










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
There is evidence that ergogenic aids and the correct application of training loads induce better physiological responses and adaptations in athletes (1). Specifically, these ergogenic aids are a relevant factor in increasing the physical performance of athletes (2). Beta-alanine (BA) is among the most widely used ergogenic aids in sports (3,4). History shows that athletes have been ingesting BA to increase physical performance for several years (5,6). This ergogenic aid is based on extensive scientific support (5,7). Specifically, BA is a non-proteogenic amino acid (aa) produced endogenously in the liver. In addition, humans acquire BA by consuming poultry and meat. One of the effects of BA intake is increased intramyocellular carnosine (CA) levels (8). It increases the capacity to buff the muscle's hydrogen ions (H+) (buffer effect). In this context, the buffering capacity of CA allows the stabilization of intramyocellular pH during high-intensity exercise, delaying the onset of fatigue (9).
Concerning the methods of BA intake in athletes, there are two forms of supplementation: one of extended duration (chronic) (10) and one of short duration (acute) (2). In this regard, it has been shown that most research has evaluated only the chronic effect of supplementation with BA on physical performance (8,11). Most of the studies that have reported an increase in physical performance have supplemented under the doses established in the position stand for tests—between 1-4 minutes (min) in duration, with a dose between 4-6 g·day-1 of BA for 2-4 weeks (3). However, despite the existing evidence linking the use of BA to physical performance, information on the acute effect of BA supplementation on the heavy-intensity domain zone (HIDZ) is scarce (2,4,12).
At the same time, the perceived exertion (RPE) rating is one of the most widely used tools for intensity control in exercise and sports sciences (13). It is a fact that through RPE, athletes can manifest fatigue perceived during exercise (14). However, for this scale to increase its reliability, it must be trained during all training sessions since the perceived effort is conditioned by multiple peripheral afferent signals that reach the brain. It is the latter organ that determines the sensation of fatigue (15).
Likewise, because it presents a high correspondence, RPE is used as a complementary or alternative measurement of physiological parameters (16), including maximum oxygen uptake (VO2max) (17), blood lactate (BL) (18), ventilatory thresholds, and heart rate (HR) (19). In addition, RPE allows quantification of exercise load (20), becoming an alternative to measure fatigue levels (21) and the state of post-exertion recovery (22). For example, a lower RPE value during exercise and post-training is associated with a possible metabolic adaptation of athletes (23).
Besides, the buffering effect of CA resulting from the intake of BA could cause a lower RPE during exercise and post-exertion recovery in athletes (on a scale of 1-20, 1 RPE point is equivalent to approximately ten beats per minute) (4). In this regard, some research has related the use of BA to the RPE (24,25). However, there is no history of using BA for maximal post-exertion recovery RPE in HIDZ. The HIDZ includes maximal aerobic speed (MAS) and VO2max (4) for this study. In this context and to the best of our knowledge, only the research presented by Huerta Ojeda et al. (2) has studied the acute effect of 30 mg BA·kg-1 on MAS performance. Specifically, in that study the researchers reported non-significant differences in term RPE when comparing the experimental group (EG) with placebo (PL) (p > 0.05), with no evidence of the post-exertion recovery RPE (2).
As has become evident, there is a conclusive history of chronic supplementation with BA and increased physical performance (26). However, the effect of acute BA supplementation on HIDZ is scarce and controversial, even more so on RPE (2,4,12). Despite this low evidence, and as previously described, a lower RPE value after acute supplementation with BA could be associated with a lower level of fatigue (4). However, considering the scarce information on this subject, it would be risky to assert this relationship. Therefore, this study's purpose was to determine the effect of acute BA supplementation, with low dose (30 mg·kg-1) and high dose (45 mg·kg-1), on the post-exertion RPE, HR, and BL in middle-distance athletes and to determine the effect of acute BA supplementation on physical performance on the 6-minute race test (6-MRT).
