










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Colorectal cancer (CRC) is the most frequent tumor and the second leading cause of cancer related death in Spain and the Western world 1,2,3. The progressive sequence from adenoma to carcinoma in the pathogenesis of CRC was first described by Fearon y Vogelstein 4. Since then, CRC has been one of the paradigms of the efficacy of screening programs in the general population 5,6. Apart from the reduction in incidence, several randomized trials and a meta-analysis have confirmed that CRC screening reduces specific cancer mortality by between 20% and 35% at five and eight years, respectively 7,8,9,10,11.
Full colonoscopy has the highest sensitivity and specificity of all the screening procedures applied. However, a major limitation is its invasive nature, which is not always readily accepted by the general population 12,13. Several studies have reported differences in the histologic phenotype and survival in patients whose tumors were diagnosed via a screening program as opposed to those diagnosed as a result of clinical symptoms 10,14,15,16,17,18.
The aims of the present study were to analyze the clinical and pathologic features of the tumors and compare the long-term oncologic outcome between patients in a screening program via colonoscopy and those diagnosed as a result of the development of CRC symptoms (non-screening group).
MATERIALS AND METHODS
All patients undergoing surgery for CRC with a curative intent with stage I, II, and III tumors as defined by the American Joint Commission on Cancer (AJCC) 19 between 2004 and 2014 were identified from a prospective database of patients, maintained since 1995. Colon cancer was defined as a tumor located between the cecum and the rectosigmoid junction at < 15 cm from the anal verge. Cases of stage IV disease were excluded as these require a different therapeutic approach. Cases of hereditary colon cancer and those associated with inflammatory bowel disease were also excluded.
Patients diagnosed via the colonoscopy screening program 6 of the center and those diagnosed as a consequence of clinical symptom presentation were identified. The following data were collected: demographic data (age and sex), ASA (American Society of Anesthesiologists) functional status 20, body mass index (weight in kilograms divided by height in meters squared) and data related to the surgical procedure (duration, type of operation [e.g., open vs laparoscopic], the use of blood products, overall incidence of complications and the number of severe complications defined as those equal or greater than class IIIb according to the Clavien-Dindo classification) 21. Colectomies were performed with proximal ligation of the mesenteric vessels and rectal excisions via full resection of the mesorectum 22,23. From 2008 onwards, most of the resections were performed laparoscopically 24.
Pre-operative anemia was defined according to the World Health Organization (WHO) criteria for adults over the age of 15 years as a hemoglobin level < 130 g/dl in males and 120 g/dl in females 25. Dehiscence of anastomoses was defined according to the criteria of the International Group of Rectal Cancer 26 and hospital mortality was defined as that occurring during the first 30 days after surgery or during hospital admission for the surgery.
Histopathologic analyses were performed according to the norms of the American College of Pathologists and pathologic staging (TNM) using the criteria of the American Joint Committee on Cancer Staging, 7th edition 19,27. Perineural and lymphovascular invasion were classified according to the Batsakis and Sato criteria, respectively 28,29. The degree of tumor differentiation was assessed using the WHO classification 30.
Adjuvant chemotherapy for colon cancer was administered according to the norms of the American Society of Clinical Oncology (ASCO) and the Spanish Society of Medical Oncology (SEOM) 31,32. Locally advanced rectal cancers (at stages cT3-4 or cN1) and clinically bulky tumors received external radiotherapy (45 Gy to 54 Gy) neoadjuvant treatment over four weeks in combination with 5-fluorocil-based chemotherapy, according to a regimen described previously 33. All patients were monitored according to the guidelines established by the SEOM 32,34.
The diagnosis of local recurrence was made on the basis of histologic or radiologic confirmation and supportive laboratory findings. Disease-free survival (DFS) was defined as the time elapsed between surgery and the first recurrence or loss to follow-up. The screening and non-screened groups of patients were compared for the primary outcomes described above. The groups were matched for survival analysis according to the pathologic stage of the tumor (I, II and III) to determine if this feature affected the long-term outcome at each stage.
The study was approved by the Research Ethics Committee of the center. All the authors contributed to the drafting of the manuscript.
STATISTICAL ANALYSIS
Descriptive statistics were calculated for the screening and non-screened groups. Continuous variables are described using the mean and standard deviation and the difference between these variables was analyzed using the Student's t-test. Categorical variables are described using frequencies and percentages and the difference between groups was measured using the Chi-squared test, or the Fisher's exact test when the number of cases was less than 5. A two-tailed p value of < 0.5 was considered to be statistically significant.
