










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
In the early 1990s, Hiraku Sato was the first to characterize Takotsubo cardiomyopathy (TM) or stress cardiomyopathy (SC) as a condition that mimicked acute myocardial infarction (AMI). The ventriculogram of the heart resembles the shape of Japanese octopus trap, raising the name of Takotsubo syndrome [1].
It is a reversible cause of acute heart failure and has a clinical appearance similar to AMI with normal coronary arteries on angiography. The basal segments of the ventriculogram typically exhibit hypercontractility along with changes in apical contractility and its trigger is frequently physical or emotional stress [1, 2].
There have been several case reports of TM linked to thyroid conditions. However, there is no definite proof of a causal connection [1].
We present a case of TM in a patient with an impending thyroid storm due to Graves' disease.
CASE REPORT
In 2022, a 45-year-old woman with no known underlying diseases was referred due to sudden oppressive chest pain lasting for 3 hours associated with nausea and dyspnea at rest. Physical examination with a normal state of consciousness, heart rate 71bpm, blood pressure of 110/50 mmHg, cardiopulmonary auscultation revealed an S3 gallop and bibasilar rales. There was no jugular vein engorgement, and the other findings were unremarkable.
A chest X-ray was performed showing enlargement of the cardiac silhouette and bilateral interstitial infiltrates consistent with stage 2 acute pulmonary edema (Figure 1).
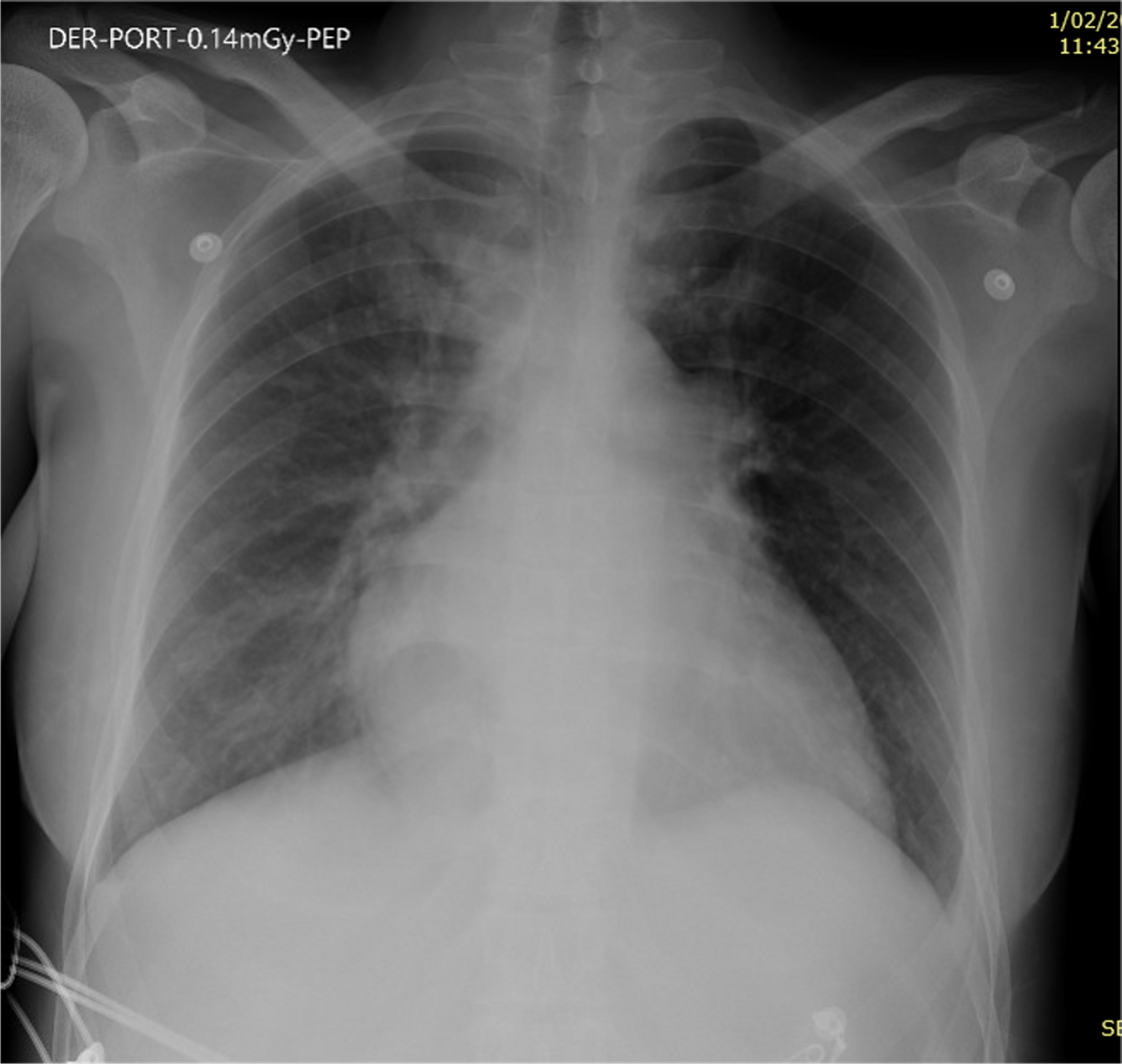
Figure 1. Chest X-ray shows enlargement of the cardiac silhouette and bilateral interstitial infiltrates.
