










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Antineoplastic chemotherapy consists of the use of cytotoxic drugs alone or in combination, which act on tumor cells. In order to inhibit the proliferation of cancer cells, the cell cycle is one of the main foci in the action of antineoplastic agents. Each drug class will act at a particular stage of the cell cycle, not only acting on cancer cells, but also on normal cells of rapid proliferation. Therefore, these drugs produce undesirable side effects and are toxic to those taking such medications (1).
Immunotherapy presents as the great proposal of treatment of some neoplasias with a focus on the decrease of adverse reactions. Tumor immunotherapy is based on the use of elements of the immune system to eliminate or neutralize tumor cells and factors that benefit tumor survival (2).
Monoclonal antibodies, as target therapy, have high specificity with few side effects, being the focus of many research on diseases that require more aggressive treatment. These agents are gaining space in the treatment of some types of cancer, as is the case of Trastuzumab in the treatment of breast cancer, Cetuximab in the treatment of colorectal cancer and Rituximab in the treatment of lymphomas (3).
There are few studies that are concerned with the toxicity of monoclonal antibodies in the treatment of malignancies. Therefore, this article aims to identify the main adverse reactions presented by patients in an outpatient clinic specialized in chemotherapy in the city of Caruaru-PE.
MATERIAL AND METHODS
This is a retrospective, quantitative and descriptive study based on the medical records of patients who used the monoclonal antibody Trastuzumab. Data collection took place from February to June 2017, in which the medical records of the patients of the Caruaru Oncology Center, who used the Trastuzumab antibody, were evaluated as isolated therapy or associated with other chemotherapeutic agents for the treatment of breast cancer HER2 positive.
A total of 59 patients attended at the outpatient clinic from January 2015 to December 2016, who used the monoclonal antibody Trastuzumab, associated or not with other antineoplastic agents, were excluded only patients who underwent hormone therapy, since hormone therapy alone, may be object of study in specific work, not being included in the objectives of this work. The analysis of medical records sought data such as: patient identification, cancer classification, drugs used to treat cancer, time of chemotherapy treatment, presence of associated diseases, laboratory and imaging exams, using as an aid an adapted data collection tool of the Instrument for Data Collection of the Oswaldo Cruz Foundation’s Report of 2014.
The inclusion criteria used were female patients with HER2-positive breast cancer who used Trastuzumab in the treatment of their neoplasia, whether or not they were associated with other antineoplastic agents. The established exclusion criteria were patients with other types of cancer that did not express the HER2 receptor, as well as smokers and patients who underwent antiestrogen therapy.
After the retrospective analysis of the medical records, it was verified that of the 59 patients selected, only 24 met the established criteria.
RESULTS
The study consisted of 24 female patients with HER2 positive breast cancer, in whom the analysis of the data collected revealed that the patients’ age ranged from 35 to 71 years. It was verified that about 6 patients had hypertension and 2 had diabetes. Regarding the histological classification of cancer, 21 patients presented Ductal Invasive Carcinoma, figure 1 shows the main histological types presented by the patients.

FIGURE 1 Prevalence of the histological type of breast cancer in the patients analyzed in this study
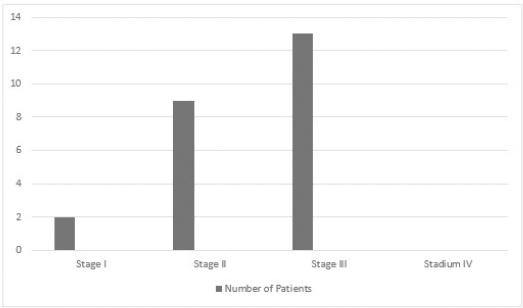
Analyzing the clinical staging of these patients, it was observed that of the 24 patients, 13 had stage III, 4 stage IIB, 3 stage IIA, 2 stage II and 2 stage I, which shows a predominance of patients in stage III, in the sample there were no patients in stage IV.
Regarding the therapeutic approach, about 8 patients underwent a surgical procedure, of which 6 performed Radical Mastectomy and 2 underwent Quadrantectomy with axillary emptying. Regarding radiotherapy, 19 patients performed, of which 10 did before starting treatment with Trastuzumab and 9 discontinued the use of Trastuzumab for radiotherapy and returned to the administration of Trastuzumab after radiotherapy, in which the mean dosage was 50.4 Gray.
As for chemotherapy, the vast majority of patients had protocols with anthracyclines, as shown in figure 2, in which the protocol Doxorubicin associated with Cyclophosphamide was one of the most used by the study patients. After treatment with anthracycline protocols, 16 patients performed protocols with taxanes associated or not with Trastuzumab, of which 10 used Paclitaxel and 6 who used Docetaxel.

