CoV-2 with severity of COVID-19 disease outcome among 36 countries revealed an insignificant negative correlation with percentage of death cases (rs = -0.132, p = 0.44), and with percentage of recovery cases (rs = -0.035, p = 0.83). However, it was observed an insignificant positive correlation with percentage of active cases (rs = 0.092, p = 0.59) and with percentage of critical cases (rs = 0.034, p = 0.84). The correlation between SARS-CoV-2 inactivated virus vaccine with severity of COVID-19 disease outcome among 36 countries showed an insignificant positive correlation with percentage of death cases (rs = 0.321, p = 0.056), percentage of recovery cases (rs = 0.218, p = 0.201) and with percentage of critical cases (rs = 0.32, p = 0.85). Nevertheless, an insignificant negative correlation with percentage of active cases was observed (rs = -0.313, p = 0.063).
The mean percentage of death cases (1.4%) and percentage of recovery cases (91%) from Table 1 was used to classify the countries into two groups to assess the sensitivity and specificity of vaccine. The AUC results from ROC curve for percentage of recovery cases accepted (area = 0.643, 95% CI 0.550 - 0.735, p = 0.004) and the cut-off 19.5% of vaccination or higher significantly increased the recovery rate (Figure 1). However, it was poorly accepted AUC results for death cases (area = 0.593, 95% CI 0.497 - 0.689, p = 0.06) and the cut-off 23.5% of vaccination and higher needed to decrease the percentage of death cases (Figure 2).
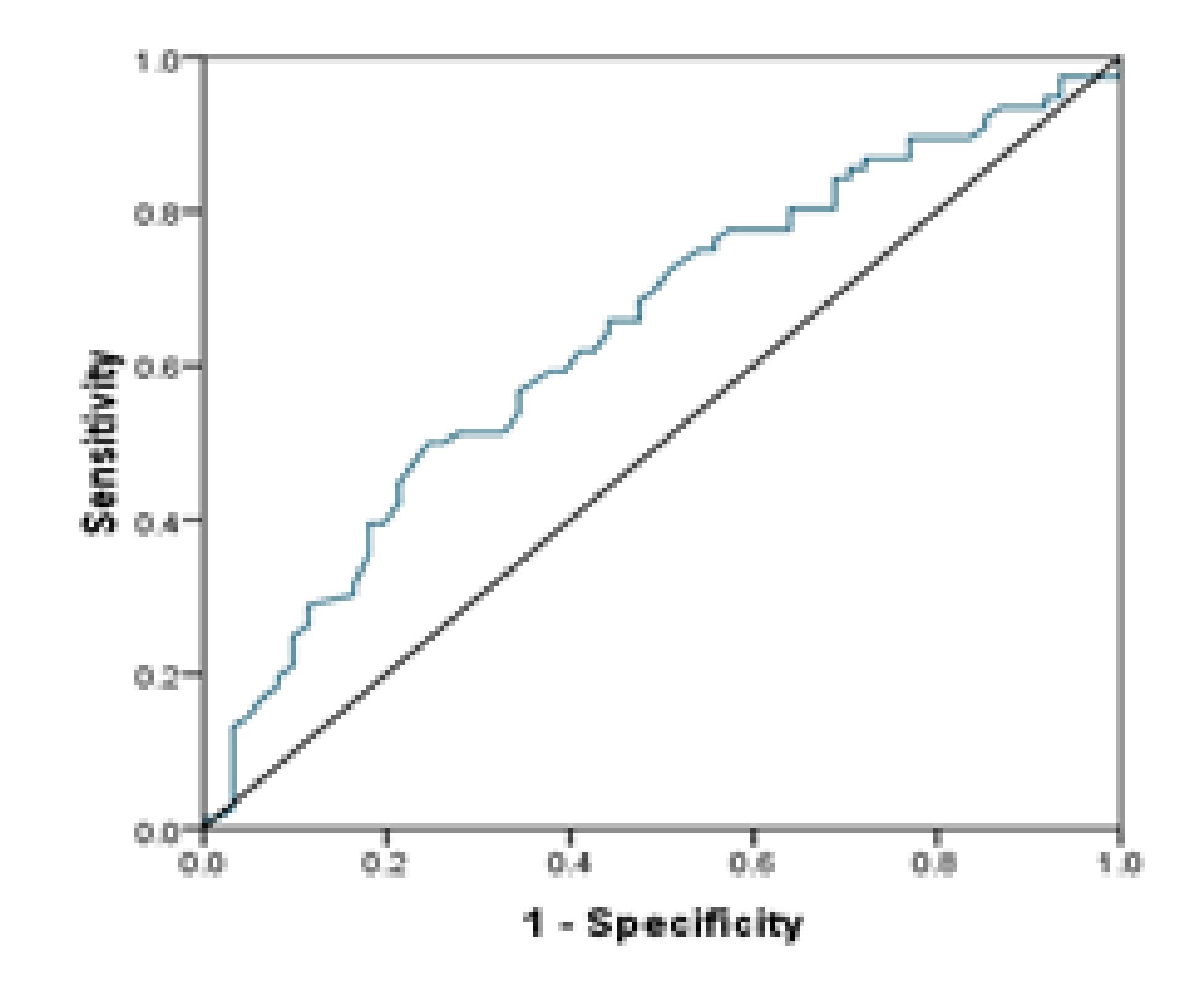
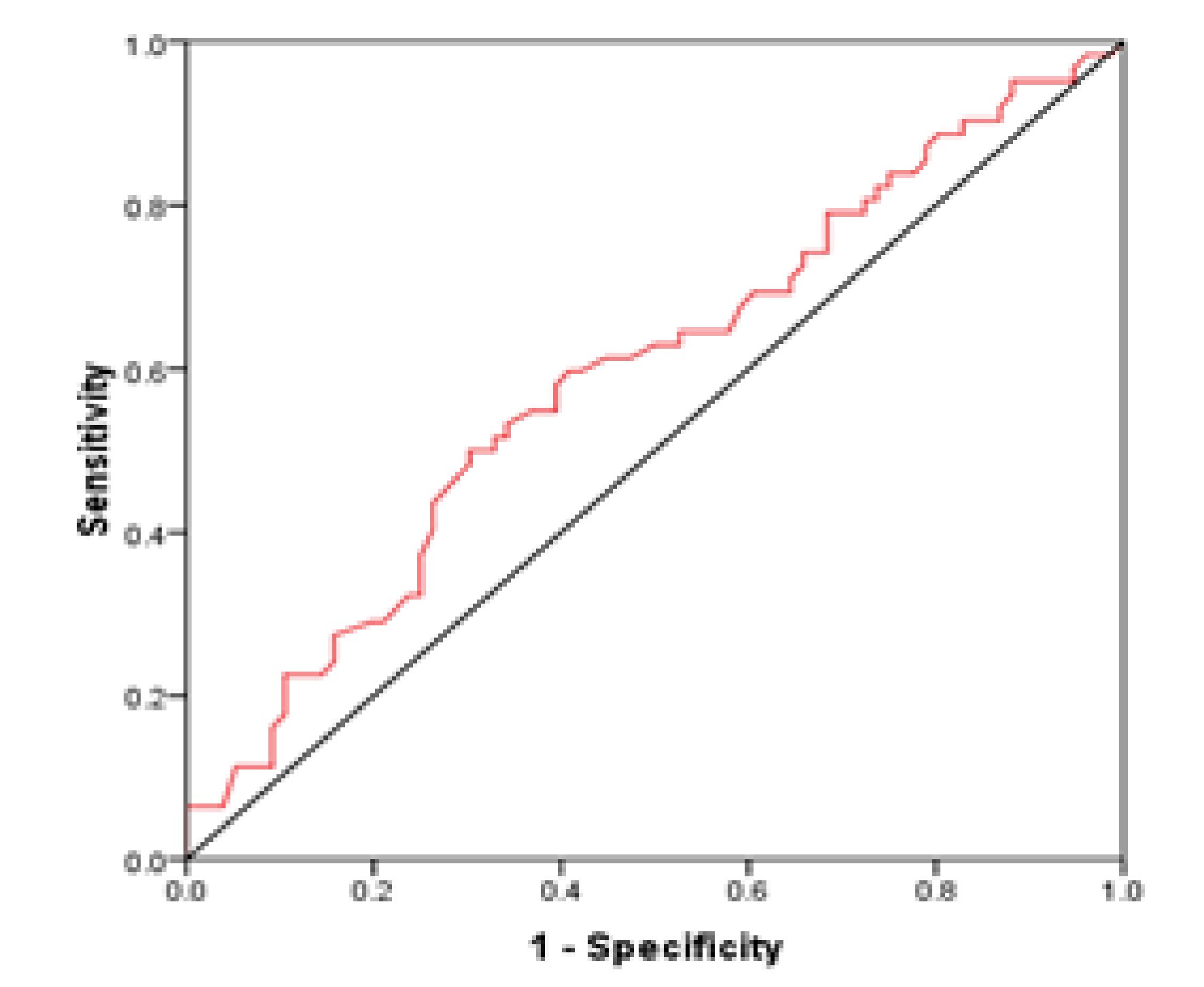
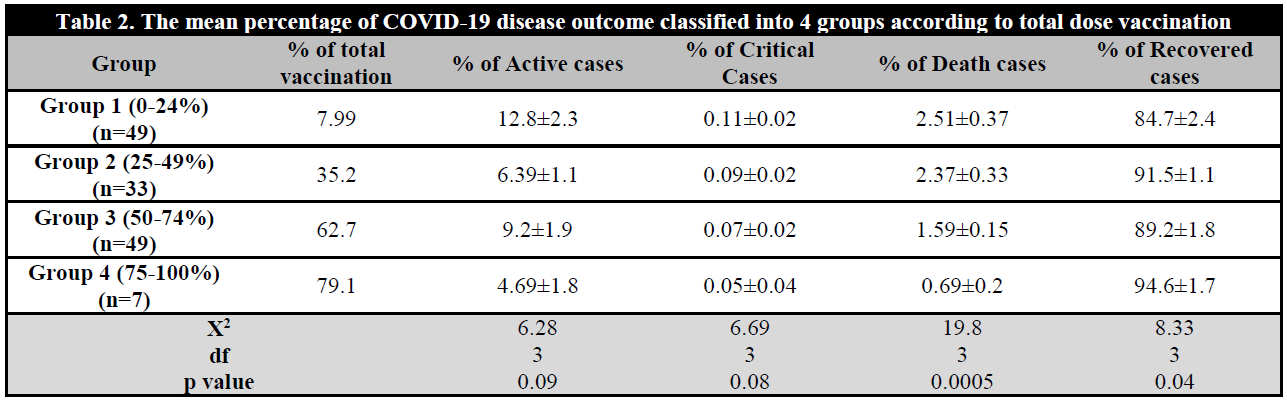
Table 2 illustrates the mean percentage of each four groups distribution by percentage of total vaccine group 1 (0-24%), group 2 (25-49%), group 3 (50-74%) and group 4 (75-100%). There were observed significant differences in death cases among countries in 4 groups. The countries with higher percentage of total vaccine showed the lowest percentage of death cases rate (χ2(3) = 19.8, p = 0.0005), but insignificant with percentage of critical cases (χ2(3) = 6.69, p = 0.08) and active cases (χ2(3) = 6.28, p = 0.09). However, there were observed significant differences in percentage of recovered cases, showing the group 4 the higher recovered rate followed by group 2, group 3 and lowest with group 1 (χ2(3) = 8.33, p = 0.04) (Table 2).
