










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Body composition, admittedly plays a key role in the health/disease process, since its components have, among others, metabolic functions that may be involved in the prevention or genesis of various diseases 1,2,3,4,5. In this sense, the precise measurement or monitoring of fat mass (FM), lean mass (LM) or bone mineral content (BMC) can have significant clinical application, once can interfere in the diagnosis and prescription of drug or non-drug treatment 6,7.
Based on this premise, a recent systematic review 8 indicates that the dual energy X-ray absorptiometry (DXA) is being considered the new gold standard for measuring body composition, due to its high correlation with the methods of the MRI and computed tomography and present better cost benefit compared to these methods. This is making to engage yourself in some studies to analyze the reliability of measurements of the apparatus for body composition assessment 9,10,11,12,13,14. However, these studies only analyze the data relating to measures total body and not providing accurate information about DXA to measure segmental body composition.
Segmental body composition is measured by DXA defining regions of interest (ROI) 15, which can be automatically set by the apparatus or manually by the observer. Both definitions can lead to errors which, in turn, can interfere with the measurement result. In this sense, none of the studies reviewed had dedicated to analyze if assessing the measurements of ROI made by the same evaluator are accurate or not.
Therefore, this study aimed to evaluate the reliability of the measurement of body composition by DXA and intraobserver reproducibility for the measurement of ROI.
METHODS
SAMPLE
The sample included 15 young adults, males, apparently healthy and physically active who volunteered for the study. None of the volunteers reported use of drugs or any substance that could interfere with the results of the measures.
Before any test, all volunteers were informed of the possible risks and objectives of the study and signed informed consent to participate. All assessment procedures were done in the Exercise Physiology Laboratory of the Department of Biomedical Sciences at the University of León. The procedures used in this work were approved by the Ethics Committee of the University of León, in accordance with the ethical principles expressed in the Declaration of Helsinki.
PROCEDURES
To set the measurements precision, both the apparatus used and the evaluator who performed the measurements of the ROI, was conducted the design presented in Figure 1.
To check the reproducibility of DXA to measure body composition, the volunteers were subjected to two full-body scans by DXA using a densitometer General Electric, model Lunar Prodigy and the software Encore 2009, version 13.0. Before conducting the exploration, the equipment has been calibrated.
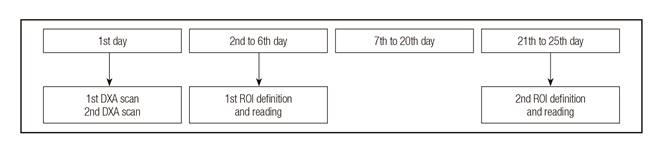
The two scans of each volunteer were done after stand by for 30 minutes and under the same conditions. In the first whole body scan (S1) by DXA, the volunteer laid in supine position on the device, with upper limbs extended and parallel to the trunk, hands pronated and supported on the device. The lower limbs were also extended, with standard separation at hip width and secured by a tape that held his ankles. They were instructed to remain as still as possible for the duration of the scan 10,15,16. After the end of the first scan, it was requested to the volunteer stands up and lies down again on device, keeping the same body position of the first scan. From there, the second exploration proceeded with another whole body scan (S2) by DXA. Each scan took about seven minutes and from S1 and S2, an automatic calculation of DXA outcome parameters (TBM, FM, LM, BMC) was achieved. For each subject, the following outcome parameters were obtained: TBMS1, FMS1, LMS1, BMCS1, TBMS2, FMS2,LMS2, BMCS2. Using these outcome parameters, were calculated the coefficient of variation (CV), the interclass correlation coefficient (ICC) and its 95% confidence interval (CI95%).
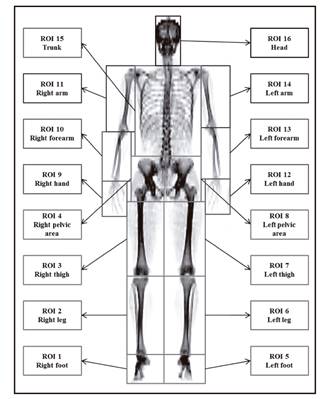
To measure the intraobserver reproducibility for ROI measures, in two different days (D1 and D2, seven to twenty days between both readings), one expert manually defined ROIs on the S1. Then, the body was divided into 16 ROI, determined based in some anatomical points, as follows:
Foot: it was considered as part of the bottom edge of the distal phalanx of the hallux to the line drawn on the medial and lateral malleolus of tibiotalar joint. The medial and lateral boundaries of the ROI were made so that encompasses all soft tissue. The same points were considered for the right and left feet.
