










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Traumatic dental injuries (TDI) accounts for about 5.0% of all bodily trauma.1-3 However, its incidence and characteristics changes according to age group and socio-demographic factors involved, as is the case of children injuries, in which TDI represents 17.0-20.0% of all traumas they were involved in.4
Unlike other injuries, the incidence of these lesions decreases from the second decade of life.1,2,4 This can be explained by periodontal ligament space characteristics, upper incisor exposure and lack of lip sealing during the growth phase. In addition, there is an association between Class II malocclusion and TDI.5 Among dental elements, the upper central incisors are most commonly affected due to their projection and exposure.5 Less complex injuries such as single crown fracture and concussion are more frequent than complicated crown fractures or severe dental dislocations.6,7
TDI is a public health hazard due to its high frequency and association with violence, traffic accidents and sports activities.8-10 These injuries have an impact on the quality of life of patients by impairing chewing, phonation, esthetics, as well as their physical and psychological condition.7,11,12
Knowledge of TDI characteristics is important for the establishment of preventive action and treatment so as to reduce associated costs and improve the population's quality of life.9,12 This study aims to identify the characteristics and factors associated with TDI in patients treated at a specialized service for a ten-year period.
Material and methods
The present cross-sectional retrospective study was reviewed and approved by an Institutional Research Ethics Committee for Human Beings (protocol n. 049/2007). Records of patients treated at an Oral and Maxillofacial Surgery Department (Pelotas, south of Brazil) during a ten-year period were evaluated. Patients with DAT records in permanent teeth were included in the study, but those with incomplete records or showing other kinds of injury were excluded.
After researcher calibration, data were collected and transferred in duplicate to a table specifically created for the study. The collected variables were age, gender, cause of trauma, presence and type of dislocation, tooth fracture and bone plate fracture. Data were analyzed by means of descriptive statistics, and the chi-square test at 95% significance level was performed; when the null hypothesis was rejected, complex analysis to verify the association between variables was carried out.
Results
After collection, 545 records of patients treated at the service were included in the study, 387 of whom (71.0%) were male and 158 (29.0%) female. As to age, there was an average of 20.77 ± 12.04 years, and the study included patients ranging from six to 63 years, with a median of 17 years.
The prevailing age group was between 13 and 19 years (30.6%), followed by 6-12 years (27.9%) and 20-29 years (22.2%). The most common etiologies were bicycle (20.4%) and traffic (16.9%) accidents, falls (16.1%) and aggression (16.0%) (Table 1).
Table 1 Distribution of TDI cause according to gender, age, TDI type. Chi-square association test and complex analysis.
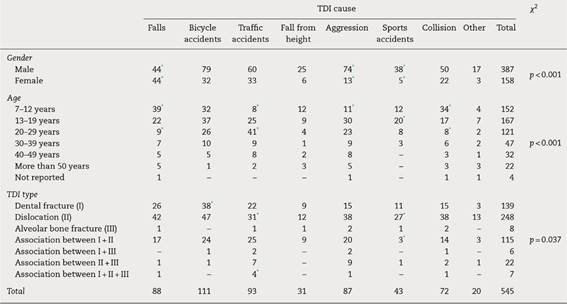
*Statistically significant association through complex analysis.
The 545 patients included in the study had a total of 1304 teeth affected by TDI, an average of 2.39 ± 1.69 teeth per patient. Twelve was the maximum number of affected teeth in one isolated patient, with four cases. The most affected dental elements were the maxillary central incisors (57.0%), followed by upper lateral incisors (17.7%), lower central incisors (9.3%) and lower lateral incisors (6.7%) (Table 2).
Table 2 Distribution of affected tooth according to age, TDI cause and TDI type. Chi-square association test and complex analysis.
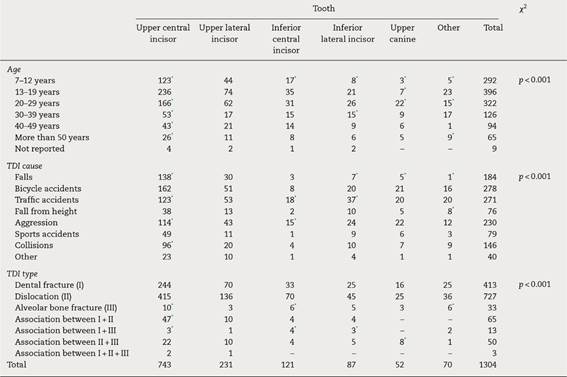
*Statistically significant association through complex analysis.
Concerning TDI, 1438 injuries were observed, among which dental dislocations were found in 55.8% of cases alone, whereas 9.0% were associated with dental and/or bone fractures. Dental fractures occurred isolatedly in 31.7% of cases whereas in 6.2% of them were associated to other kinds of injuries. Alveolar bone fractures occurred in isolation in 2.5% of cases as contrasted to 1.2% associated with tooth fractures or dislocations (Table 2).