Table 2. The mean percentage of COVID-19 disease outcome classified into 4 groups according to total dose vaccination
Data is expressed as mean ± standard error.
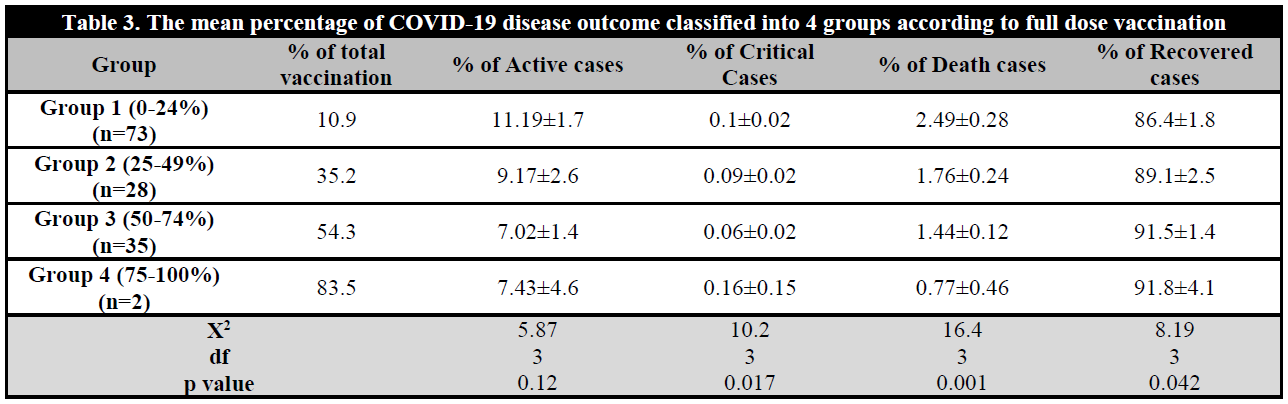
The mean percentage of 4 groups distributed by the percentage of full dose vaccine among countries may be observed in Figures 3 and 4. The results showed a significant difference in death caused by COVID-19. The countries with higher percentage of full vaccine showed a significantly lowest percentage of death cases (χ2(3) = 16.4, p = 0.001), and percentage of critical cases (χ2(3) = 10.2, p = 0.017) compared with other groups. However, no statistical significant differentes were observed attending to active cases (χ2(3) = 5.87, p = 0.12). The recovered rate was significantly higher in countries of group 4 compared with the other groups (χ2(3) = 8.19, p = 0.04) (Table 3). Figures 5 and 6 show the percentage of death cases distribution before the vaccine program and post-vaccination programme, respectively.