MATERIALS AND METHODS
PARTICIPANTS
Twelve male middle-distance athletes volunteered to be part of this study (age: 21.8 ± 2.37 years, weight: 69.8 ± 4.36 kg, height: 174.8 ± 5.45 cm, body mass index [BMI]: 22.8 ± 1.63 kg·m2, body fat percentage: 9.3 ± 2.62 %). The inclusion criteria were: a minimum of two years of experience in middle-distance events, with knowledge of the RPE and familiarization trial with the 6-MRT. The exclusion criterion was the inability to perform the 6-MRT. Statistical software (G*Power, v3.1.9.7; Heinrich-Heine-Universität, Düsseldorf, Germany) was used to calculate the sample (27). The combination of tests used in the statistical software to calculate the sample size was as follows: a) F test, b) ANOVA: repeated measures, within factors, and c) a priori: compute required size - given α, power, and effect size. Tests considered effect size f = 0.4, α-error < 0.05, power (1-β error) = 0.8, number of groups = 1, number of measurements = 3, correlation among repeated measures = 0.5 and non-sphericity correction = 1; the total sample size was 12 participants. All participants were informed of the aim of the study and the possible risks of the experiment. All subjects signed the informed consent before the application of the protocol. The study protocol and the informed consent were approved by the Ethical-Scientific Committee on Human Research of Universidad de Las Américas, Chile (registration number CEC_PI_2020005) following the ethical standards for exercise and sport sciences (28). This study was registered at ClinicalTrials.gov with identifier: NCT05096793.
ANTHROPOMETRIC MEASUREMENTS
Height (cm) was evaluated with a stadiometer from the feet to the vertex (Frankfort plane). Weight (kg) was assessed using a Tanita Inner Scan BC-554® digital scale. Weight and height were assessed with barefoot, shorts, and a light T-shirt. BMI was measured according to anthropometric standards to assess nutritional status (29).
RESEARCH DESIGN
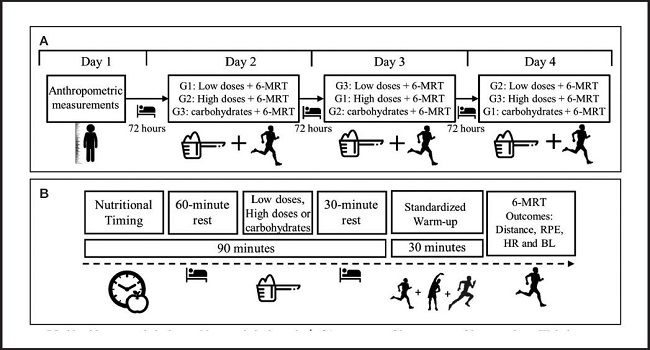
The research had a quasi-experimental, intrasubject, double-blind, crossover study design. The study, including all assessments, was conducted within one week. All participants (n = 12) were asked to refrain from ingesting protein, caffeine, energy supplements, or any substance that would increase metabolism during the entire intervention week before the experiment. On day one of the intervention, anthropometric measurements were taken. Then, the 12 participants were divided into three subgroups of four participants each: group 1 (G1, n = 4), group 2 (G2, n = 4), and group 3 (G3, n = 4). On day two, all groups performed the first 6-minute race test (6-MRT): G1 with a low-dose BA (30 mg·kg-1), G2 with high-dose BA (45 mg·kg-1), and G3 with fast-absorbing carbohydrate PL (30 mg·kg-1). On day three, all groups performed the second 6-MRT: G1 with a high-dose BA (45 mg·kg-1), G2 with fast-absorbing carbohydrate PL (30 mg·kg-1), and G3 with low-dose BA (30 mg·kg-1). On the fourth and last day, all groups performed the third 6-MRT: G1 with fast-absorbing carbohydrate PL (30 mg·kg-1), G2 with low-dose BA (30 mg·kg-1), and G3 with high-dose BA (45 mg·kg-1). Subgroups were evaluated at the same time during all interventions (G1: 09:00 a.m., G2: 09:30 a.m., and G3: 10:00 a.m.). The evaluations were separated by 72 hours. This time allowed a BA washout to be generated between evaluations (8,30). Also, participants did not exercise between assessment days (Fig. 1A).
LOW BETA-ALANINE DOSE
The high dose consisted of acute supplementation with 30 mg·kg-1 of BA dissolved in 500 mL of distilled water. This supplementation was performed after 60 minutes of nutritional timing and 60 minutes before 6-MRT (Fig. 1A).
HIGH BETA-ALANINE DOSE
The low dose consisted of acute supplementation with 45 mg·kg-1 of BA dissolved in 500 mL of distilled water. This supplementation was performed after 60 minutes of nutritional timing and 60 minutes before 6-MRT (Fig. 1A).