The electrocardiogram (ECG) revealed upsloping ST segment depression with prominent and symmetrical T waves in the precordial leads and reciprocal ST segment elevation in aVR compatible with “winter ECG pattern” (Figure 2).
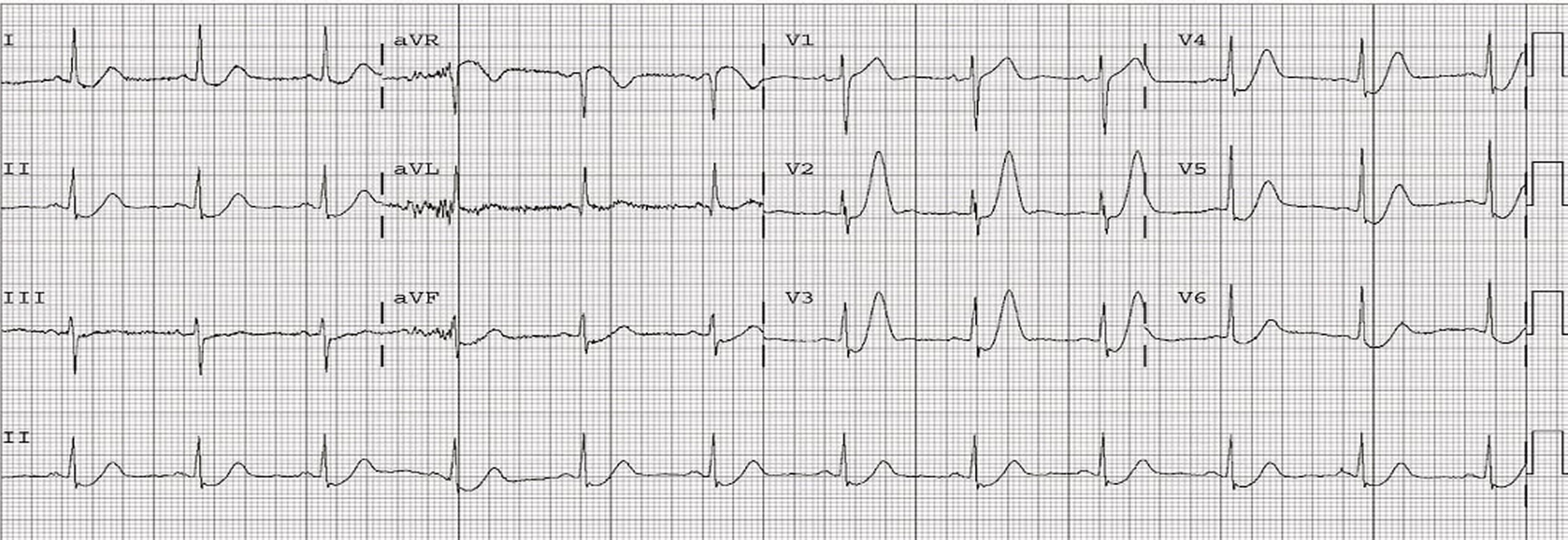
Figure 2. 12-lead ECG showed upsloping ST segment depression with prominent and symmetrical T waves in the precordial leads and reciprocal ST segment elevation in aVR.
Hemogram, plasma creatinine, urea and electrolytes tests were normal and troponin I was 0.15 ng/ml [Normal value (NV): less than 0.06 ng/ml].
Coronary angiography was done due to the initial suspicion of acute coronary syndrome (ACS) and the results showed that the coronary tree was free of lesionsand ventriculography revealed significant ventricular dysfunction, with hypercontractility of the most basal segments and akinesia of distal ones, consistent with Takotsubo syndrome (Figure 3). These findings were also found in the Doppler echocardiogram.