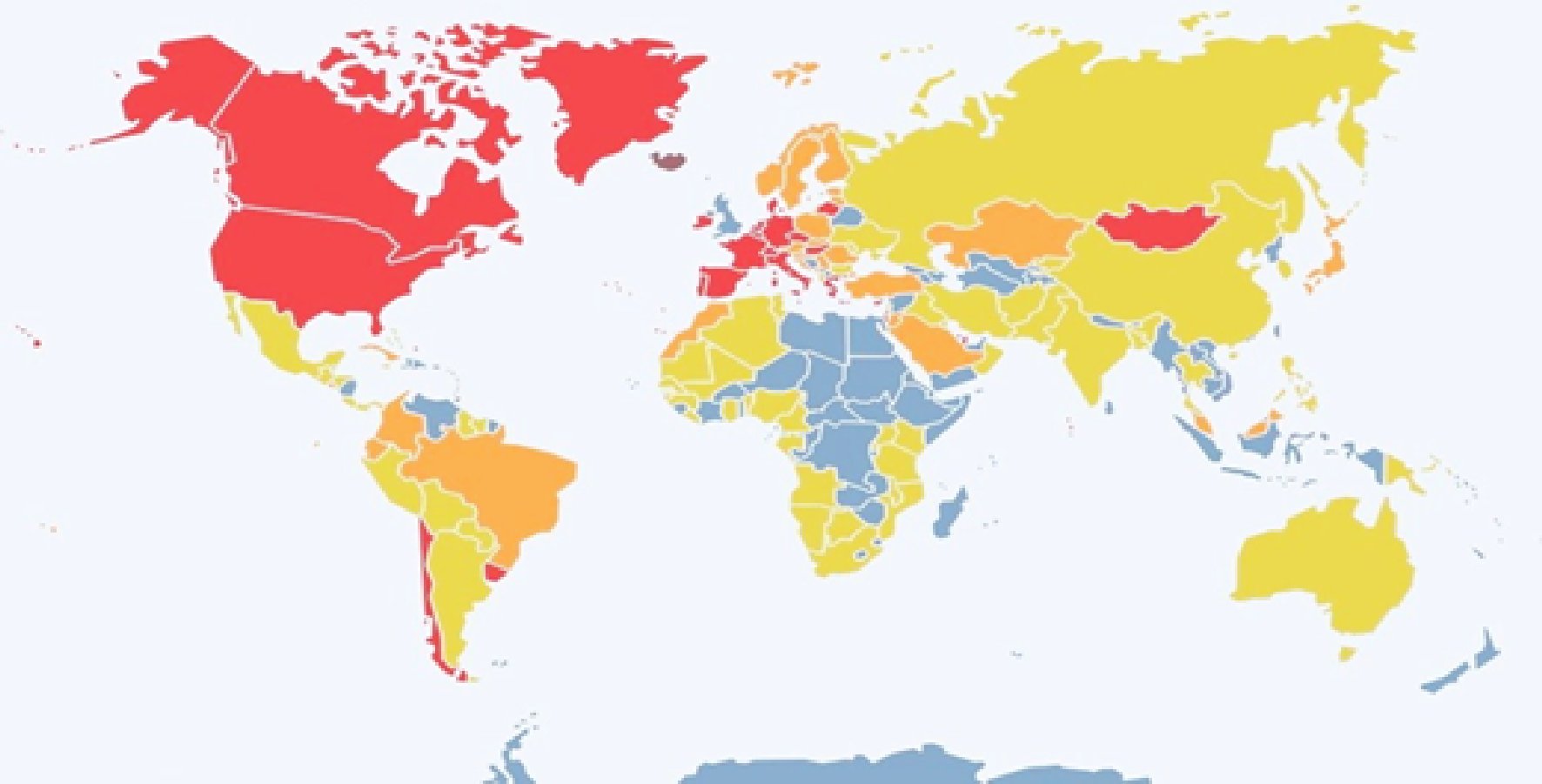
Figure 3. Distribution of full dose vaccination among countries.= No data; = 0-24%; = 25-49%; = 50-74 %; = 75-100%).
