










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
The so-called "memory wars" controversy (Loftus, 2004) surrounding dissociative amnesia within forensic contexts has been closed for some time (Freyd et al., 2010; Lindblom & Gray, 2010; Loftus, 1993; Loftus & Ketcham, 1996). However, it has recently resurfaced and reopened an interesting discussion (Brand et al., 2017a, 2017b, 2018; Patihis et al., 2021; Merckelbach & Patihis, 2018; Patihis et al., 2019) with special impact on forensic contexts.
The acceptance of repressed and later recovered memories phenomenon (i.e., dissociative amnesia or repressed memories) can lead to judicial errors in the form of bad practices when attempting to elicit memories of events that had not taken place (Arce et al., 2023; Loftus, 2004). Accepting dissociative amnesia should not be limited to whether the courts accept this phenomenon (Patihis et al., 2019), as courts are not the space for psychological theorizing, and theoretical ambiguities are inadmissible. In fact, the phenomenon of repressed memories or dissociative amnesias is not currently admissible in court as it fails to meet the criteria established in Daubert vs. Merrell Dow Pharmaceuticals, Inc. (1993).
The persistence of false dissociative amnesias can be attributed to several factors. Firstly, the confusion between clinical psychology and forensic psychology leads to a misunderstanding of the diagnosis and treatment of dissociative amnesia. Secondly, the inadequate definition of amnesia obscures the understanding of the phenomenon. Lastly, inherent difficulties in researching traumatic memories pose challenges to understanding the true nature of dissociative amnesia. The discord and misinformation generated among professionals due to the lack of consensus on the scientific evidence is worrisome.
This article proposes the Continuous Memory Accessibility Model. The model represents the variabilities in access to autobiographical memories depending on the causes of different memory conditions. This model poses an alternative to resolve the discussions around dissociative amnesias in the forensic context.
Clinical vs. Forensic Psychology
Clinical and forensic psychology are distinct fields with different objectives, methods, and requirements (Greenberg & Shuman, 1997). While dissociative amnesia may be relevant in the psychotherapeutic context, it cannot be accepted uncritically in forensic psychology. In forensic psychology, scientific support and theoretical agreement are particularly relevant as the underlying reality of the alleged event is crucial.
One of the main reasons the assumption of dissociative amnesia persists is its acceptance in a therapeutic context. Most memory experts deem the repression of traumatic memories implausible and the possibility of remembering them in a therapeutic context. Despite this, many professionals, students, and the general public continue to hold onto this belief (Patihis et al., 2021).
In the psychotherapeutic space, patients may, for example, report that they cannot leave the house due to a past attack or use the excuse of not remembering traumatic events to avoid talking about them. In this case, the therapist's main concern is the patient's subjective experience and mental health in the present moment, beyond the event's occurrence and the memory's accuracy. When a patient reports an inability to remember certain events, the therapist does not necessarily question the accuracy of the patient's memory unless it assists the therapeutic process. By contrast, in forensic contexts, the primary goal is to determine the factual accuracy of the person's statements, and, therefore, the truthfulness of recollection gains significance and requires more rigorous assessment.
From a survival perspective, it is not helpful to forget traumatic experiences, even though they may be painful. When working with victims of natural disasters or wars, it is common to find cases where people claim not to remember their traumatic experiences. However, research suggests that the real problem is that they want to forget but cannot (Manzanero et al., 2020). In a study of memories of sexual assault, Porter and Birt (2001) found that traumatic memories tend to be recalled more frequently than other autobiographical memories. Human memory processes emotionally significant information and events distinctively, leading to traumatic memories taking priority over others. In cases where these events have been forgotten, it is more likely due to a deliberate attempt to suppress the memory than to repressed or dissociated amnesia. Memories of traumatic events are likelier to create a flashbulb memory (Brown & Kulik, 1977) rather than amnesia (Hirst et al., 2015).
Amnesia vs. Poor Memory
Another element that generates debate in dissociative amnesia is the poor definition of what is meant by amnesia. Amnesia, which implies a total lack of memory, is confused with bad memory, but remembering poorly is not the same as remembering nothing. The DSM-5 (American Psychiatric Association, 2013) contributes to the confusion when, in some pathologies such as PTSD, it mentions the "inability to recall key features of the trauma" as a criterion (Manzanero et al., 2020).