PLACEBO
The PL consisted of ingesting 30 mg·kg-1 of rapidly absorbed carbohydrates dissolved in 500 mL of distilled water. This intake was performed after 60 minutes of nutritional timing and 60 minutes before 6-MRT (Fig. 1A).
NUTRITIONAL TIMING
In order to avoid the presence of paresthesia, all participants were given a pre-exercise snack (2,4,12). The snack consisted of a carbohydrate load before the 6-MRT. For this purpose, all athletes were available to the researchers two hours before the tests under fasting conditions. The nutritional timing consisted of 2 g of rapidly absorbed carbohydrates per kg of body weight (2 g·kg-1) (Fig. 1B).
STANDARDIZED WARM-UP
The standardized warm-up for all 6-MRT runs consisted of 10 minutes of jogging, five minutes of lower extremity ballistic movements (adduction, abduction, hip flexion and extension, and knee and ankle flexion and extension), and three 80-meter accelerations (Fig. 1B).
SIX-MINUTE RACE TEST
The 6-MRT is a maximal effort test aiming to estimate MAS in athletes. The test consists of covering the greatest possible distance in 6 minutes (31,32). The development of this test was performed on a 400-meter athletic track. Before the evaluation, the participants were instructed to cover the greatest possible distance in the 6 minutes the test lasted. During the test, participants received verbal incentives from the researchers. At the end of each 6-MRT, the distance covered in meters (m), RPE, HR, and BL were assessed.
RATING OF PERCEIVED EXERTION
The RPE was used to assess the intensity of the physical effort made by the subjects, which was evaluated through the modified Borg scale (1 to 10), where 1 was a very light effort, and 10 was a maximum effort (14). The RPE was evaluated immediately after 6-MRT and post-exertion (min 1, min 3, min 5, min 7, and min 9).
HEART RATE
A Polar Team® brand heart rate monitor was used to determine the HR per minute, while this data was stored through the Polar Beat® application. HR was assessed immediately after 6-MRT and post-exertion (min 1, min 3, min 5, min 7, and min 9).
BLOOD LACTATE
For the measurement of BL, capillary blood samples were collected from the fingertip. For this purpose, a lactometer (h/p/cosmos®) was used, which generates an enzymatic-amperometric lactate detection with an accuracy of ± 3 % (minimum standard deviation of 0.2 mmol/L-1), a sample volume 0.2 µL and with a measuring range of 0.5-25.0 mmol/L-1. BL was evaluated immediately after completing 6-MRT and post-exertion (min 1, min 3, min 5, min 7, and min 9).
STATISTICAL ANALYSIS
Descriptive statistics were used to express the mean values, and standard deviations (SD) of the variables studied. The Shapiro-Wilk test was used for the normal distribution of the results. Comparison of RPE, HR, and BL at the end of 6-MTR, post-exertion min 1, min 3, min 5, min 7, and min 9, in addition to the 6-MRT performance (m) among the three conditions (low dose, high dose, and PL), was performed by repeated-measures ANOVA. This analysis was complemented with a post hoc through Tukey's multiple comparisons tests.
The analysis of RPE, HR and BL was performed for the three conditions independently (low dose, high dose, and PL) at the end of the 6-MRT, min 1, min 3, min 5, min 7, and min 9 post-exertion, was performed by one-way repeated-measures ANOVA. This analysis was complemented with a post hoc Tukey's multiple comparisons tests.
The association between the study variables for the two treatments and the PL, independently, was quantified through the Pearson's correlation coefficient (r) and according to the following scale: trivial (0.00-0.09), small (0.10-0.29), moderate (0.30-0.49), large (0.50-0.69), very large (0.70-0.89), almost perfect (0.90-0.99) and perfect (1.00) (33). All other statistical analyses were performed with the Prism version 7.00 for Windows® software. The significance level for all statistical analyses was p < 0.05.