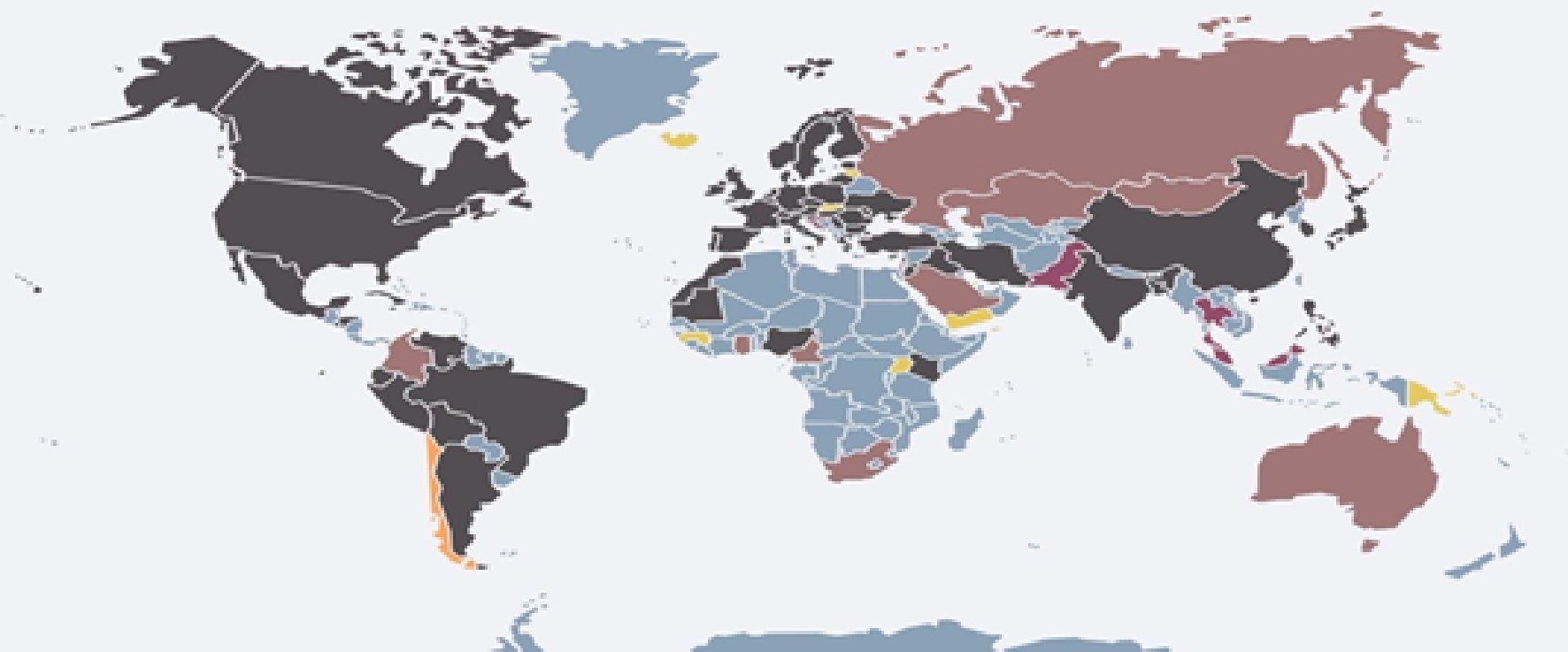
Figure 4. Distribution of pre-vaccinate death cases among countries.= No data; = 0-0.75%, = 0.76-1.43%; = 1.44-1.76%; = higher than 1.77%.
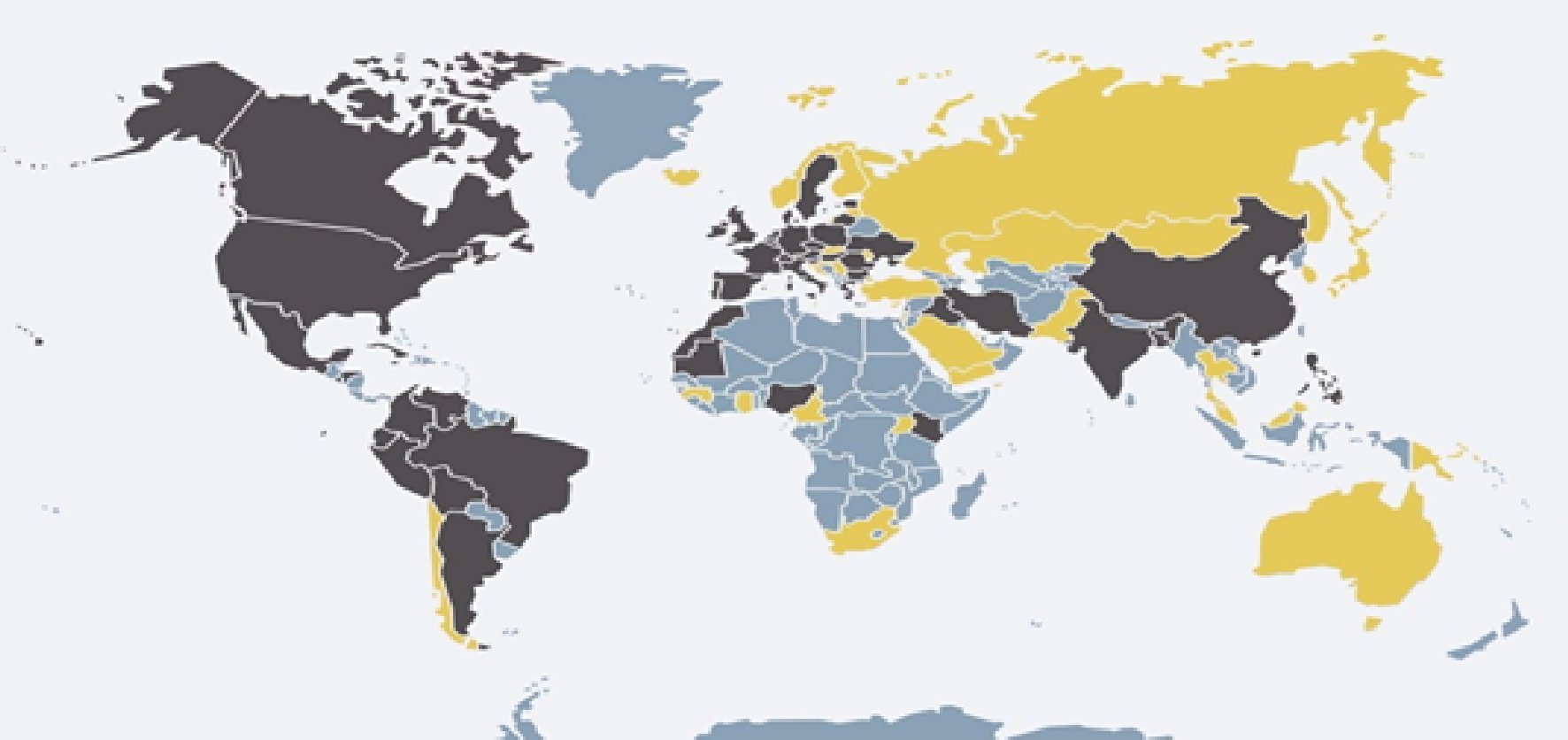
Figure 5. Percentage of death cases distribution before the vaccine program.= No data; = 0-2.2 %; = higher than 2.2%.
