










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkREC: Interventional Cardiology
versão On-line ISSN 2604-7276versão impressa ISSN 2604-7306
REC Interv Cardiol ES vol.5 no.4 Madrid Out./Dez. 2023 Epub 04-Mar-2024
https://dx.doi.org/10.24875/recic.m22000320
Clinical cases
Massive hemoptysis. Selective embolization of bronchial artery-left pulmonary artery fistul
aServicio de Cardiología, Unidad Cardiovascular, Sanatorio Allende, Córdoba, Argentina
bServicio de Neumonología, Sanatorio Allende, Córdoba, Argentina
cServicio de Diagnóstico por Imágenes, Sanatorio Allende, Córdoba, Argentina
CASE PRESENTATION
Hemoptysis is the subglottal expectoration of blood from the tracheobronchial tree. Most cases of massive hemoptysis originate at the bronchial arteries (90%) and often become complicated due to systemic arterial blood pressure. The mechanism of action is the rupture of hypervascularized reticulum and vascular dilatation as a response to the substances released in the inflammatory process. This clinical entity has elevated morbidity and mortality rates. Early diagnosis and the timely administration of therapy are of paramount importance.
This is the case of a 73-year-old woman with a past medical history of breast cancer with ED presentation of early onset massive hemoptysis. She was admitted to the intensive care unit with a heart rate of 122 bpm, arterial blood pressure of 78/45 mmHg, and oxygen saturation of 82% with high-flow oxygen mask. Emergency orotracheal intubation and mechanical ventilation were decided. Given the patient's hemodynamic instability, vasopressor drug infusion was started at increasing doses until a mean arterial blood pressure of 60 mmHg was reached with noradrenalin at 0.3 μg/kg/min. Lab test results showed hemoglobin levels of 7.5 g/dL, hematocrit of 21%, PaO2 of 62%, and hyperlactacidemia. A total of 2 bags of packed red blood cells were transfused, and the patient was transferred to the computed tomography scan room. The CT scan revealed the presence of a fistula from the left bronchial artery towards the upper branch of the left pulmonary artery with images consistent with alveolar hemorrhage compromising all lobes from both pulmonary fields (figure 1).
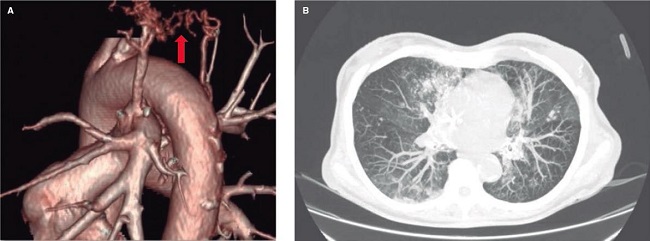
Figure 1. Computed tomography scan at admission. A: 3D reconstruction showing the arterio-arterial fistula from the pulmonary artery branch towards the bronchial artery. B: axial view showing an image consistent with bilateral alveolar bleeding.
It also revealed the occupation of the left main bronchus and the lower and upper lobe branches with dense material suggestive of blood clots due to its high spontaneous density (figure 2). Given this clinical presentation and the features revealed by the CT scan, right bronchial selective intubation was decided. Afterwards, the patient was immediately transferred to the cath lab for endovascular embolization.

Figure 2. Computed tomography scan at admission. Coronal view showing the left main bronchus occupied by the blood clots.
The patient gave her informed consent for publication purposes.
SEE RELATED CONTENT:
https://doi.org/10.24875/RECICE.M22000325https://doi.org/10.24875/RECICE.M22000326 Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