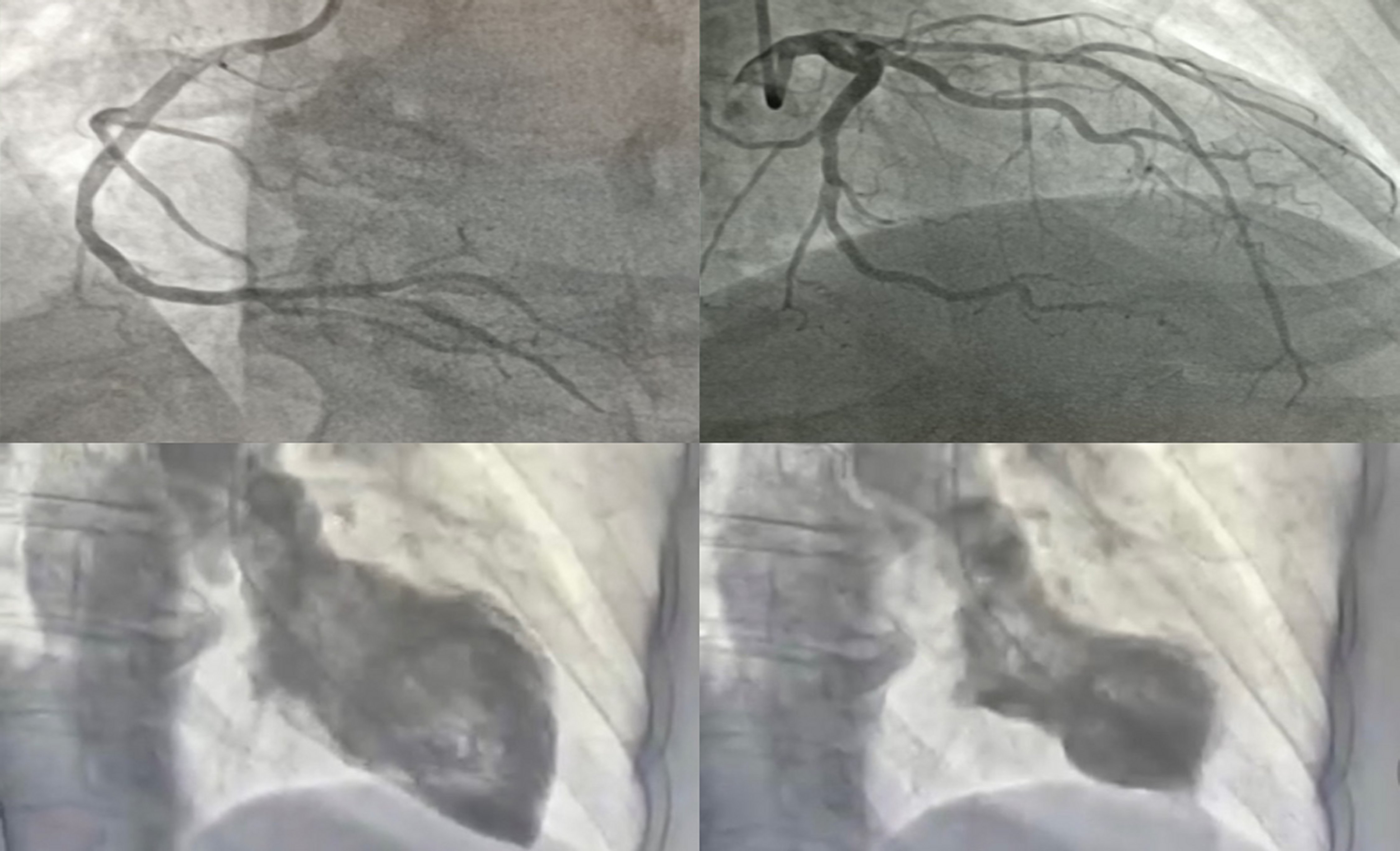
Figure 3. Coronary angiography without significant lesions and ventriculography image of apical ballooning.
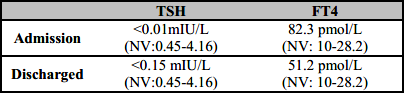
The patient was interrogated again and mentioned symptoms such as tremors, agitation, palpitations, and diarrhea throughout the previous three weeks. Thyroid function test revealed a free thyroxine 4 (FT4) value of 82.3 pmol/L (NV: 10-28.2), thyroid stimulating hormone (TSH) <0.01 mIU/L (NV 0.45-4.16), TSH receptor antibody (TRAb) 9.2 IU/L (NV<3.5) and the thyroid echography showed moderate enlargement of the thyroid gland, without nodules; being consistent with Graves' disease diagnosis.