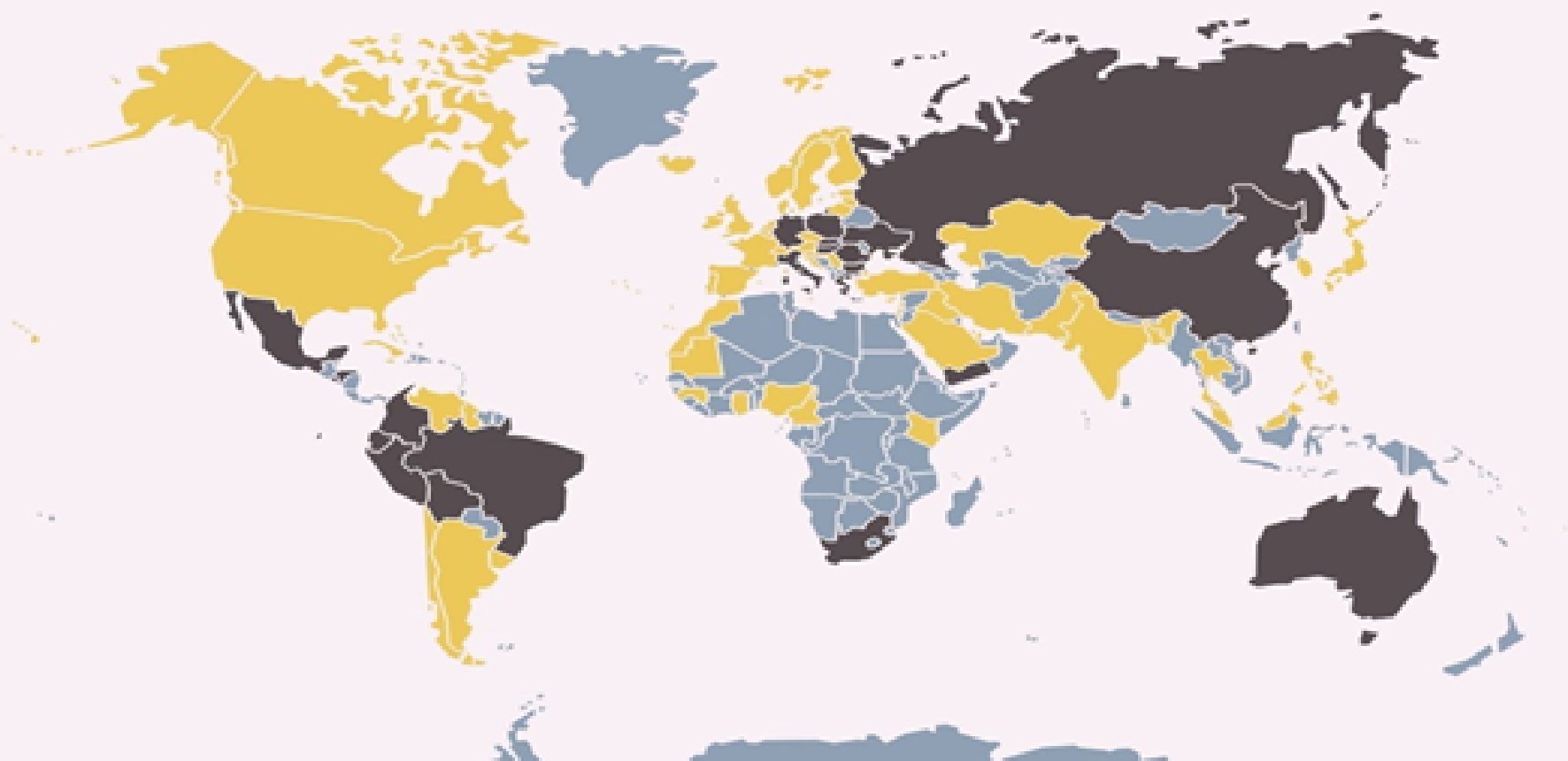
Figure 6. The impact of full dose vaccination on the percentage of death cases according to mean percentage of post-vaccination.= No data; = 0-2.2%; = higher than 2.2%.