The reduction of cognitive resources by the effect of high levels of activation (stress) (Yerkes & Dodson, 1908) produces a narrowing of the attentional focus (Easterbrook, 1959). It hinders the integration processes in the generation of memory traces. As a result, the memories of traumatic events associated with high anxiety levels are characterized by a detailed description of the central information but with few peripheral details (Byrne et al., 2001). Traumatic memories frequently appear fragmented and predominantly sensorial (as processing sensory information requires few cognitive resources). This lack of cognitive resources in the coding phase would also cause weak memories, hindering in-depth information processing and the establishment of associations with prior knowledge and experience (Craik & Lockhart, 1972).
In traumatic events, deficits in encoding processes would hinder explicit (controlled) retrieval but allow implicit (automatic) retrieval, likely leading to incidental memories instead of deliberate ones (Graf & Mandler, 1984; Schacter, 1987). Incidental retrieval involves non-conscious retrieval processes; thus, it is not possible to identify the recovery signs that make this memory accessible, and therefore, it is not possible to control them (Baddeley, 1990).
Depersonalization is often interpreted as a symptom of amnesic dissociation in victims of traumatic events. However, it is normal for autobiographical memories to be recovered from different points of view, such as an observer's perspective (in the third person or as if it were a film) or from the protagonist's perspective. This difference is not necessarily due to a pathology like dissociation, which is serious and rare, but rather to the normal functioning of memory (D'Argembeau et al., 2003; Manzanero et al., 2015). It is also an effect of multiple recoveries that is typical in traumatic memories, and this can also be seen in the earliest and most elaborated memories (Crawley & French, 2005).
The current misconceptions about dissociative amnesia, viewing it as an amnesia rather than a phenomenon resulting from the normal functioning of memory in extreme psychological situations, contribute to the confusion surrounding the nature of dissociative amnesia. In reality, dissociative amnesia involves deficient coding of the event and the generation of incomplete or deficient memory traces that complicate its posterior recovery. Additionally, the complex verification of traumatic mechanisms, low incidence phenomenon, and important ethical implications in investigations all contribute to the maintenance of the phenomenon.
Problems in Studying Traumatic Memories
Brewin (2007) points out controversy due to variability in the findings on traumatic memories, with the sample being quoted as the main cause. Firstly, there is a problem with the presence of pathologies: studies involving clinical samples may not accurately represent the general population (Steel et al., 2009; Dimitry, 2012; Manzanero et al., 2021). Secondly, there is the problem of unverifiability of the event in non-clinical samples: it can be difficult to accurately assess the veracity of traumatic experiences, such as childhood traumatic events. Finally, there is the problem of the uncontrolled samples: studying victims of wars and catastrophes provides more reliable information on the characteristics of traumatic memories since the reality of the experience can be easily established (Patihis et al., 2019). However, extraneous variables such as organic damage, drug effects, pharmacological treatments, sleep deficits, and nutritional deficiencies affect the study result.
Many countries have proposed that sexual crimes against minors be considered imprescriptible, and associations of victims of child sexual abuse have arisen to uncover these types of crimes that have remained hidden for decades. However, proving such crimes is extremely difficult and some have advocated for the victim's testimony to be sufficient to establish a conviction, even if it distorts the presumption of innocence (Subijana & Echeburúa, 2018). In this context, memory experts have raised concerns about certain iatrogenic psychotherapeutic practices, such as guided imagination, dream interpretation, hypnosis, sodium amytal administration, and bibliotherapy, which may induce false memories in patients (Loftus, 2004). These false memories, combined with erroneous indicators of abuse, could lead to false complaints, even if the intention was to detect "repressed" cases of sexual abuse in childhood.
Factors such as the age of the victim at the time of the event(s), whether it was a single occurrence or repeated over time, the duration and type of aggression, the dynamics of the recall process, and the procedures followed to obtain the victim's statement; should be considered to minimize false accusations based on false memories. It is also important to consider whether it could be a "repressed" and then recovered memory, the number of victims, the relationship between the victim and the perpetrator, and any other relevant factors. For instance, it is not the same to consider a case of sexual assault that lasted for years during childhood and was always remembered by the victim but not reported due to embarrassment or fear, compared to a case where an adult victim undergoes therapeutic procedures to remember a single instance of sexual assault when they were less than five years old by a family member. While both cases may involve sexual assault, the latter is more likely to be a false memory than a recovered one.
The following is a model proposed to facilitate understanding the different degrees of accessibility of memories based on different factors.