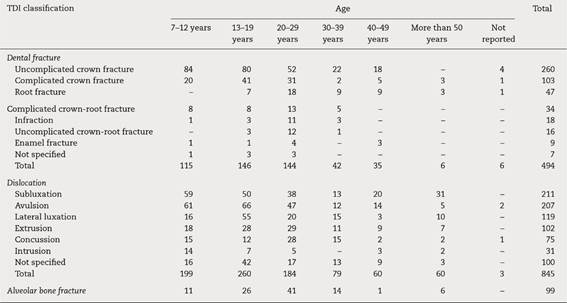
Among dental fracture types, uncomplicated crown (52.6%) and complicated crown (20.9%) were the most frequent. As to dislocation, subluxation and avulsion occurred most frequently, with 25.0% and 24.5% respectively (Table 3).
The chi-square association test was statistically significant upon crossing all categories of variables (p ≤ 0.05), except for gender and age (p = 0.06), gender and dental element (p = 0.57), gender and TDI type (p = 0.42), and age and TDI type (p = 0.65). Tables 1 and 2 include variable crossings that showed statistically significant associations, as well as complex analysis which highlight the associated pairs of variables.
Regarding the cause of trauma, statistical analysis mainly demonstrates a positive association between male patients with aggression, falls and sport accidents; age (7-12 years) with falls and collisions; age (13-19 years) with sports accidents; age (20-29 years) with traffic accidents; dental fractures with bicycle accidents; and dislocations with traffic and sports accidents (Table 1).
Concerning the involved tooth in trauma, upper central incisors were associated all ages, except 13-19 years which was associated with upper canines. About cause, upper central incisors had association with falls, traffic accidents, aggression and collisions; inferior central incisors with traffic accidents and collisions; and lateral inferior incisors with traffic accidents (Table 2).
Discussion
The present retrospective study was conducted at a permanent tooth trauma monitoring and treatment center of a public institution service. Patients treated in this service are usually forwarded to Emergency Hospitals due to facial injuries. TDI cross-sectional studies allow monitoring higher age and gender prevalence, in addition to the association between different TDI and causing factors.7,9
A male prevalence at a 2.4:1 ratio was found. This finding is supported by other research in the literature, and it is agreed that boys play sports and high risk competitions of intense contact; in adult men, in turn, TDI is additionally related to traffic accidents and aggression.9,13,14 In this study, an association between gender and cause was also found, inasmuch as men, regardless of age, showed TDI due to falls, aggression and sports.
One of the major TDI risk factors is age, and the most affected age group consists of children and adolescents.1-3 The high number of injuries in this population can be explained by their daily activity characteristics, with great time spent in recreation and sports.15 In this retrospective study, 58.5% of cases were reported in patients between six and 19 years of age. The average age of 20.77 years observed in the study was similar to that found in literature.7,16
The cause-age association showed that children aged seven to 12 years suffer TDI by fall, collision with objects, traffic accidents and aggression, in this order. Falls and collisions are major causes related to school recreational activities.17 In these cases, preventive actions are rare and difficult to implement.16 However, aggression cases can be accounted for by school fights and domestic violence, and the evaluation of these patients is essential to the identification of likely domestic aggression and its report to authorities.18 The main etiology for teenagers between 13 and 19 was associated to sports, which is also in agreement with that described in literature, and reinforces the need to use mouth guards to prevent these injuries.5,19
Dental dislocations were the most prevalent TDI type, being present in 64.8% of cases. This type of TDI occurs mainly in children and adolescents6,20 due to anatomical characteristics during the phase of mixed dentition and facial growth.5 In this period, the periodontal ligament space is increased, being a dislocation predisposition and, since the mandible has not its fully developed yet, there may be lack of lip seal and excessive incisor exposure. In this study, 54.3% of dental dislocations affected patients of up to 19 years.
Higher impact etiologies are related to a greater transmission of forces to supporting tissues, dental dislocations and bone fractures.16 Medical records of the evaluated patients showed an association between bicycle accidents and dental fractures, traffic accidents with dental and bone fractures, and sports accidents with either isolated dislocations or associated with dental fractures. Thus, in the face of TDI due to higher impact accidents, injuries to the periodontal tissues should be investigated, since they show greater severity and a worse prognosis.7,13
As to TDI classification, infraction, enamel fracture and uncomplicated crown fracture accounted for only 19.9% of all injuries. The high prevalence of other lesions with pulp and/or supporting tissue involvement can be explained by the characteristics of the evaluated service. Because it is an institutional public care TDI specific service, less severe cases are resolved in the public health network, without the need for referral. Among dental elements, the results found in this study are in agreement with those in literature, which point to upper incisors as the most usually affected teeth.3,13
The knowledge of dental trauma epidemiology has an important role in clinical treatment of those injuries. According to patient profile (age, gender and cause of trauma) the attendance may be prepared for the most associated diagnosis and involved teeth. Thus, it may improve the early treatment and prognosis of the injuries.
Considering the limitations of a retrospective analysis conducted at a single TDI-referral center, TDI prevalence in children and adolescents was found along a ten-year period due to falls, collisions and traffic and sports accidents. Most TDI showed an involvement of supporting and/or pulp tissues, the upper central incisor being the most affected tooth.