RESULTS
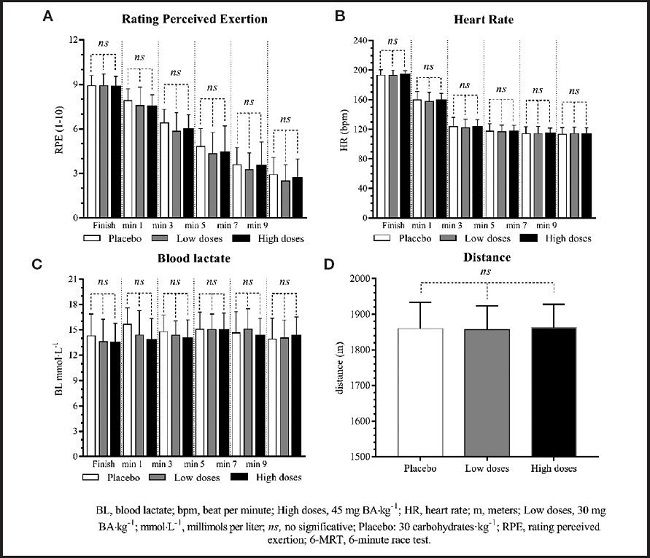
The first analysis showed a normal distribution (p > 0.05). The second analysis showed that the RPE, HR, and BL on the completion of the 6-MTR (post-exertion min 1, min 3, min 5, min 7, and min 9), in addition to the 6-MRT performance (m) among the three conditions (low dose, high dose, and PL), did not evidence significant differences (p > 0.05). The distances achieved in 6-MRT and RPE, HR, and BL post-exertion kinetics are reported in figure 2.
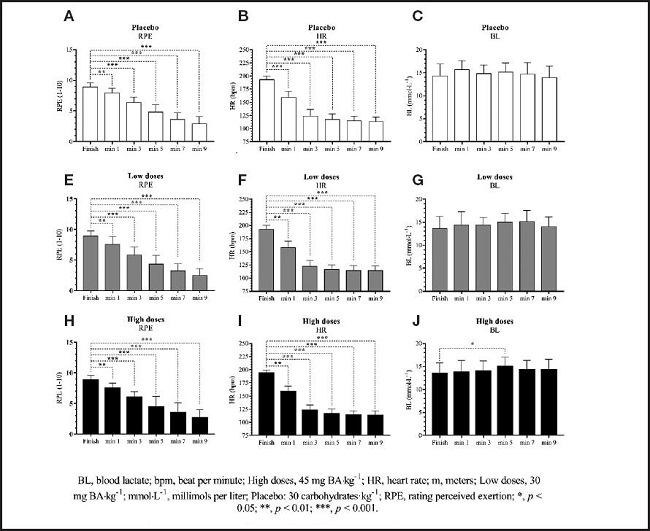
When analyzing the RPE and HR of the two treatments and PL, significant decreases were observed from the end of 6-MRT to min 9 post-exertion (p < 0.001). In parallel, only for the high dose there were significant increases in BL from the end of 6-MRT to min 9 post-exertion (p = 0.027). When analyzing the different post-exertion times (post hoc analysis), RPE and HR showed significant differences between the 6-MRT term and min 1, min 3, min 5, min 7, and min 9 (p < 0.01). The BL only presented significant differences between term and min 5 at high doses (p < 0.05). The kinetics of RPE, HR, and BL post-stress are reported in figure 3.
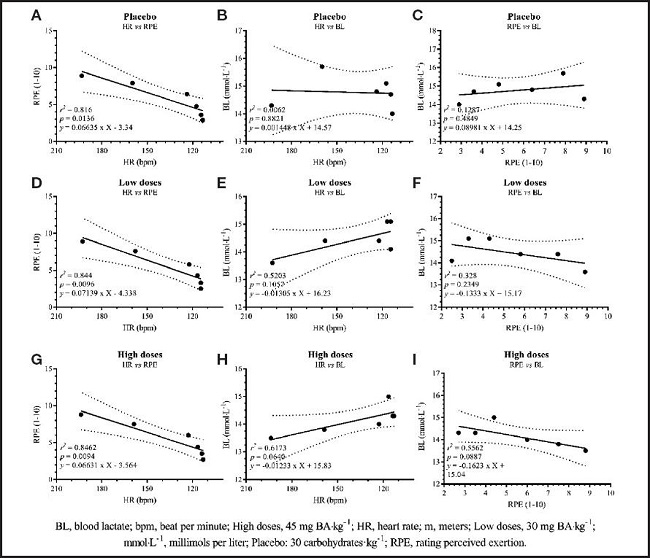
When analyzing the relationship between RPE and HR between the end of 6-MRT and min 9 post-exertion, a practically perfect correlation (r > 0.9, p < 0.05) was observed for the two treatments and PL. However, when correlating HR with BL from the end of 6-MRT to min 9 post-exertion, a trivial correlation (r < 0.1, p > 0.05) was evident for PL. At the same time, a very high correlation (r 0.7-0.9, p > 0.05) was observed for low and high-dose BA. On the other hand, when correlating RPE with BL from the end of 6-MRT to min 9 post-stress, PL obtained a moderate correlation (r 0.3-0.5), while low dose BA evidenced a high correlation (r 0.5-0.7), and high dose BA a very high correlation (r 0.7-0.9). The correlation data, lines, and linear regression equation for each treatment are reported in figure 4.
