










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Monitoring physical fitness is a powerful indicator of health condition in childhood, adolescence and adulthood 1. Although all the clinical manifestations usually appear in adulthood, the etiologic commencement of the disease seems to occur in childhood 2. In this regard, a higher physical fitness level in children has been associated with more positive health-related outcomes, regarding the present and future risk for obesity, cardiovascular disease, skeletal health, and even mental health related to depression, anxiety, mood status and self-esteem 1,3.
Physical fitness can be objectively and accurately measured by laboratory methods, but due to their high cost, the necessity of sophisticated equipment and skilled professionals and time constraints, laboratory tests are still unable to be used at a population level. Conversely, field fitness tests are easy for administration and they include minimal equipment. In addition, they can test a number of respondents simultaneously and can be evaluated in a short period of time 4 5-6.
Although physical fitness is partially genetically determined, it can be significantly influenced by environmental factors such as physical activity 7,8. Unfortunately, children today are less likely to meet the minimum daily recommendations for physical activity 9,10. In addition, a clear-cut secular trend to higher body mass index and poorer levels of physical fitness among Macedonian children has been observed in the last decades 11,12.
Health promotion national policies should be therefore designed to promote health-related levels of physical fitness from childhood 1. Since all Macedonian children attend school, it may play an important role in public health and in the promotion of healthy behaviors such as encouraging children to achieve recommended levels of physical activity 1.
From the above, it can be concluded that the introduction of an organized system for monitoring physical fitness among children in educational institutions is an important national health problem 13. However, for the optimal interpretation of children's physical fitness levels, up-to-date reference values from a random and large representative sample of the studied population are required. Ortega et al. 13 recently proposed some reference values of physical fitness among European adolescents. Unfortunately, the level of physical fitness of children depends on several biological and environmental factors that vary among countries. Since the previous study was carried out on a sample of respondents (i.e., 3,428 adolescents from ten major European cities were arbitrarily selected and none of the Macedonian cities were included), these references are not valid for evaluation of the physical fitness levels of Macedonian children. In addition, the previous study did not provide the reference values for children under 13 years of age.
The present research was performed in order to determine the age and gender stratified reference values for health physical fitness for Macedonian children and adolescents, to identify significant gender differences, and to establish a single system for continuous and systematic monitoring of the students' health fitness at a national level called MAKFIT (Macedonian fitness meter).
MATERIAL AND METHODS
PARTICIPANTS
The research was conducted on a sample of 9,241 Macedonian children and adolescents, from 19 primary schools (eight rural and eleven urban) in Central and Eastern Macedonia. Briefly, data were collected by means of proportionate stratified random sampling taking into account the location (region) and the number of students by age and sex in each school in all mainland Macedonian administrative regions. The total number of children was divided into nine groups, according to chronological age (six years, seven years, eight years, nine years, ten years, eleven years, 12 years, 13 years, and 14 years), and each age group was divided in two subgroups according to the criteria of gender (subgroup n = 4,716 boys and subgroup n = 4,525 girls). The average age of the respondents of both genders was 10.02 years of age.
