










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Eating disorders (ED) are one of the most important public health problems (1), representing a burden not only for patients but also for their families and society, due to their associated high economic and health care costs (2,3). EDs often become chronic disorders and can persist for long periods of time (4), being responsible for high morbidity and higher mortality among all psychiatric disorders (5). These disorders are characteristic of behavioral syndromes related to physiological and physical alterations (3), and are due to various factors, such as genetic, psychological, and sociocultural factors (6). Gender is a very important factor in the occurrence of ED; women are more likely to suffer from ED when compared to men; in fact, approximately 80 to 95 % of those affected are women (7-9). Despite this widespread perception that eating disorders predominantly affect women, there is growing evidence that the incidence and prevalence rate among men is increasing (10). During the last two decades, a dramatic growth in the prevalence of ED among men has been observed (11).
In several studies, the self-reported Eating Disorder Examination Questionnaire (EDE-Q) has been used to assess eating disorder symptoms. This instrument is used to assess attitudinal (weight concerns) and behavioral (binge eating) symptoms (12). In addition, it has been used in clinical and nonclinical populations (13). There are several versions of the EDE-Q; among them, the 7-item EDE-Q, which is composed of three scales that include 1) dietary restriction; 2) overestimation of shape/weight; and 3) body dissatisfaction (12). This version allows for a reduction in administration time and could provide a measure with sound psychometric properties for use in clinical and community samples in both men and women (14).
Network models offer an alternative perspective in the evaluation of psychological measures without necessarily considering a common latent variable. This approach represents the associations (edges; total or partial correlations) by using a Gaussian graph, whose thicknesses are proportional to the intensity of the correlation between the elements of the instrument nodes (15,16). In addition, it includes centrality indices that quantify the strength of the components within the network (17).
Network analysis in the research of psychological disorders is receiving increasing attention in all fields of study (16). Its use in the evaluation of the EDE-Q is denoted as an emerging system, given the interaction of the indicators with each other, which together form the construct. Such indicators are not simply caused by a common latent variable as in factor models, but direct interactions between item responses form the dynamic structure of eating disorder development. Specifically, it is possible that there is no causal variable for the occurrence of dietary restraint, body overvaluation, or body dissatisfaction (18). It is more likely that the development of ED arises as a result of interactions between these factors or their respective items (16).
It is important to evaluate these psychopathological aspects considering the gender factor, given the differences between body ideals and body image concerns (13,16). This allows us to explain which measures reinforce such sex differences in EDE-Q7, considering that there is evidence of a steady increase in the prevalence of ED in men recently (10,11). However, there are controversies in the differential characteristics in the manifestation of eating disorders between men and women; while some studies report a tentative increase in the incidence and prevalence rate of ED in men (19,20), other studies report higher levels of dietary pathologies in women (21,22). These divergent results may be related to greater emotional problems such as depression (23), which favors an increase in scores related to body dissatisfaction.
The exploration of simultaneous EDE-Q7 network structures is particularly important to evidence how higher-risk psychopathological symptoms interact with the emergence of ED in males and females, given that to date no ED-related network studies have yet been reported in South American populations. Therefore, the aim of the study was to explore the patterns of association of the components of the EDE-Q7 according to gender using two simultaneous network models in Peruvian adults.
MATERIALS AND METHODS
PARTICIPANTS AND STUDY DESIGN
A cross-sectional quantitative study was carried out using a Gaussian graphical model (partial correlation coefficient network). To evaluate the dynamic relationships of the EDE-Q7, a group of 890 Peruvian adults (63.51 % were women; mean age: 26.40) was considered using non-probabilistic convenience sampling. Approximately 70 % were university students, 25 % were high school level, 5 % were elementary school level. Additionally, 70 % lived in Lima, while 17.7 %, 6.3 %, and 6 % were from Trujillo, Arequipa, and Huancayo, respectively. Google Forms was used to share the questionnaire publicly through email and social networks such as WhatsApp and Facebook Messenger. Data were collected between May and August 2021. Foreigners and those under 18 years of age were excluded. Informed consent was obtained from those who voluntarily decided to participate in this study. To carry out this study, the ethical standards stipulated in the Declaration of Helsinki were considered. In addition, the study was reviewed and approved by the research ethics committee of Universidad César Vallejo.