Leg: it was measured starting from the line drawn on the medial and lateral malleolus of tibiotalar joint to the line drawn at the lower edge of the medial and lateral condyles of the knee joint. The medial and lateral boundaries of the ROI were made so that encompasses all soft tissue. The same points were considered for the right and left legs.
Thigh: it was measured from the line drawn at the lower edge of the medial and lateral condyles of the knee joint to the lower edge of the ischium. The medial and lateral boundaries of the ROI were made so that encompasses all soft tissue. The same points were considered for the right and left thighs.
Pelvic area: it was measured from the lower edge of the ischium to the posterior-superior border of the iliac crest. The medial boundary of the pelvic area was made by a line drawn from the midline of the pubic symphysis to the median line of the lumbar vertebra four (L4). The lateral boundary of the ROI was made so that encompasses all soft tissue. The same points were considered for the right half and the left half of the pelvic area.
Trunk: it was measured from the posterior-superior edge of the iliac crest to the upper edge of the sternoclavicular joint. The lateral boundaries of the ROI (arm spacing) were made along the midline of the glenohumeral joint, right and left.
Hand: it was measured starting from the lower edge of the distal phalanx of the middle finger to the line drawn on the lower edge of the medial and lateral styloid process of radiocarpal joint. The medial and lateral boundaries of the ROI were made so that encompasses all soft tissue. The same points were considered for the right and left hands.
Forearm: it was measured from the line drawn on the lower edge of the medial and lateral styloid process of the radiocarpal joint to the line drawn on the medial and lateral epicondyles of the humerus. The medial and lateral boundaries of the ROI were made so that encompasses all soft tissue. The same points were considered for the right and left forearms.
Arm: it was measured starting from the line drawn on the medial and lateral epicondyles of the humerus to the upper edge of the acromial extremity of the clavicle. The medial boundary of the ROI (separation of the trunk) was made in the midline of the glenohumeral joint and the lateral boundary was made so that all soft tissue was encompassed by the ROI. The same points were considered for the right and left arms.
Head: it was measured from the upper edge of the sternoclavicular joint to the cranial vertex.
All ROI are illustrated in Figure 2.
These ROI delineations were then used to compute the total mass of each body segment, for each subject. Using these outcome parameters, was computed the CV, the ICC and its CI95% to total mass of each body segment.
STATISTICAL TREATMENT
All statistical analyzes were performed in SPSS for Windows, version 21 (IBM, Chicago, USA). Initially, the data were subjected to normality test of Shapiro-Wilk. After, the descriptive analysis of the data was done, through the mean and standard deviation (SD). The reliability of body composition measurements by DXA was determined by calculating the CV and the ICC. ICC was also used to verify the intraobserver reproducibility for the measurement of each one of the 16 ROI, with a CI95%. A level of statistical significance of p < 0.05 was established for all treatments.
RESULTS
The 15 volunteers tested had a mean age of 24.25 ± 5.52 years, with extremes ranging between 18.5 and 36 years; an mean height of 179.80 ± 7.23 cm, with extremes of 169 and 192 cm; an mean body mass of 78.15 ± 7.92 kg, with extreme values of 67 and 99 kg; and an mean BMI of 24.13 ± 1.34 kg/m²,with extreme values ranging between 21.49 and 26.86 kg/m².
Regarding DXA reliability to measure the components of body composition, it may be seen in Table I that for all components, a low CV and high internal consistency of measurement repeatability were found.
Table I. Results of DXA reliability to measure TBM, FM, LM and BMC
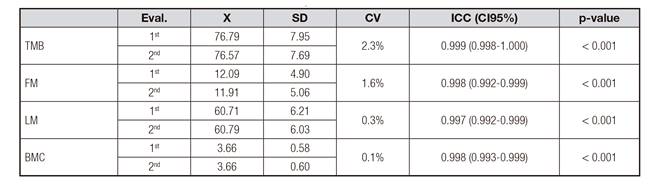
Eval.: evaluation; X: mean; SD: standard deviation; CV: coefficient of variation; ICC: intraclass correlation coefficient; IC95%: confidence interval of 95%; TBM: total body mass; FM: fat mass; LM: lean mass; BMC: bone mineral content.