Anthropometry and fitness tests were assessed by trained doctors and Physical Education teachers in March, April and May 2012. Measurements were taken in standard school conditions as a part of Physical Education classes. Parents or a legal representative signed an informed consent form after being told about the purpose of the study. The study protocol was performed following the ethical guidelines of the Declaration of Helsinki of 1961 (revision of Edinburgh 2013).
ANTHROPOMETRIC MEASUREMENTS AND BODY COMPOSITION
Anthropometric measurements were taken according to standard methodology of the International Biological Program (IBP) and according to the recommendations of the World Health Organization (WHO) and Weiner-Lurie 25. Weight was measured in underwear and without shoes, with a medical decimal weight scale to the nearest 0.1 kg, and height was measured with the children barefoot in the Frankfort horizontal plane, with a telescopic height measuring instrument (Martin's anthropometry) to the nearest 0.1 cm. Body mass index was calculated as body weight in kilograms divided by the square of height in meters.
Components of body composition were assessed using bioelectrical impedance (measuring of the electric conductivity; bioelectrical impedance analysis [BIA]). The measuring was conducted with an OMRON BF511 body composition monitor, by means of which body weight, body fat percentage and muscle mass percentage were determined. Prior to the measuring, the parameters of gender, years, and body height of each respondent were entered in the body composition monitor. In order to provide highly precise results from the body composition assessment, we ensured that the preconditions recommended by ACSM and Heyward 14 were fulfilled prior to each measuring.
EVALUATION OF PHYSICAL FITNESS
Prior to starting the study, the researchers involved in the project undertook training sessions in order to guarantee the standardization, validation and reliability of the measurements 15. The fitness test battery is a set of valid, reliable, feasible and safe field-based fitness tests for the assessment of health-related physical fitness in children and adolescents, to be used in the public health monitoring system in a comparable way within the European Union 16. The systematic error when fitness assessment was performed twice was nearly 0 for all the tests 17.
Sit and reach test. With the subject seated on the floor and using a standardized support, the maximum distance reached with the tip of the fingers by forward flexion of the trunk is measured. This test is indicative of amplitude of movement or flexibility.
Hand grip test. With the use of a digital Takei® TKK 5101 dynamometer (range, 1-100 kg), the maximum grip strength was measured for both hands.
Standing broad jump test. The maximum horizontal distance attained, with feet together, was measured. This test evaluates lower limb explosive strength.
Bent arm hang test. A standardized test was used to measure the maximum time hanging from a fixed bar. This test assesses the upper limb endurance strength.
Thirty sec. sit-ups. Maximum number of sit-ups achieved in 30 seconds. This test measures the endurance of the abdominal muscles.
Shuttle run: 4 × 10 meters. This test provides an integral evaluation of the speed of movement, agility, and coordination. The subject does four shuttle runs as fast as possible between two lines ten meters apart. At each end the subject places or picks up an object (a sponge) beside the line on the floor.
Three-minute step test. The aerobic capacity was assessed by means of a three-minute step test. The respondent was supposed to get on and off a 30.5 cm high bench in four cycles (up, up, down, down), in a period of three minutes with a standardized rhythm of 96 beats per minute (bpm) dictated by a metronome. Heart frequency was measured prior to the test, and the children having submaximum value in terms of age in the stand-by state were not assessed by this test. Polar RS800 was used for heart frequency registration. Heart frequency values measured immediately after completion of the test and one minute later, as well as their average values, were taken as a result. The aerobic fitness test used in this study has been validated for use with adolescents 18.