EATING DISORDER EXAMINATION-QUESTIONNAIRE
The Eating Disorder Examination-Questionnaire was used considering the 7-item Spanish version (24) (Table I) because it has stronger evidence of reliability and validity than the original measure (14). This measure predicts a series of basic behavioral characteristics of eating disorders, being a Likert-type scaling measure with seven options. Reliability was obtained by the general Cronbach's alpha measure of 0.83.
Table I. The Eating Disorder Examination-Questionnaire.

Note:Spanish version of the EDE-Q7 according to Grilo et al. (24).
STATISTICAL ANALYSIS
Two Gaussian graphic models (networks of partial correlation coefficients) were calculated for men and women from the seven items of the instrument using the R qgrap package and the LASSO fused graph (25), which allows us to graphically explore the patterns of the interactive system of symptoms of the EDE-Q7 according to gender. This network approach is more reliable than bivariate analysis because it eliminates illegitimate relationships and fixes independent relationships beyond the other connections (26), considering the 5000-sample bootstrap method to reinforce the stability of the network results. To determine the level of network connections, the interpretation of effect size values (≤ 0.1 = small; > 0.1 to < 0.5 = moderate; ≥ 0.5 = large) was considered. In addition, the strength centrality index was reported as a measure that quantifies the importance of network association magnitudes (26).
Finally, the R package Network Comparison Test (NCT) was used to assess differences in network structure (assess that the structure of both networks is equal), overall strength and borders (equality in overall connectivity and between the borders of both networks) in men and women.
RESULTS
More moderate-sized connections (13) were found in the women's network (Fig. 1A). In this group, a higher measure of strength (1.27) is reported for item EQ7 (dissatisfaction with body image), which presents a greater interaction with item EQ4 (overvaluation of weight), integrating the two factors of relative closeness and superior connectivity compared to the diet restriction dimension. These items are more reinforced in the EDE-Q7 network of women, for example, the dynamic link “EQ4-EQ6” of body image overvaluation and weight dissatisfaction is more reinforced in this group compared to men. In addition, the relationship of “EQ1-EQ2” (partial r = 0.33) stands out, which, together with the other connections mentioned above, drives a better dynamic that activates the operation of the other components of this network. Likewise, the relationship between dietary restriction in the male network model was noteworthy (partial r = 0.38).

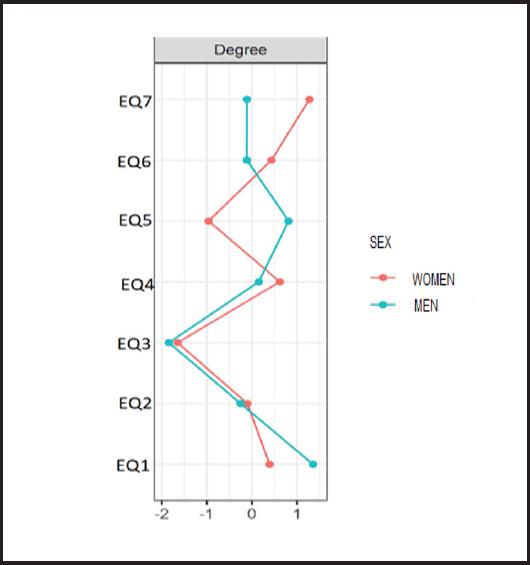
A difference of interest is visualized in the male network (Fig. 1B) in the “EQ1-EQ5” relationship (partial r = 0.27) between the dimension's weight overvaluation and diet restriction, where both items present a higher strength index (1.34 and 0.81) in males compared to females (Fig. 2). In other words, there is a higher prevalence of dietary restriction in men, while in women the measure of dissatisfaction with body image stands out. Assessment of networks for men and women using the NCT showed no differences in network structure (p = 0.07) or overall strength (p = 0.06). Because the network structure was found to be invariant, the strengths of individual connections were not tested.
DISCUSSION
The EDE-Q7 is one of the instruments most used to evaluate measures of higher risk to develop an eating disorder (14). This study was conducted in response to concerns about the non-utilization of the eating disorders network in the Latin American context. To our knowledge, this is the first study that evaluates through the network approach the EDE-Q7 measure that presents components such as dietary restriction, overvaluation, and dissatisfaction about weight and body image in males and females.