Table 3. The mean percentage of COVID-19 disease outcome classified into 4 groups according to full dose vaccination
The paired T-Test was used to compare the COVID-19 disease outcomes in 85 countries before the SARS-CoV-2 vaccine programme started (pre-vaccination programme) and after its initiation (post-vaccination). The results showed a significant decrease in mean percentage of death cases of post-vaccination patients (mean = 2.25, SD = 2.39) compared with pre-vaccination subjects (mean = 3.85, SD = 3.56); (t (85) = -3.59, p = 0.001). A significant decrease in critical cases rate in post-vaccination (mean = 0.08, SD = 0.11) compared with pre-vaccination (mean= 1.87, SD = 1.71); t(81) = -9.41, p = 0.0005) was also observed. Similar results were observed with active cases rate, observing statistically differences in the post-vaccination group (mean = 8.78, SD = 11.87) compared with the mean percentage of pre-vaccination (mean = 75.2, SD = 20.5); t (84) = -27.19, p = 0.0005). Finally, the recovered cases rate in post-vaccination subjects (mean = 89.05, SD =12.15) was significantly increased compared with post-vaccination patients (mean = 20.55, SD =20.22); (t (84) = 28.4, p= 0.0005) (Table 4).
Table 4. The mean percentage of COVID-19 disease outcome of pre and post-vaccination among countries
Data is expressed as mean ± standard error.
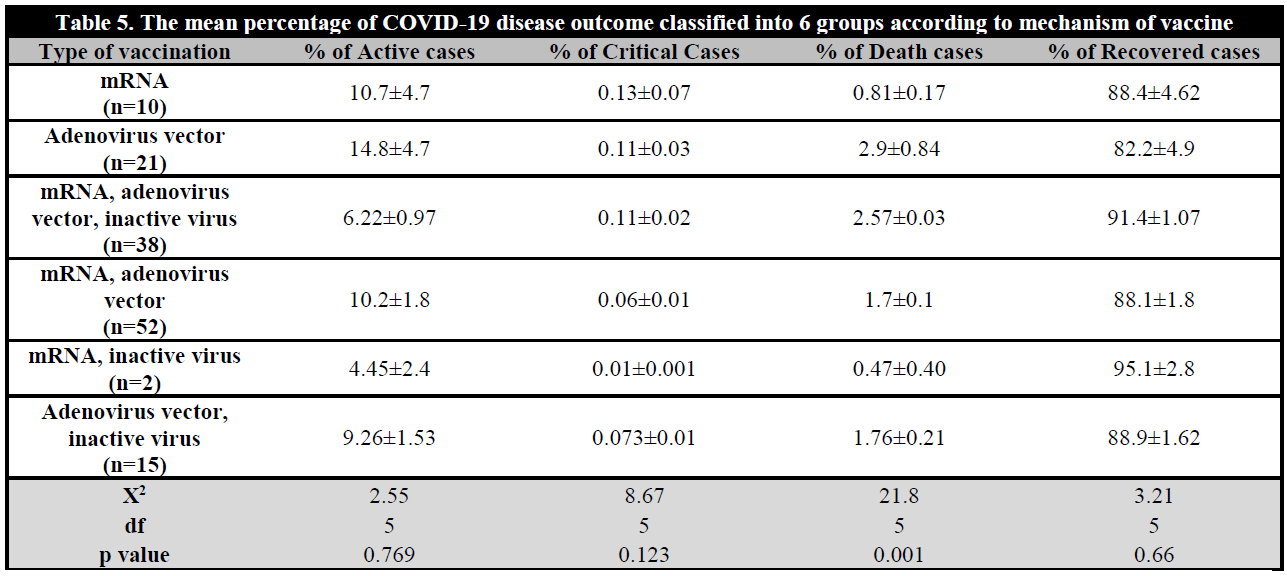
The comparison of vaccine types assessed among 6 groups of countries was also evaluated. The results showed a significantly higher rate of death cases due to COVID-19 in countries used group 2 SARS-CoV-2 vaccine (Adenovirus vector only) followed by group 3 (mRNA, Adenovirus vector and Inactive virus), group 1 (mRNA only), group 6 (Adenovirus vector and Inactive virus), group 4 (mRNA and Adenovirus vector). The lowest percentage of death cases with group 5 (mRNA and inactive virus) countries (χ2(5) = 21.3, p = 0.001). No statistically significant results were observed in the percentage of critical cases (χ2(5) = 8.75, p = 0.11), active cases (χ2(5) = 2.38, p = 0.79) and recovered cases (χ2(5) = 3.4, p = 0.63) (Table 5).