STATISTICAL ANALYSIS
Statistical analysis, anthropometric and physical fitness characteristics of the study sample are presented as means (SD), unless otherwise indicated. Sex- and age-group differences were analyzed in the anthropometric and physical fitness variables by two-way analysis of variance. Paired t-test was used to compare means of distances performed in tests between boys and girls at the same age. Categorical data (weight status) were analyzed using the X2-test. A significance level of 5% was used for statistical testing.
To provide percentile values for Macedonian children and adolescents, physical fitness data were analyzed by maximum penalized likelihood using the LMS statistical method for boys and girls separately 19,20. Smoothed centile charts were derived using the LMS method. This estimates the measurement centiles in terms of three age sex-specific cubic spline curves: the L curve (Box-Cox power to remove skewness), M curve (median) and S curve (coefficient of variation). For the construction of the percentile curves, data were imported into the Lms Chartmaker software v. 2.3 (by Tim Cole and HuiqiPan) and the L, M and S curves were estimated. Except for the LMS method calculations, the SPSS v. 22.0 software for Windows (SPSS, Chicago, Illinois, USA) was used and values of p < 0.05 were considered as statistically significant.
RESULTS
The results of anthropometric indicators and tests for assessing the level of physical fitness in terms of gender and age are presented in Table 1. From the review of the table it can be seen that boys show better results (p < 0.000) in all tests for assessing the level of physical fitness, except in the sit and reach test, where girls show better results. Generally, the anthropometric characteristics and the level of physical fitness increase with age.
Table I. Characteristics of the study sample by sex
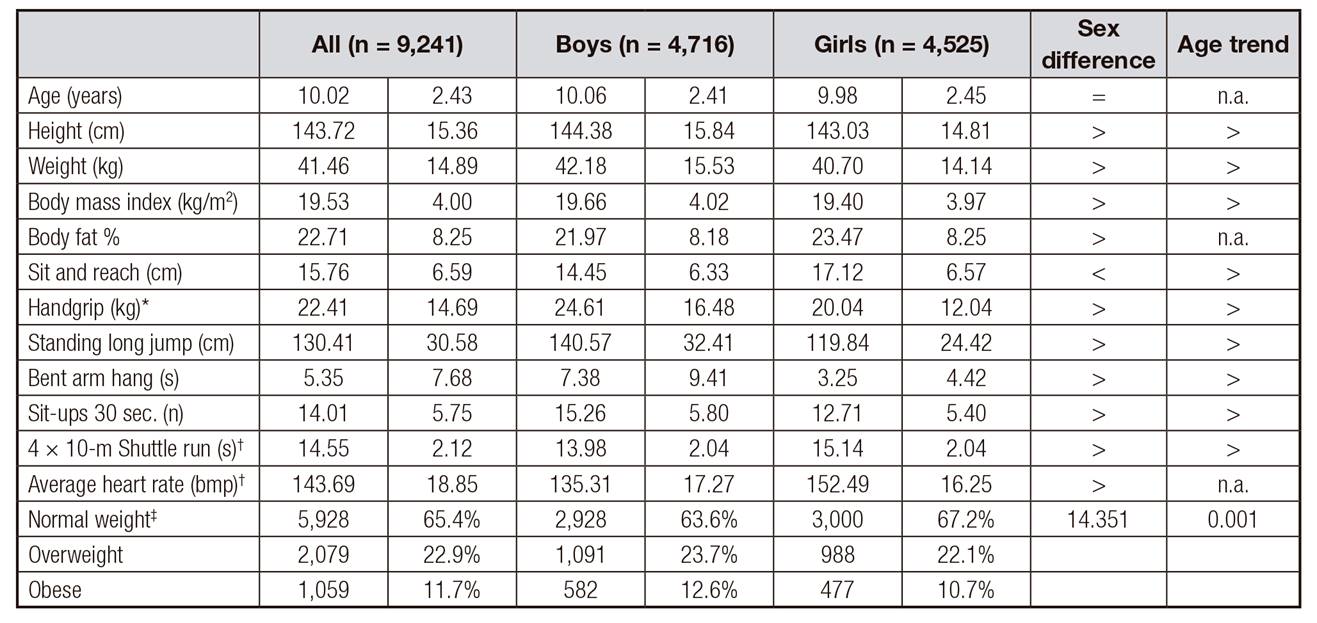
Data are shown as mean (SD), unless otherwise indicated. Sex and age differences were analyzed by two-way analysis of variance, with sex and age group as fixed factors, and anthropometric or physical fitness measurements as dependent variables
*Values are expressed as average of right and left (hand) scores.
†Lower values indicate better performance.
‡The respondents were categorized according to the international gender and age-specific BMI (kg/m2) cut-off points (Cole et al., 2000 and 2007 29,30; p < 0.010 for the difference between boys and girls (Chi-square tests). The symbol > in the "sex difference" column means the variable is significantly (p < 0.05) higher in boys than in girls; < means the opposite; and =, the non-significant differences. Likewise, the symbol > in the "age trend" column means the variable tends to increase by increases in age; < means the opposite; = means non-significant differences. n.a.: not applicable.
From the review of the table it can be seen that 65.4% of Macedonian children and adolescents have normal weight, 22.9% are overweight and 11.7% are obese. Values of the X2 test (X2= 14.351, p = 0.001) indicate that there are statistically significant differences in the level of nutrition between boys and girls. The percentage values show that a higher percentage of boys present moderately high and high BMI (obese).
Table 2 Table 3, Table 4, Table 5, Table 6, Table 7, Table 8, Table 9, Table 10 show the normative values of tests for assessing the level of physical fitness of Macedonian children and adolescents in terms of gender and age, expressed as 5. to 95. percentile. Figure 1 and Figure 2 display the polished percentile curves (P5, P10, P25, P50, P75, P90, P95) for tests for assessing the fitness according to age and gender. The data on the graph clearly show a slight increasement of ability with increasment of age.
Table II. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Body mass index (kg/m2)

