










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.5 Madrid Mai. 2017
PICTURES IN DIGESTIVE PATHOLOGY
An unusual cause of Boerhaave's syndrome in a young patient
Samuel Raimundo Fernandes1, Carlos Noronha-Ferreira1, José Paulo Freire2 and José Velosa1
1Department of Gastroenterology and Hepatology. Hospital de Santa Maria. Centro Hospitalar Lisboa Norte. Lisbon, Portugal.
2Department of General Surgery. Hospital de Santa Maria. Centro Hospitalar. Lisbon, Portugal
Author contributions: Samuel Raimundo Fernandes (MD), Carlos Noronha Ferreira (MD) and José Freire (MD): elaboration and critical review of the manuscript. José Velosa: critical review of the manuscript.
Case report
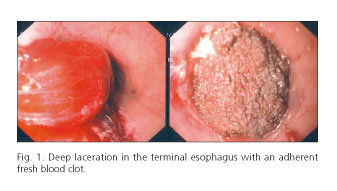
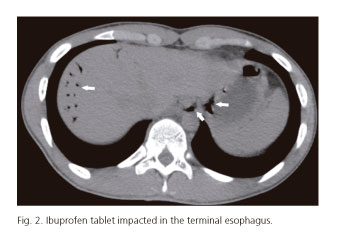
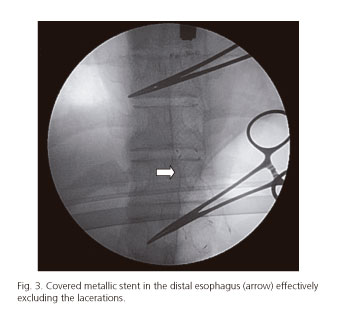
An 18-year-old male patient with a history of atopy and intermittent dysphagia for solids presented to the Emergency Department with sudden onset total dysphagia followed by hematemesis, after ingesting an ibuprofen tablet. Urgent upper gastrointestinal endoscopy revealed a deep laceration (Fig. 1) just above the tablet impacted in the distal esophagus (Fig. 2). Abdominal computed tomography (CT) scan confirmed the suspicion of an esophageal perforation. The impacted tablet was broken up with biopsy forceps, and a covered metallic stent (Hanarostent® 60/100 x 20/26 mm) was placed across the cardia effectively excluding the fistula (Fig. 3). Recovery was uneventful and the stent was easily removed six weeks later. Follow-up biopsies showed marked mucosal infiltration by eosinophils confirming the diagnosis of eosinophilic esophagitis (EE). The patient was treated with oral budesonide and remains asymptomatic.
Discussion
EE is a chronic inflammatory condition of the esophagus typically presenting with dysphagia and food impaction in adulthood (1). Sustained chronic inflammation may weaken the esophagus predisposing to a potential perforation (1). However, perforation unrelated to endoscopic maneuvers has rarely been reported in EE (1-3). In a recent review including 511 patients with EE, perforation occurred in only 2.0%, mostly related with prolonged food bolus impaction (2). While surgery has been classically advocated for this complication, endoscopic management using self-expanding stents may present an alternative (3), as shown in our case. Potential benefits include lower morbidity, earlier resumption of oral feeding and shorter duration of hospitalization.
References
1. Lucendo A, Friginal-Ruiz A, Rodríguez B. Boerhaave's syndrome as the primary manifestation of adult eosinophilic esophagitis. Two case reports and a review of the literature. Dis Esophagus 2011;24(2):E11-5. DOI: 10.1111/j.1442-2050.2010.01167.x. [ Links ]
2. Runge T, Eluri S, Cotton C, et al. Causes and outcomes of esophageal perforation in eosinophilic esophagitis. J Clin Gastroenterol 2016. In press. DOI: 10.1097/MCG.0000000000000718. [ Links ]
3. Jacobs J, Fatima H, Cote G, et al. Stenting of esophageal perforation in the setting of eosinophilic esophagitis. Dig Dis Sci 2014;60(4):1098-100. DOI: 10.1007/s10620-014-3387-9. [ Links ]