DISCUSSION
RATING OF PERCEIVED EXERTION
Concerning the main objective of this study, the results indicate that the term RPE and post-exertion recovery RPE do not present significant differences between the two treatments and the PL (p > 0.05). As a first analysis, it can be mentioned that, after maximum efforts, such as 6-MRT, it is expected to observe maximum values in the RPE (15,19,34). These peak perceptions at maximum effort are independent of gender, age, exercise modality, or physical activity level (19). Likewise, maximum values have been observed in the RPE at maximum effort, including cognitive loads in addition to physical effort (15). Also, maximum values in RPE have been observed when comparing groups with and without the intake of ergogenic aids (34). Therefore, the RPE values observed in the present investigation show that the participants exerted their maximum effort in each of the 6-MRT runs, independent of the treatment used.
In a second analysis, it can be mentioned that both ingestion of 30 mg BA·kg-1 and 45 mg BA·kg-1 generate a decrease in RPE from min 1 to min 9 post-exertion when compared to PL after the 6-MRT. In this context, our results allow us to infer that a lower RPE post maximal effort, with both acute doses, could be associated with a positive metabolic response to exercise in HIDZ (35). In this sense, Conde (15) describes that the perception of effort comprises two-thirds of physiological responses and one-third of psychological factors. In turn, this same author explains that fatigue perceived during exercise, from a complex systems model, is a consequence of the complex interaction of multiple peripheral systems that act as afferent signals to the brain, with the higher centers of this organ processing the information and generating a sensation of fatigue (15). Likewise, evidence shows that the ingestion of BA stabilizes pH during exercise and exertion (36). This pH stabilization could generate less noxious afferents to the brain, with a consequent decrease in post-peak recovery RPE. However, the physiological pathway that explains this decrease in post-peak recovery RPE following acute BA intake needs further exploration.
HEART RATE
Our results showed non-significant differences between the two treatments and the PL (p > 0.05) concerning term HR and post-maximal effort recovery. In this sense, Huerta Ojeda et al. (2) found higher term HR in subjects supplemented with 30 mg BA·kg-1 compared to the PL group (p < 0.05). This increase in term HR observed by Huerta Ojeda et al. (2) may be conditioned to an increase in intramyocardial CA after BA intake. Indeed, the cardiac influx during the action potential after increased CA levels has been demonstrated, thus facilitating cardiac contraction and HR (37). However, the term HR depends on the intensity of the exercise (38). Therefore, in this study, it was expected that the term HR for both treatments and PL would not present significant differences. Despite this, at the end of 6-MRT, high-dose BA generated a slightly higher HR than low-dose and PL (p > 0.05).
BLOOD LACTATE
On the other hand, our results show no significant differences between the BL of term and post-exertion recovery between the two treatments and the PL (p > 0.05). However, when analyzing the BL of each treatment separately, it is observed that the group supplemented with 45 mg BA·kg-1 shows significant increases between the 6-MRT term and post-exertion recovery (p = 0.027). This increase in post-exertion BL may be related to the increase in intramyocellular CA (due to BA supplementation) (39). In this sense, it has been observed that a high concentration of intramyocellular CA could buffer H+, increasing the possibility of a more prolonged and intense physical effort (36). Consequently, it is a physical effort at a higher intensity, associated with pH stabilization, responsible for increased BL at the end of 6-MRT and post-exertion recovery. Therefore, in light of the results, it is possible to infer that supplementation with 45 mg BA·kg-1 increases physical performance in middle-distance athletes, allowing better performance in HIDZ.