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation. L: skewness; M: median; S: coefficient of variation.
Table III. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Body fat percentage (%)

Centile values were estimated by using LMS method for exact ages. SD: standard deviation. L: skewness; M: median; S: coefficient of variation.
Table IV. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Speed/agility: 4 × 10-m shuttle run test (s)

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.
Table V. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Upper-limb maximal strength: handgrip strength test (kg)

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.
Table VI. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Flexibility: sit and reach test (cm)

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.
Table VII. Tabulated physical fitness centile values by sex and age groups in Macedonian children and adolescents. Upper-limb endurance strength: bent arm hang test (s)

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.
Table VIII. Tabulated physical fitness centile values by sex and age in European adolescents. Lower-limb explosive strength: standing long jump test (cm)
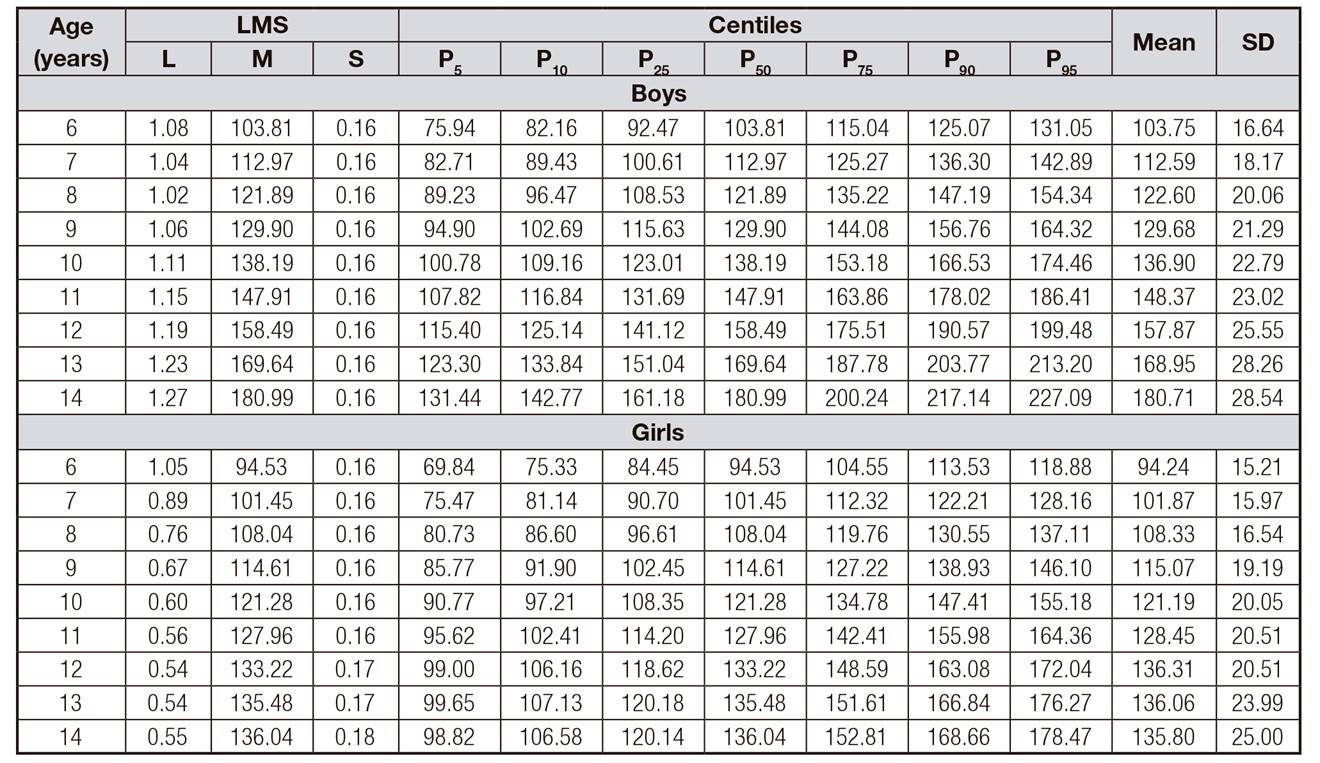
Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.
Table IX. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Abdominal strength: sit-ups 30 sec.