Continuous Accessibility Model of Memory
Forensic psychologists have struggled to provide conclusive and reliable evidence for the existence of dissociative amnesia of traumatic events. Accumulated evidence alludes to a more vivid and repeated recall of traumatic events (Hirst et al., 2015; Manzanero et al., 2020; Porter & Birt, 2001). Nevertheless, reaching a consensus is important to conclude whether dissociative amnesia could or could not be considered in court.
Psychologists need to establish a solid empirical foundation to understand better the mechanisms of memory involved in remembering and forgetting traumatic memories. As suggested by Patihis et al. (2021), it is crucial to explore the nature of traumatic memories, their relationship with dissociation, and the phenomenon of repressed memories. A particular focus should be placed on studying the psychological mechanisms involved in motivated forgetting, retrieval inhibition (Catarino et al., 2015), and its association with emotion (Gagnepain et al., 2017).
Empirical evidence has challenged theoretical perspectives on memory deficits in trauma victims, as the accessibility of traumatic memories can vary greatly (see Figure 1). While amnesia is typically associated with organic damage resulting from head injuries, encoding conditions and retention factors can result in poorly detailed memories that are still considered memories, even without organic pathology. However, most traumatic experiences generate memories with expected characteristics and accessibility, particularly in primary and indirect victims. Social and individual factors can also contribute to memories with greater accessibility and vividness, which may be a precursor to PTSD, a memory disorder characterized by chronic accessibility of traumatic memories in the form of flashbacks, ruminations, or nightmares, with increasingly intense emotions associated with each recall (Rubin et al., 2008).
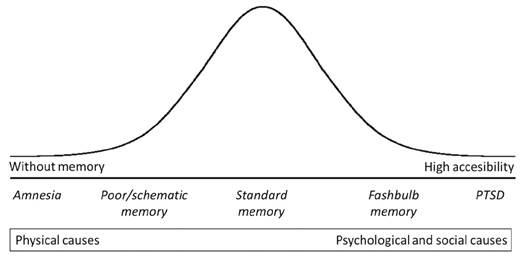
Figure 1. Continuous Accessibility Model of Memory, According to the Causes That Generate the Different Types of Memory
Individuals with PTSD tend to recall traumatic events in greater detail, and this is related to the number of recalls they make, which may lead to an over-generalization of retrieval cues (Desmedt, 2021). This over-generalization could reinforce the connections in the brain and increase memory accessibility, which is a step closer to developing PTSD.
However, some studies indicate that the risk of PTSD among victims of wars decreases significantly over time (Ehlers & Clark, 2003; Giacco & Priebe, 2018; Ssenyonga et al., 2013). These findings suggest that even for traumatic events, there is a natural decline in memory vividness, and coping with trauma may be promoted through time and acceptance of greater variability in recall, with less detail and more distance and perspective.
In the forensic context, it is important to distinguish the typical expression of the cause behind the memory impairment. For example, traumatic events likely lead to high accessibility of memories, although, as we noted above, these memories often appear fragmented and predominantly sensory. In the same sense, the model makes an important distinction between amnesia and poor memory because, as we said before, remembering poorly is not the same as not remembering anything. Finally, the model considers populations physically affected, healthy and exposed to traumatic events in a single continuum, allowing its use in different contexts.
Conclusions
This paper discusses the controversy surrounding dissociative amnesia in forensic contexts. The confusion between clinical psychology and forensic psychology, an inadequate definition of amnesia, and methodological problems in studying traumatic memories are core issues in this discussion. It is important to note that dissociative amnesia may be relevant in the psychotherapeutic context. However, it cannot be uncritically accepted in forensic psychology, where the underlying reality of the alleged event is the main point.
The Continuous Accessibility Model of Memory poses an alternative for understanding the different degrees of accessibility to memories depending on the causes. While organic causes are mainly associated with amnesia and/or poor memory, psychological and physical causes are associated with flashbulb memories and PTSD. Moreover, memory accessibility moves in a continuum from low accessibility, where the accuracy of recall is affected, to high accessibility, where control of recall is affected. The model also refers to the frequency on which these levels of accessibility appear in the general population in the form of a bell curve, with standard memory representing the “healthy” level of accessibility. However, it is important to point out that apparent “quality of recall” is not an indicator of veracity in testimony. The fact that a potential victim cannot remember the events does not necessarily mean they did not occur, as can happen in cases of crimes committed through chemical submission (Quintana et al., 2020). Similarly, remembering them is not indicative that it did happen, as demonstrated in cases of false autobiographical memories (Arce et al., 2023).