BA USAGE AND PERFORMANCE IN HIDZ
Concerning the distance obtained in the 6-MRT by the three intervention groups, “excellent” performance was observed in physically active males between 18-25 years of age (32). From these results, the high dose of BA (45 mg BA·kg-1) stands out, evidencing the highest performance in the 6-MRT (1,861.8 ± 65.9 m), with no significant differences between treatments (p > 0.05). Despite the slight differences found between treatments, we suggest the dose of 45 mg BA·kg-1 since a coefficient of variation of 0.1 % can generate a significant difference in sports performance in middle-distance athletes (e.g., a performance of 2 min 10 s in 800 m flat, could improve 0.13 s with the intake of 45 mg BA·kg-1 60 min before the race). However, individual analysis is needed to determine whether BA supplementation can improve training and competition performance in HIDZ (40).
RELATION BETWEEN RPE AND HR
When analyzing the relationship between RPE and HR from the end of the 6-MRT until min 9 post-exertion, our results show an almost perfect correlation for all treatments (r > 0.9, p < 0.05). Several studies report a strong relationship between RPE and HR during exercise (19) and post-exertion (2). Consequently, these antecedents show that RPE is a reliable and low-cost method for establishing physiological stress (41) and workload during and after exercise (42).
RELATION BETWEEN RPE AND BL
In parallel, when analyzing the relationship between RPE and BL from the end of 6-MRT to min 9 post-exercise, our results indicate that low dose and high dose BA present a high and very high correlation between RPE and BL, respectively. In this context, in an investigation by Scherr et al. (19), a very high correlation between RPE and BL during exercise is observed (r = 0.83, p < 0.001). Unfortunately, the researchers do not report the relationship between both variables during post-exertional recovery. This scarce information makes this analysis and discussion difficult. However, thanks to the data collected in our study, it can be inferred that the group supplemented with 45 mg BA·kg-1 presents kinetics in the BL of post-exertion recovery inverse to the RPE (r = -0.745, p > 0.05). Likewise, with this treatment (45 mg BA·kg-1), a peak in BL was observed at min 5 post-exertion, differing significantly from term BL (13.47 ± 2.31 vs. 14.99 ± 2.20 mmol·L-1, p < 0.05). In this sense, in an investigation developed by Huerta Ojeda et al. (2), which aimed to determine the acute effect of supplementation with 30 mg BA·kg-1, a significant increase in the BL at min 3 post-exertion was observed, differing significantly from the BL of the PL group (13.60 ± 3.67 vs. 16.80 ± 3.35 mmol·L-1, p < 0.05). The increase in post-exertion BL observed in the present study (min 5), as in other investigations (min 3) (2), may be associated with increased bioavailability of intramyocellular CA (product of BA supplementation) (43). Likewise, in several studies that included maximum-intensity exercise, it is evident that BL increases progressively after the end of exercise (44). Indeed, lactate values close to 15-25 mmol·L-1 at 3-8 minutes post-exertion have been observed (45). Based on these results, both the use of a low dose of BA (30 mg BA·kg-1) and a high dose of BA (45 mg BA·kg-1) may generate a peak in BL between 3-5 min post-exertion; this post-exertion BL kinetics could be evidence of a greater H+ buffering capacity within skeletal muscle (buffer effect) (8), delaying the onset of fatigue during high-intensity exercise (9) and allowing better performance in HIDZ.
In summary, a lower post-maximal effort RPE generated by the acute intake of BA or another ergogenic aid would allow better manipulation of training loads and, eventually, enable better results in HIDZ (4). For example, a faster post-exertion recovery could reduce the rest time between repetitions, optimizing training sessions. Consequently, it has been shown that RPE can be a helpful tool to prescribe and control training intensity practically and economically since it reliably represents physiological parameters involved in exercise (16,46). Furthermore, RPE allows the quantification of exercise load (19,20), becoming an alternative to measure fatigue levels (21) and the state of post-exertion recovery (22).
CONCLUSIONS
Our findings show that acute supplementation with BA, with low and high doses, generates a lower post-maximal effort RPE in middle-distance athletes. This decrease in post-peak RPE and the increase in post-exertion BL, mainly with the high dose of BA, could be related to an increase in physical performance in HIDZ.
PRACTICAL APPLICATIONS
Coaches and middle-distance athletes seeking an ergogenic aid to enhance physical performance in HIDZ should consider BA supplementation. Based on our findings, we suggest a 30- 45 mg BA·kg-1 60 min before training or competition. However, the first step is to consult qualified professionals about each reality's most appropriate dosing formats. Also, athletes should be educated about RPE. Finally, it is advisable to observe the individual responses of each athlete to determine the actual effect of BA supplementation (40).