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.
Table X. Tabulated physical fitness centile values by sex and age in Macedonian children and adolescents. Cardiorespiratory fitness: average heart rate (bmp)

Centile values were estimated by using the LMS method for exact ages. SD: standard deviation; L: skewness; M: median; S: coefficient of variation.

Figure 1. Percentile curves (from bottom to top: P5, P25, P50, P75, P95) of nine tests to measure different fitness components. The smoothing of the percentiles was done with the LMS method (boys).

DISCUSSION
Physical fitness is today considered to be a strong marker of the health and quality of life in childhood 1,2, highlighting the need for a widespread physical fitness assessment among children 10. Unfortunately, in many countries the importance of monitoring physical fitness as an important diagnostic tool for determining the health status of children is most often overlooked 21.
In addition, the proper interpretation of the level of physical fitness requires comparison of the results obtained with a particular child with reference values of the same sex and age population. In this context, the study provides gender and age-specific percentile values for eight commonly used field-based physical fitness tests in a random and large national representative sample of Macedonian children aged six to 14 years.
Schools are the most appropriate places to identify children with low levels of physical fitness and to promote healthy behaviors 1. Hence, these reference values represent an undoubtedly important tool in the educational environment. The results of this research will allow Physical Education teachers to detect children with health problems early and begin immediate intervention. For instance, scores below the 5th percentile should be taken as a "warning signal" due to the potential pathology of children scoring them. Therefore, these children should undergo a clinical evaluation of the coexistence of other risk factors that may cause future diseases (e.g., decreased muscle AMP deaminase because of C34T mutation of the gene AMPD1) 22, and they should be encouraged to follow a healthier lifestyle, for example, engaging in recommended daily levels of physical activity, reducing time in sedentary activities or following a healthy diet. Then, the effect of intervention on the level of the child's physical fitness could be observed by following the evolution of percentile lines through the years.
Furthermore, the percentile values provided in the study could represent two additional contributions. From the standpoint of prevention, the obtained reference values will enable the diagnosis and detection of those physical fitness components in children who present the worst values (for example, under the 10th or 25th percentile) and be susceptible to improvement with an appropriate physical exercise program 20. On the other hand, current reference values can be used by Physical Education teachers and coaches to identify sports talents. In this sense, children who score over the 90th or 95th percentile should be considered as talented for those sports for which that particular physical fitness component is relevant.
The results of the survey show a higher level of physical fitness in boys than in girls of all ages, with the exception of flexibility (sit and reach test), where girls have achieved better results. These differences have increased with age. Furthermore, there was a trend towards increased physical fitness levels as the age increased in both boys and girls, although girls generally reached the plateau when 13-14 years old, while boys' values continue to increase. Previous studies have shown similar results. For example, studies on European children and adolescents have shown that boys are better in cardiorespiratory fitness 13,21 22-23, muscle strength 13,22,24,25 or speed 13,22,26. However, the same studies have shown that girls in all adult categories achieve better results in flexibility assessment tests 13,26,27. The reason why girls achieve better results in the sit and reach test may be the differences in the level of growth and development of the connective, muscle and bone tissue, as well as the difference in the anatomy of the hip joint and pelvis between boys and girls 28,29,38. Additionally, the same studies found a plateau approximately at the same ages. Gender differences in adolescence in combination with the effects of the endocrine adaptation (influence of gonadal steroid hormones and the growth hormone) typical for sexual maturation, morphological differences, mainly the body composition (for boys, the content of minerals in the bones and muscle mass increases and fat deposition around the hips decreases), functional differences and physical activity are the main factors for the differences in the level of muscular fitness in adolescence between boys and girls 31,32.
However, the question is, why in early school age there are differences in the level of fitness between boys and girls? Perhaps the reasons for these differences are more sociological than biological. Environmental factors (social interests, peer influence or lack of motivation towards physical activity) unequivocally encourage girls to be less active than boys. Increasing muscle mass until puberty is a consequence of the effect of "insulin similar to the growth hormone IGLF-1", which has the same effect for boys and girls during and after puberty. The increase of muscle mass is due to the effect of the testosterone hormone.