A Kaplan-Meier analysis was performed to assess overall and disease-free survival. The analysis was performed according to tumor stage and the results were compared using the log rank test in order to calculate the p value of the difference between the groups. Univariate Cox regression was used to assess the association between type of diagnosis and survival. All analyses were performed using the SPSS statistical package (SPSS, Inc., Chicago, IL). Differences were considered significant at p = 0.05.
RESULTS
Of a total of 2,903 patients that underwent surgery for colorectal cancer, 1,580 met the inclusion criteria; 950 patients had colon cancer and 630 had rectal cancer (Fig. 1). Colon cancer was more frequently diagnosed than rectal cancer in the screening program (80% vs 56.4%; p < 0.01). There were no differences with regard to right sided colon cancer in the screening and non-screening group (50% vs 44.1%; OR 1.26; 95% CI 0.92-1.73; p = 0.139) (Table 1). Demographic data and those related to surgical risk, the surgical procedure, post-operative complications, histologic parameters and pattern of recurrence are summarized in Table 1. There were no differences between the two cohorts with regard to gender, BMI and ASA functional status. The patients with symptomatic tumors had significantly lower baseline levels of hemoglobin (p < 0.01).
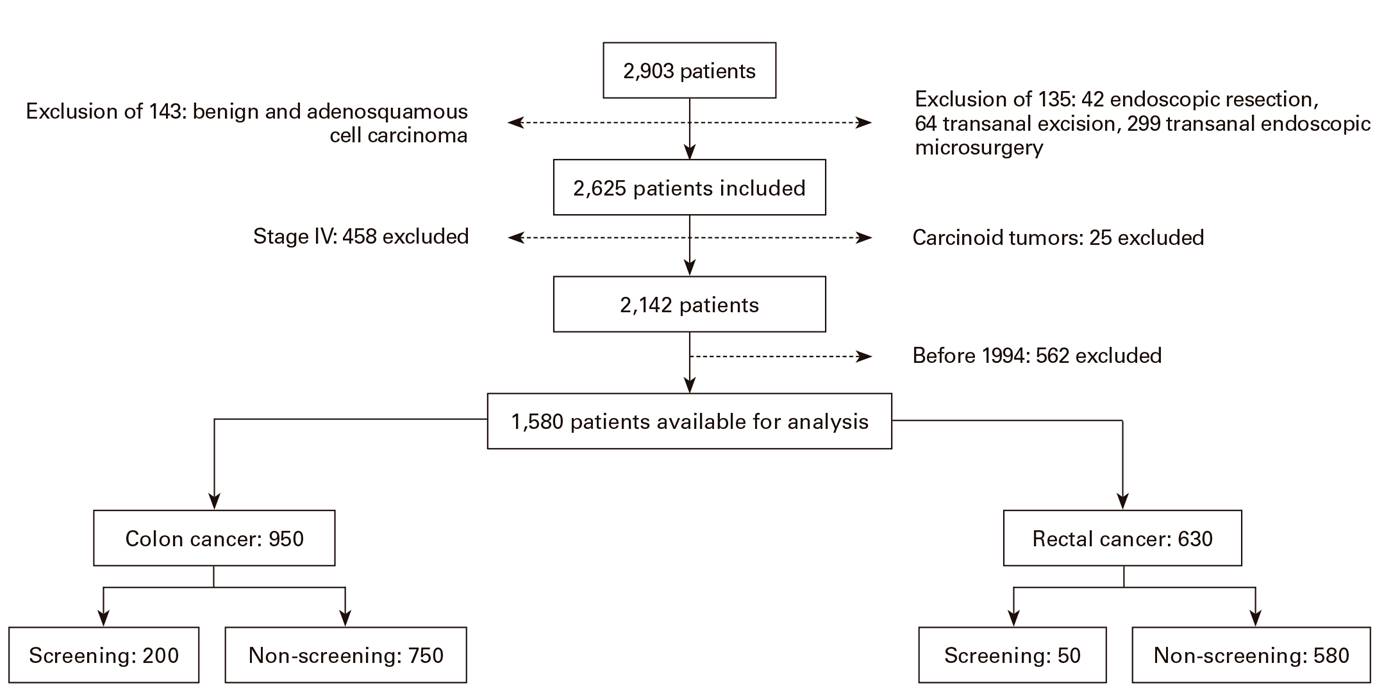
Fig. 1 Flowchart of the total population. All cases of colorectal cancers surgically treated from 1995 to 2014.