The Burch-Wartofsky point scale (BWPS) indicated an imminent thyroid storm; therefore, antithyroid medication (Methimazole 10 mg every 8 hours) and beta blockers (Propranolol 40 mg every 6 hours) were initiated with positive clinical and analytical progress (Table 1).
A cardiac magnetic resonance (CMR) was performed on the patient six days after admission, and the results showed that the left ventricular function and contractility abnormality had returned to normal.
The patient was discharged with outpatient follow-up by cardiology and endocrinology teams.
DISCUSSION
Stress cardiomyopathy occurs in 1-2% of patients presenting with troponin-positive suspected acute coronary syndrome. The most typical form of this disorder is a hypokinetic or akinetic mid and apical segments with hyperkinesis of the basal walls of the left ventricle [3]. However there have been described a few additional takotsubo types, such as right ventricular, biventricular, midventricular, and basal (Takotsubo inverted) [4].
According to the International Takotsubo Registry, the mean age of stress cardiomyopathy patients was 66.4 years, and 89.9% of them were female. It is yet unknown why postmenopausal women are more susceptible [5].
Despite the fact that the exact cause of this syndrome is unclear, several theories have been proposed. One of these is microvascular spasm or dysfunction and direct myocardial toxicity due to catecholamine excess [6]. Therefore, clinically, and physiologically, hyperthyroidism can resemble a hyperadrenergic condition and cause similar changes. Through the upregulation of beta-adrenergic receptors, thyroid hormones exert both direct and indirect effects on cardiomyocytes, resulting in an increased chronotropic and inotropic response to normal levels of catecholamines [7].
Limited information is available on the risk factors for stress cardiomyopathy, and the development of the condition is frequently but not always associated with an extreme emotional or physical stress [8]. There have been reports of familial cases, raising the idea of a genetic susceptibility [9], and a potential correlation between serotonin norepinephrine reuptake inhibitors (SNRIs) and stress cardiomyopathy, but a causative relationship has not been proved [10].
The most common symptom of stress cardiomyopathy is acute substernal chest pain, which is similar to an acute coronary syndrome; however, some patients may experience dyspnea or syncope. ST segment elevation is a frequent ECG finding, typically in the anterior precordial leads; ST depression, QT interval prolongation, T wave inversion, aberrant Q waves, and non-specific abnormalities are other less frequent findings. Serum cardiac troponin and natriuretic peptides levels are elevated in most patients with stress cardiomyopathy [5].
The proposed Mayo Criteria for the Clinical Diagnosis of the Transient Left Ventricular Apical Ballooning Syndrome include: a) transient akinesis or dyskinesis of the left ventricular apical and mid-ventricular segments with regional wall-motion abnormalities extending beyond a single epicardial vascular distribution; b) absence of obstructive coronary disease or angiographic evidence of acute plaque rupture, new electrocardiographic abnormalities (either ST-segment elevation or T-wave inversion); and c) absence of recent significant head trauma, intracranial bleeding, Pheochromocytoma, obstructive epicardial coronary artery disease, Myocarditis and hypertrophic cardiomyopathy. These all criteria must be present [11].
Cardiac magnetic resonance may be useful in the diagnosis and evaluation of stress cardiomyopathy. In TM, the CMR may reveal a single mid-wall or subepicardial pattern of late gadolinium enhancement (LGE), but in AMI, LGE is either subendocardial or transmural [12].
In the absence of severe coronary artery disease, ST segment abnormalities have been related to a range of syndromes besides stress cardiomyopathy, such as myocarditis, coronary spasm and ACS associated to cocaine addiction. In addition, Similar reversible cardiomyopathy with global or focal dysfunction has been seen in individuals with severe brain damage and pheochromocytoma [13, 14].
Although most people with stress cardiomyopathy recover, the risk of serious complications are similar to those with acute coronary syndrome [5], and patients who survive the acute episode typically recover systolic ventricular function within one to four weeks [15].
CONCLUSIONS
This case shows that the most obvious diagnosis is not always the right one. Although TM is regarded as a rare cardiac disease, this condition it has been diagnosed more frequently. It may be preceded by a traumatic or upsetting experience, and it is typically associated with a positive prognosis. We propose the measurement of thyroid hormones when this entity is suspected; considering that, similar cases have been reported in the literature with clinical improvement with the standard antithyroid therapies. If thyroid disorders are identified, the management by the endocrinologist team will be necessary for cardiomyopathy resolution.