DISCUSSION
By 28 February 2021 COVID-19 pandemic caused 2.5 million deaths worldwide and there have been over 110 million infected cases [16], leading to negative impact on economy and social life. Therefore, the need of an effective vaccine increased to prevent further mortality and morbidity [4]. This study was designed to assess the effectiveness of coronavirus vaccine worldwide and showed that countries with high percentage of vaccinated people have significantly lower percentage of death and critical cases among SARS-CoV-2 infected people and significantly higher percentage of recovered cases from the infected cases in total and full dose vaccination, although the countries with higher rate of full dose vaccination correlated significantly more with COVID-19 outcome when compared with total dose vaccinated countries. This study supports previous findings of COVID-19 vaccine's effectiveness against symptomatic infection by decreased mortality rate, severity of disease and effectively prevent hospitalization, while other studies showed that one dose of vaccination was less effective on COVID-19 disease outcome [17, 18, 19, 20].
The SARS-CoV-2 vaccine effectiveness was supported classifying countries into groups according to percentage of full dose vaccinated people. First group was classified according to the mean percentage of full dose vaccination. The countries with a vaccination rate higher than 28% of people have significantly lower rates of death, active and critical cases and significantly higher recovered cases compared with countries with a vaccination rate lower than 28%. The second group classified countries into four groups according to percentage of vaccine received in their population. The results indicated that countries with more than 75% of total and full dose vaccination have lower percentage of death followed by countries with less than 74%, less than 49% and countries less than 24%. In addition, countries with more than 75% of total and full dose vaccination have higher percentage of recovered cases than other countries. Moreover, countries with higher percentage of full dose vaccinated people showed decreased rates of critical cases.
More evidence of the impact and effectiveness of COVID-19 vaccine came from the comparison of COVID-19 disease outcomes before these countries started the vaccination program at 13th April 2020 with COVID-19 disease outcomes after vaccination program for the same countries at 17th August 2021. There was observed a significant decreased rate in death and critical cases and significantly increased rate in recovered cases. These results indicate that the vaccination program campaign made a good effect on the countries by reducing the critical cases and death. However, we cannot ignore the difference in adherence to COVID-19 prevention measures among countries [21, 22, 23], as well as differences in the stringency of measures over time and across geographical regions [23]. In addition, the way of the population on how to protect themselves from the SARS-CoV-2 infection by some simple precautions such as wearing mask, hand hygiene and social distance [5]. However, all these precautions do not affect to recovery and death rates from COVID-19 once they got infected with the virus. Therefore, the sensitivity and specificity of vaccine impact for more than 23.5% of people vaccination against SARS-CoV-2 needed to decrease percentage of death and increase recovery rate, some vaccines showed to prevent infection and disease, while others prevent disease but not infection [23]. The SARS-CoV-2 vaccine will not prevent infection but decrease death rate, hospitalization and increase recovery rate.
Different types of SARS-CoV-2 vaccine mechanisms used worldwide including mRNA vaccines, inactivated vaccines and vector adenovirus vaccines. There were insignificant differences between types of vaccine used in these countries for active, critical and recovery cases, while the study indicated that countries using both mRNA and inactivated virus vaccine has significantly lower percentage of death cases and countries compared to countries which used only vector SARS-CoV-2 vaccine. These results may be due to the few number of countries using adenovirus vector vaccine alone. Previous studies showed that the effectiveness of adenovirus vector from AstraZeneca vaccine was 79% in preventing symptomatic COVID-19 [25].
The distribution rate of vaccine type in each country showed that countries which used more mRNA vaccine have significantly less death cases by SARS-CoV-2 virus. This observation supports the effectiveness observed of mRNA vaccine (Pfizer/BioNtech Comirnaty and the Moderna vaccine) (91-94%) preventing symptomatic COVID-19 disease [26, 27]. The mRNA vaccine effectiveness against COVID-19 hospitalization was higher than the adenovirus vector vaccine [28]. Other studies showed that mRNA vaccines have 79% of effectiveness against confirmed infection with Alpha and Gamma SARS-CoV-2 variant and 84% to 88% effectiveness against symptomatic infection caused by Gamma and Beta [17, 29], while adenovirus vector vaccine showed to be 71% effective against Delta variant hospitalization and 67% with Beta variant [30].
CONCLUSIONS
This study indicated that different vaccine mechanism against SARS-CoV-2 virus of more than 23.5% of vaccination people with full dose vaccine is effective to decrease death and serious symptoms of COVID-19 disease. In addition, this ratio also increases the recovery rate. However, due to the SARS-CoV-2 variant and genetic susceptibility, we recommend each country to compare the effect of each vaccine mechanism type among COVID-19 cases received full vaccine. In addition, future studies are needed to assess the effect of single dose vaccine in COVID-19 disease outcome and to determine if the vaccine will accelerate the period of recovery rate and reduce the infectious period in each country.