With regard to surgical parameters, there were no differences in the time taken for the procedure. Although laparoscopic techniques were used more frequently in the screening group as opposed to the non-screened group (44.4% vs 20.5%; OR = 3.08, 95% CI = 2.32-4.09; p < 0.01). Patients with symptomatic tumors required more blood products but there were no significant differences between the two groups with regard to the incidence of operative complications, the rate of severe complications (Clavien-Dindo ≥ IIIb), dehiscence of anastomoses or operative mortality (Table 1). There was a significantly higher prevalence of adenocarcinomas, larger and poorly differentiated tumors in the symptomatic group. There was also a lower prevalence of carcinoma in situ, with more advanced pathologic stage and a greater incidence of perineural and lymphovascular invasion (p < 0.01 for all values) (Table 1).
Table 1 Patient demographics, tumor characteristics, treatment and outcome of screening and symptomatic patients
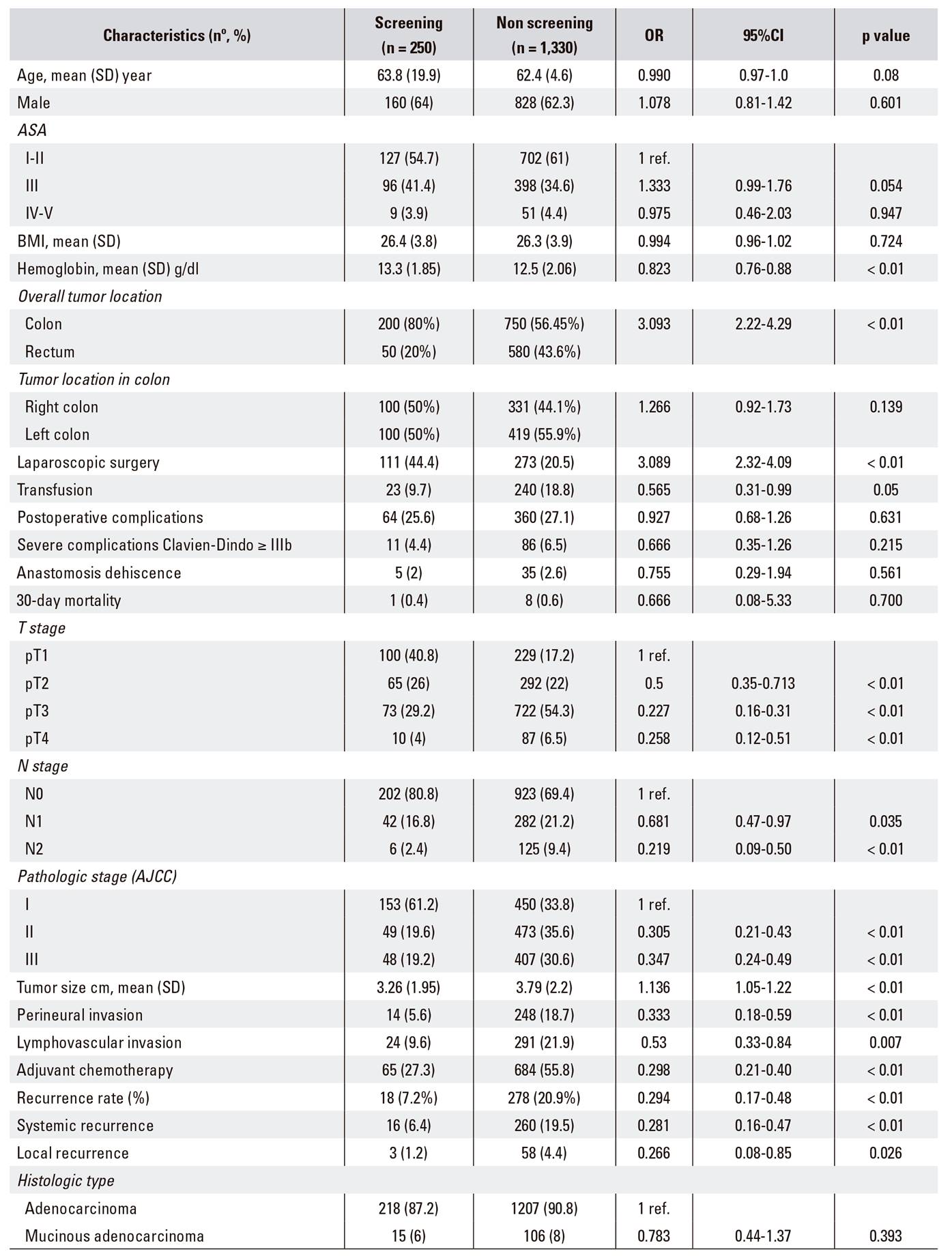
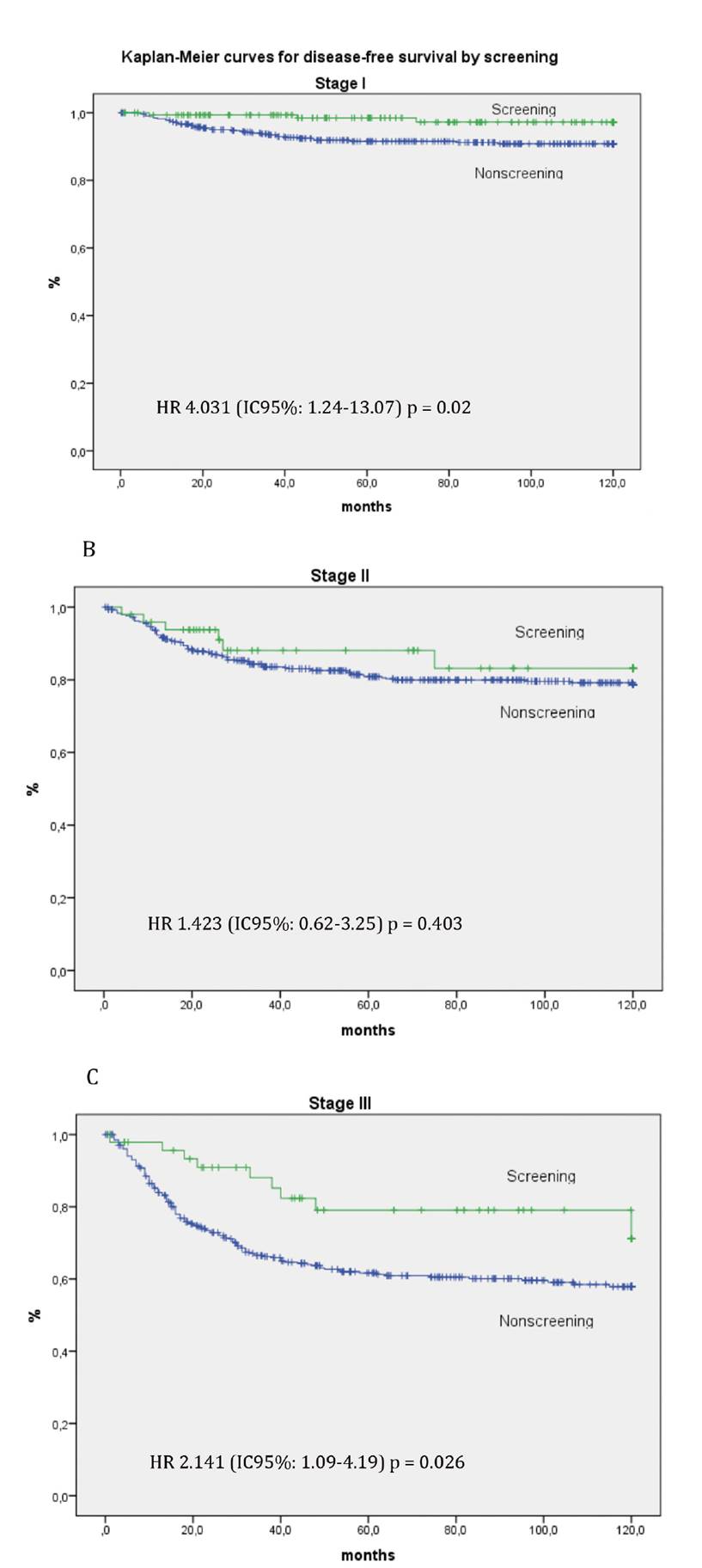
Two hundred and twelve patients died from colorectal cancer during a median follow-up of 85 months; eleven and 201 in the screening and non-screening group, respectively. There was a significantly greater incidence of recurrences during follow-up in patients with symptomatic tumors than in the screening group, 7.2% vs 20.9% respectively (OR = 0.294; 95% CI: 0.17-0.48, p < 0.01). Distant recurrences were more frequent than local recurrences in both groups (Table 1). Disease-free survival at five and ten years was significantly higher in the screening program as compared to those that presented clinical symptoms (HR 2.93, 95% CI 1.82-4.72; p < 0.01) (Fig. 2). However, there were differences between patients with stage I, II and III tumors in both groups with regard to disease-free survival by pathologic stage (Fig. 2). Disease-free survival at five years was significantly higher in the screening group as compared to the symptomatic patients group; 98.4% and 91.5% for stage I (HR 4.03; 95% CI 1.24-13.07; p = 0.02) and 79.1% vs 61.7% for stage III (HR 2.14; 95% CI 1.09-4.19; p = 0.02) (Fig. 3C).