According to our results for the different levels of fitness abilities between boys and girls, there is a need for a differentiated approach in the Physical Education class in terms of adjustment of physical activity based on gender, level of fitness abilities and students' needs and interests.
Except for the cardiorespiratory fitness test (three-minute step test), the EUROFIT fitness test battery was selected in this study because it is probably the most extended, validated and standardized method for assessing children's physical fitness in Europe 33. However, some methodological problems were found. Similarly to previous studies 13,25, a substantial number of children that scored 0 in the bent-arm hang test (27.9% boys and 36.9% girls) was observed. Although there are definitely some differences in physical fitness among these children that failed, the test was unable to discriminate them. Therefore, its usefulness and future use in children is questionable.
Comparing the international studies with the results obtained in our study, it can be concluded that Macedonian students from both genders achieve lower scores on average in the "30 sec. sit-ups" and "sit and reach" tests at the ages of eleven and 14 in terms of peers from Serbia, Belgium, Italy, Spain, Lithuania, Latvia and Estonia 34 35 36 37 38-39. Male and female students from Macedonia achieve lower results on average in the test "standing broad jump" at the ages of eight and eleven, and better results at the ages of 12 and 14 when compared to students from Hong Kong 40. Macedonian male and female students achieve similar results at the age of 13 and 14 in the "standing broad jump" test in relation to previous researches performed on adolescents from Spain measured by the AVENA study 41. Macedonian boys at the age of 13 and 14 achieve better results on average in the "standing broad jump" test compared to European male peers measured in the HELENA study 13. On the other hand, Macedonian 13 and 14-year-old girls achieve worse results in the "standing broad jump" test compared to same age European female adolescents measured by the HELENA study. Macedonian boys at the age of 13 and 14 achieve better results on average, and the girls achieve similar results in the "hand grip" test in comparison with their European peers measured by the HELENA study, and 13 and 14-year-old Macedonian students of both gender achieve lower results on average in the test compared to adolescents from Spain measured by the AVENA study. Six and ten-year old Macedonian students from both genders achieve better results on average in the "hand grip" test compared to their peers from Portugal 42 and Latvia 34, while adolescents at the age of nine to 14 achieve lower results on average than their peers from Australia 43. In the "shuttle run 4 × 10 meters" test, male and female Macedonian students at the age of 13 and 14 achieve lower results on average than their European peers measured by the HELENA and AVENA studies, and they achieve lower results on average at the age of six to ten than their peers from Portugal 42.
This study has some limitations. Firstly, due to its cross-sectional nature we cannot discern the direction of the observed associations between physical fitness and future cardiovascular risk, which may indeed be reciprocal. Secondly, important variables associated with blood lipids such as levels of physical activity, sex hormone levels, and familial health background were not measured. In addition, the weakness of the survey was the selection of the sample, which did not represent the entire population of children and adolescents from Macedonia, since it did not include respondents from the western part of the country or respondents from ethnic communities. The advantage of this research is the large sample included, strict field-based standardization and the large expert team of kinesiologists and doctors who carried out the research in order to avoid bias due to inconsistency in the measurement protocols.
CONCLUSION
In summary, indigenous boys showed better results than girls in cardiorespiratory fitness, lower- and upper-limb strength and speed/agility and girls performed better in low back flexibility. The results obtained can be used to identify children and adolescents at higher risk for developing unfavorable health outcomes owing to their low fitness level (< 10th percentile). Also, these cut-offs are especially interesting in educational settings because schools can play the main role in identifying children with a low level of physical fitness. At the same time, this research provides a precise categorization, which considers a youth age and gender, and enables comparisons among normative values from other countries. In addition, they are important because monitoring health-related physical fitness early in life might contribute to substantial improvements in life expectancy and reduced risk of chronic diseases such as obesity, cardiometabolic disease, skeletal and mental health in the indigenous population.