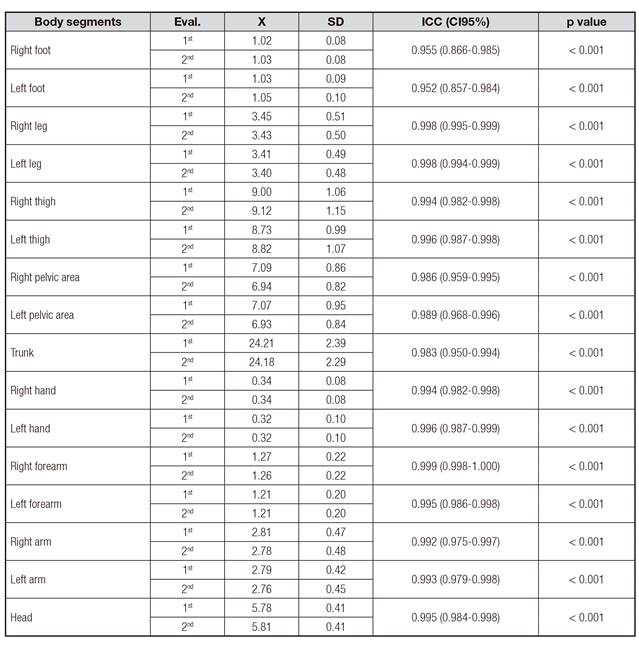
The results of the intraobserver reproducibility for the measurement of the 16 ROI show a high consistency of the measures of the two assessments, with intraclass correlation values slightly lower in the feet, pelvic areas and trunk, as shown in the Table II.
DISCUSSION
The reliability of results for DXA to measure the TBM, FM, LM and BMC, showed high levels of reproducibility for all components evaluated with lower CV (< 2.3%) and higher ICC (between 0.992 and 1.000).
Similar results were observed by Hind et al. 12, in a study that sought to assess DXA reliability in vivo (GE Lunar Prodigy) to measure body composition in 52 British adults. The authors found low CV for BMC (1.3%) and FM (2.5%). However, they did not describe the CV for LM and TBM. Similarly, Rothney et al. 14, in a study that aimed to characterize in vivo the reliability of total and regional body composition by DXA (GE Lunar iDXA) in a sample of obese American adults, found CV of 0.5% for BMC, 1% for FM and 0.5% for LM with the total body scanning.
In obese people, Carver et al. 11, who sought to evaluate DXA reliability (GE Lunar iDXA) to measure body composition and fat distribution, also observed low CV values for measures BMC (1.08%), FM (0.9%) and LM (0.94%). The authors also reported ICC values of 0.99 for the three components (BMC, FM and LM).
Based on the protocols, study objectives and characteristics such as quality control, reliability and valuation measures, the DXA may be considered as one of better methods to determining the values of FM, LM and BMC, and also one advanced and cost-effective technology that is useful for data acquisition of body composition in clinical trials of short to medium term, since its limitations are considered when planning the stages of an intervention 16,17.
Thus, regardless of the characteristics of the populations evaluated, DXA has shown good reliability, with high ICC and low CV 11,12,14, as observed in our study. These results allow us to consider the DXA as a method for assessing total body composition with precise and consistent results at different times of evaluation.
Little has been done to evaluate the intraobserver reproducibility of measurements of the ROI in DXA, especially since most studies assessing the reproducibility of this method were based in automatic measurements performed by the device. Thus, this study presents an unprecedented contribution to the scientific literature by evaluating the reproducibility of measurements intra analyzed for the 16 ROI, in which higher ICC values were obtained (between 0.952 and 0.999), indicating an excellent measurement reliability of this method for all body regions.
Similarly, the study by Buckinx et al. 10, which aimed to evaluate the correlation between the bioelectric impedance and DXA (Hologic QDR Discovery) for assessment of body composition in 138 Belgian adults, found an intraobserver reproducibility also high [ICC = 0.89 (0.86 to 0.92) for the total sample], although presented lower values than the ones of this study. However, Buckinx et al. 10 did not determine the reproducibility of measures for body segments; neither established which procedure used to define the ROI in the members. The ICC is a statistical calculation that can be used to indicate reliability or reproducibility between two measurements for the same evaluator. The more ICC approaches 1, the higher the precision or reproducibility, thereby resulting in equal values of 0.90 or superior can be regarded as very high, values between 0.70 and 0.89, can be regarded as high and values between 0.50 and 0.69, as moderate 18. In this sense, the values found in this study indicate an intraobserver agreement very high for the definitions and readings of the measures, regardless of the region scanned and region size.
Thus, it is possible to consider that in measurements TBM, FM, LM and BMC, the DXA has very high reliability. In this study, for the 16 ROI analyzed, was also obtained a high intraobserver reproducibility, which indicates a high reliability for both measures, for the instrument and the observer.
This study presents a possible limitation for evaluating only a sample of men, once sex can influence body composition 19,20 and that the amount of fat may involve greater variations in measurements of DXA (Valentine et al., 2008). However, we opted for this strategy in order to minimize a possible influence of factors related to the female gender, as the menstrual cycle, in the body composition. Future researches should establish the possible differences in segmental body composition between genders.
Based on the results of this study, we can conclude that the calculations performed with DXA in young people show a high reproducibility for both, TBM and FM, LM and BMC. In addition, the definition of specific body segments, the ROI, performed by a single observer, presents high reproducibility in both large and small segments.