DISCUSSION
Colorectal cancer is the second leading cause of cancer death in Spain and the Western world 1,2,3,35. Its growth pattern follows an adenoma to carcinoma sequence and screening programs have shown their efficacy in reducing the incidence and specific mortality from cancer 4,7,8,10,11,12. The main objective of this study was to compare the long-term oncologic outcome of stage I, II and III colorectal tumors diagnosed via a screening program using full colonoscopy as opposed to those diagnosed due to the appearance of symptoms. Stage IV tumors were excluded as they require a different therapeutic approach 36.
In our study, there were no significant differences in the demographic variables, baseline physiologic status (ASA, BMI) and degree of severity of post-operative complications between the screening and symptomatic patient groups. The only noteworthy parameters were significantly lower hemoglobin levels in the symptomatic patients and more laparoscopic colectomies in the screening group. The similarity in age between the two groups is striking, as the average age of the screening group would be expected to be lower as clinical guidelines recommend screening from the age of 50. This difference was reported by other studies 5,10,16,37. However, similar survival rates (non-significant p) between both groups for stage I and II tumors was observed when survival was analyzed independently according to pathologic stage. In contrast, overall and disease-free survival for stage III disease were significantly higher in the screening group. These differences are consistent with those reported by other studies 10,16,38. However, the reasons for such differences have been a matter of debate, as in our study. There were no differences in age, preoperative risk factors or post-operative complications in these subpopulations of patients (stage III), which is consistent with other studies 10,16,17. As a possible explanation, it has been proposed that symptomatic tumors express a more aggressive biological phenotype and grow more rapidly than the "silent" tumors that are diagnosed incidentally via a screening program 10,16,39,40.
Several studies have linked these differences to lead time bias and length time bias. Lead time bias occurs as a result of early diagnosis, in such a way that survival is additionally and artificially prolonged. In theory, both cohorts would have the same survival time if they had been diagnosed due to the presence of symptoms 17,41,42. Length time bias is produced due to the slower growth of tumors identified via screening programs, which have a longer latent or pre-symptomatic phase. Thus, these tumors are more likely to be diagnosed in screening programs and therefore, survival is also artificially overestimated in these patients 17,41,42.
Although pathologic stage (TNM) and histologic parameters are the most important prognostic factors to determine long-term outcomes in CRC, there are other factors related to the host and surgical treatment which may have some bearing on our findings 14,15. Most authors agree that the subjects that voluntarily enroll in a screening program are more responsible, more health conscious, more likely to follow health care recommendations and usually have a better prognosis due to their habits and lifestyle. The symptomatic patients presented tumors at more advanced stages and with a greater number of histological factors indicative of a poor prognosis (presence of perineural invasion, positive lymphovascular invasion and poorly differentiated tumors) than those diagnosed incidentally. This has also been reported by other studies 10,16,17,18. Furthermore, lower T stage and more stage I tumors and less rectal tumors were found in the screening group (Table 1). Logically, these findings were associated with a lower overall and disease-free survival in symptomatic patients as compared to the screening group 16,17,18. Due to all of these reasons, it is considered that screening could bias survival outcome 43,44,45.
In our study, the patients from the screening group required fewer blood products and had significantly higher baseline hemoglobin levels. It is well known that blood transfusion leads to a decrease in the cellular adaptive immune response, which in turn is associated with an increase in tumor recurrence. However, there were no differences in operative time or the incidence of severe post-operative complications in our series. These factors are also associated with a reduction in survival time in colorectal cancer 46,47,48.
Our study suffers from the limitations inherent to retrospective studies, which cover a wide period of time, 20 years in this case. There may have been variations in the therapeutic approaches throughout this period. Although it is true that all the patients underwent surgery performed by colorectal surgeons with standardized criteria and all the data were collected prospectively. Furthermore, as our center is specialized in the treatment of these patients, the delay between cancer diagnosis and surgery was relatively brief.
Our results confirm the positive effect of colorectal cancer screening on survival in patients with potentially curable tumors (stages I and III) that are treated with surgery. Such findings support the efficacy of screening programs in CRC and serve as an argument in favor of implementing preventive measures in the general population.