According to the NCT measure, the dynamic network evaluation suggests that the DTS-Q7 systems for women and men shared most borders and network characteristics; however, some descriptive differences were found; for example, based on the strongest connection in both networks, EQ1-EQ2 can be considered as one of the multiple possible routes for connecting the other network elements. One of the possible connectivity routes that involve those measures of greater centrality in the network of women indicates 5 elements (EQ1-EQ2-EQ4-EQ6) that represent the three domains of the EDE-Q7, unlike men (EQ1- EQ2-EQ4-EQ5) that identify only two subscales: diet restriction and body overestimation.
Such findings suggest variations in the weight dissatisfaction dimension (more prevalent in women) and the body image dissatisfaction dimension (EQ7), which are the most central in the female network. Both items are part of the body dissatisfaction subscale. This could explain the fact that there is a greater psychological vulnerability in ED development in women compared to men. These results are supported by recent research findings that included the EDE-Q7 measures, where women reported a lower level of caporal appreciation compared to men (21). However, these results are contrasted by a study that reported higher score differences on the EDE-Q subscale in favor of women (22). On the other hand, Wang and colleagues assessed binge eating disorder in males and females through the network approach, finding a greater central importance in the two body dissatisfaction items (27). Another recent network study in the South American context demonstrated a higher measure of strength in weight dissatisfaction (ED6) in men and women, but this measure was more prevalent with higher levels of psychological distress and stress by COVID-19 (28). However, another network study conducted in men found a higher centrality of the body image devaluation symptom, however, weight devaluation was not influential in this network (16), which is contrary to the findings reported in the current study. Therefore, the implementation of ED prevention and health promotion programs in males is necessary.
The network results obtained from the current study show simultaneous statistical interactions after partializing the effects of the other network relationships. In this sense, this dynamic model applicable to instruments related to health and behavioral sciences is novel. It is also possible to integrate the results of self-report measurements or other clinical measurements, such as physiological, biochemical, anthropometric, psychiatric, and others (15,29), for the integral evaluation of the functioning and interaction of various aspects linked to different health conditions, such as arterial hypertension (30), pathology considered as one of the risk factors in mental health (31,32).
Moreover, it is possible to identify and group the variables with the highest probability of connection, these measures present an underlying latent characteristic in the structure of the network, considering the example of an exploratory graphical model reported by Ramos-Vera (33) where the relationships of depressive symptomatology in patients with arterial hypertension were grouped into two dimensions of emotional and somatic nature based on network clustering algorithms and factor analysis.
The burgeoning methodology of network analysis of statistical relationships has had some questioning about its statistical replication in binary models (37), which has been contested by (34). Regarding its use in polytomous variables, it has presented greater replicability by previous authors, but like any new methodology, it usually presents some points to discuss. It is also a method under development, which currently has statistical replication techniques (35) for the robustness of health and behavioral science research that allows evaluating new clinical hypotheses in eating disorders (36). It is also possible to evaluate the Bayes factor to weigh the evidential strength of the statistical relationships of the network (37,38) or to estimate the degree of evidence of the comparative hypotheses according to sex or other conditions of interest (39).
The results of this article from the network approach have a favorable clinical implication to direct intervention and treatment of eating disorders (40); in addition, it can be oriented to complement instrumental and correlational investigations to reinforce the inferential property of such more comprehensive conclusions for decision-making in clinical studies that may affect people's health.
LIMITATIONS
The current study has several limitations. First, the data were collected by non-probability convenience sampling (mostly female participants). In addition, the results were self-reported, which obviously limits the generalizability of the findings to other populations. Furthermore, it is important to consider that this is a cross-sectional design and therefore direct causality cannot be inferred. Finally, the data were collected during the health crisis caused by COVID-19, which could affect our results, being that COVID-19 could behave as a confounding variable affecting eating disorders.
CONCLUSION
This study that evaluated two simultaneous network models of EDE-Q7 by sex in Peruvian adults presented evidence of invariance in both structure and connection magnitudes using the network model. However, descriptive differences were found in the central network measures. In fact, in women, it was evident that the dimension of dissatisfaction with body image presented a greater network centrality. However, in the case of males, a higher central prevalence of network in the dietary restriction dimension was highlighted. Such findings allow us to explain the possible variations in the activation of factors of greater risk in the development of ED according to the gender of greater psychological vulnerability in Peruvian adults.