During the administration of the doses of Trastuzumab, three patients discontinued the use of the monoclonal antibody due to a decrease in the ejection fraction after the 6th, 7th and 10th cycles, one presented pulmonary thromboembolism after the 6th cycle, another presented dysuria after the 7th cycle, another patient had a seizure after the 12th cycle of Trastuzumab, in which an magnetic resonance imaging was performed on the skull showing the possibility of metastasis. Another reported constipation after the second cycle, abdominal pain after the 7th cycle and nausea after the 9th cycle and another patient presented odynophagia after the 5th cycle of Trastuzumab.
DISCUSSION
Chemotherapy is based on the application of non-specific antineoplastic agents, injuring both normal and malignant cells, inhibiting the growth and / or vital processes of tumor cells (4). Currently, one of the major stakes in the treatment of cancer is immunotherapy, which consists of stimulation of the immune system through the use of substances modifying the biological response, which may occur through the result of the antigen-antibody interaction or the mechanisms involved in the mediated immunity by cells (5).
Monoclonal antibodies are products based on modified immunoglobulins, which exert a specific effect on a specific target, which makes it one of the great bets in the treatment of certain tumors, as it decreases the adverse reactions caused by the antineoplastic chemotherapeutics. The main antibodies used in the clinic are Cetuximab, Rituximab, Trastuzumab, Bevacizumab, among others (6).
Trastuzumab is a humanized monoclonal antibody that acts on human epidermal growth factor receptor-2 (HER2), in which its target is the subdomain IV of the extracellular region of HER2, being indicated in the treatment of breast cancer with high expression of HER2 and in the treatment of adenocarcinoma of the gastroesophageal or metastatic gastric junction with high expression of HER2. Its mechanism of action is associated with interference with signal transduction pathways, inhibition of extracellular domain cleavage, inhibition of DNA repair, reduction of angiogenesis, induction of cell cycle arrest, activation of antibody-dependent cellular cytotoxicity (6).
According to the study by Cintra et al (7), the age range of patients with breast cancer with HER2 overexpression presents in two peaks 40 and 59 years and 70 years or older, which is consistent with the data collected in the study, also demonstrating the predominance of invasive ductal histological type with 73.3% of the cases. With respect to clinical staging, Santos et al (8) demonstrated a greater number of patients with stage III and II, corroborating the data collected in this study, presenting 13 patients in stage III and 9 patients with stage II as shown in figure 3.
These are new drugs in the clinic, for this reason, there is very little information on its side effects, although its mechanisms of action are very specific, these monoclonal antibodies are not free of side effects. Trastuzumab is often associated with significant cardiotoxicity, which is primarily responsible for premature termination of treatment, in which this effect may be related to arterial hypertension, age greater than 50 years, exposure to anthracyclines (Doxorubicin, Epirubicin and Daunorubicin) and baseline left ventricular ejection fraction (9).
According to the study by Ayres et al (10), about 32.9% of patients using Trastuzumab have cardiotoxicity. Other adverse events also seen in chemotherapy combined with Trastuzumab include pain (myalgia / arthralgia) (20.4%), nausea and vomiting (15.9%), fever (9.7%) and neutropenia (7.1%), with respect to the use of Trastuzumab monotherapy, the most frequent adverse events were pain (19.6%), fatigue (10.8%), nausea and vomiting (9.8%) and headache (8.8%). Table 1 presents the main adverse events presented by the study patients, presenting results with some reactions different from those presented in the Ayres et al (10) study.
TABLE 1 Main adverse events found by the use of Trastuzumab
| Adverse event | Number of patients | Frequency |
|---|---|---|
| Cardiotoxicity | 3 | 12,5% |
| Pulmonary thromboembolism | 1 | 4,16% |
| Dysuria | 1 | 4,16% |
| Constipation | 1 | 4,16% |
| Abdominal pain | 1 | 4,16% |
| Nausea | 1 | 4,16% |
| Odynophagia | 1 | 4,16% |
Some clinical studies have demonstrated that Trastuzumab can cause damage to the myocardium, with a reduction in the contractile force of the left ventricle, and it is possible to reverse this clinical situation after the suspension of the drug since there is no damage to the cardiomyocyte. Between 3.5% and 17.3% of patients using trastuzumab associated with chemotherapy, there is a reduction in asymptomatic ejection fraction and from 2.5% to 5.1% have severe myocardial failure (11).
One of the most used tests in the clinic for the cardiac evaluation of these patients is the echocardiogram because it allows to evaluate not only the systolic function but also the diastolic function, the cardiac valves and the pericardium. The examination is performed periodically following the cycles of chemotherapy with this aiming to detect early myocardial lesion, in which the initial attention is attributed to the systolic function, with the calculation of the ejection fraction, the shortening function, the cavity dimensions and ventricular volumes (11).
According to the National Institutes of Health (NIH), the definition of cardiotoxicity in oncology in the last two decades is based on measurements of left ventricular ejection fraction (LVEF), defined as Grade I (asymptomatic LVEF reduction between 10% and 20%), Grade II (reduction of LVEF below 20% or below normal) and Grade III (symptomatic heart failure) (12). The three patients who discontinued use of Trastuzumab were due to drop in ejection fraction by more than 20%, indicating cardiotoxicity.
CONCLUSION
The analysis of the results of this retrospective study of the medical records of patients with HER2 positive breast cancer and the adverse reactions to the treatment with the monoclonal antibody Trastuzumab, concludes that the monitoring and notification of these adverse events, as well as the need for cardiological follow-up of these patients is of fundamental importance with a focus on the reduction of risks and the benefit of therapeutics. Because they are specific target drugs, few studies are concerned with evaluating the possible adverse events caused by these agents, often correlating with other clinical situations of cancer patients. Based on data found in the research, a need to combine efforts among efforts among oncologists, cardiologists, nurses and clinical pharmacists was recognized, in order to identify these adverse events.

