










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
There is evidence suggesting that physical inactivity and sedentary behavior increase the risk of adverse health outcomes (1). In particular, a sedentary lifestyle and/or low physical activity increases the risk of pathologies in the lower extremities (LE) (2) and, from a musculoskeletal point of view, it has been associated with a decrease in muscle mass (3), generating a reduction in the physiological cross-sectional area, altering the ability to develop higher levels of muscle strength and power. Strengthening protocols are largely used to improve muscle performance outcomes such as maximum strength and power. A variety of strength training modalities have been shown to be effective in improving these variables in both trained and untrained populations (4). However, in an untrained population, the effects have been described with little verification of their level of physical activity (i.e., sedentary, physically inactive or physically active-sedentary), even though it has already been established that training status influences the capacity of a muscle to gain strength (5), and sedentary lifestyle is considered as an additional risk factor to physical inactivity (6,7). In brief, how different types of strength training affect lower limb muscle activity, strength, and power of sedentary and/or physically inactive subjects remains unclear.
It has been stated that gender (8) and age (9) modulate the effects of strength training on physical and muscle performance. Additionally, there are differences in the effects of strength training between the upper and lower limbs due to morphological and functional differences (10). From a functional perspective, it is thought that the upper limbs have adequate levels of strength and mobility to allow their use in daily life activities and that the lower limbs have adequate levels of strength and balance to safely allow mass displacement. In the upper limb, strength training has been shown to improve other performance and functional variables (11-14). In the lower limb, there is evidence suggesting that strength protocols can reduce pain and improve physical function in knee osteoarthritis (15), and can reduce the risk of an anterior cruciate ligament tear in athletes (16). However, the effects of strength protocols on muscle power and electrical activity in sedentary or physically inactive subjects is lacking, despite the relevance of these variables for the function attributed to the lower limbs (i.e., walking, sit to stand).
Regarding the benefits of strength exercise in an untrained population, it has been suggested that some training methods (i.e., plyometric) might be more suitable for this population as they require almost no equipment, very little space, and relatively little time to be completed, as a lack of these things can be a major determinant of sustained engagement in a physically active lifestyle (17). Also, plyometric training improves jumping performance and skeletal muscle contractile properties in seniors (18), as well as muscle activation during the performance of strength and jumping tasks (4). Similarly, traditional resistance training leads to positive effects on strength and body composition in overweight sedentary populations (19). However, due to the scarce verification of the level of physical activity of the subjects included in those studies, the effects of these two modalities (and other types of strength training) on lower limb power and muscle activity of sedentary and/or physically inactive subjects remain unclear.
Considering the above, it is necessary to substantiate the effects that strength protocols have on the levels of strength, power, and muscular activity of the lower extremities to establish interventions that improve these muscle outcomes, considering their impact on preventing the risk of injuries and/or comorbidities in sedentary and/or physically inactive subjects. Despite a review conducted on untrained individuals (without a specific analysis based on the level of physical activity of the untrained) (4), no systematic review has been conducted to establish the effects of lower extremity strength protocols on muscle activation, strength, and power outcomes in sedentary or physically inactive subjects. Thus, the objective of this systematic review was: a) to determine the quality of evidence from studies assessing the effects of different lower limb strengthening protocols on muscle activity, strength, and power in sedentary and/or physically inactive subjects; and b) to determine the effectiveness of lower extremity strengthening protocols on muscle activity, strength, and power in sedentary and/or physically inactive subjects.
MATERIALS AND METHODS
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines were used (20). The protocol of this review was registered in PROSPERO (CRD42021267316).
STUDY SEARCH
The search was performed by two authors. The databases used were Medline, Scopus, SPORTDiscus and Web of Science. The search was performed from inception until July 2021. The following keywords were included: “Resistance Training”, “Resistance exercise”, “Strength training”, “Lower Limb”, “Lower Extremities”, “Sedentary Behavior”, “Physical Inactivity”, “Sedentary Lifestyle”, “Sedentary”.
ELIGIBILITY CRITERIA
To ensure a comprehensive review, articles were selected without time limits and based on the following criteria: a) subjects > 18 years old who were sedentary or physically inactive, both determined according to previous criteria (1); b) participation in lower extremity strength training program over four weeks; c) randomized clinical trial design; d) studies reporting measures of power, strength and/or muscle activity (i.e., electrical activity); e) full text available; and f) articles in English. In addition, exclusion criteria were: a) articles which included trained and/or physically active subjects; b) conference presentations, theses, books, editorials, review articles and expert opinions; c) duplicate articles; and d) those in which the principal or secondary authors did not respond to e-mail requests.
STUDY SELECTION
The articles retrieved from the search were entered into the Rayyan QCRI application (21), an app that assists the article selection process, optimizing review time and allowing collaborative work among researchers (available for free from: http://rayyan.qcri.org [accessed on July 17th, 2021]). Duplicate articles were eliminated, and two investigators independently reviewed titles and abstracts to identify articles that met the eligibility criteria. In case of discrepancies, a third investigator was consulted and the dispute was resolved by consensus. Finally, the selected articles were thoroughly read, and the reference list was reviewed for relevant articles that could be included.
ASSESSMENT OF THE RISK OF BIAS AND QUALITY OF EVIDENCE
Each article included in this systematic review was independently assessed for methodological quality by two researchers using the PEDro scale (22). This scale consists of eleven items encompassing external validity (item 1) and considers two aspects of trial quality, namely the “credibility” or internal validity of the trial (criteria 2 to 9), and whether the trial contains enough statistical information to make it interpretable (criteria 10 and 11). Items were rated yes or no (1 or 0) according to whether the criterion was clearly satisfied in the study. A total PEDro score was achieved by adding the ratings of items 2 to 11 for a combined total score between 0 to 10. It has been suggested that scores < 4 are considered “poor”, 4 to 5 are considered “fair”, 6 to 8 are considered “good” and 9 to 10 are considered “excellent” (23). In case of disagreement among researchers, the consensus approach was used; for cases in which consensus could not be reached, a third researcher was consulted.
DATA EXTRACTION AND ANALYSIS
An Excel template was used for data extraction for each manuscript selected for review and the following information was considered: sample size, gender, age, body mass, height, type of training, resistance training protocols (frequency, weeks, volume, rest), outcomes (muscle activity, power, strength), conclusions or practical applications. No method was used to prepare the data for presentation or synthesis, only original information from the included manuscripts was presented. Meta-analyses could not be undertaken due to the heterogeneity of the methods used to quantify force (i.e., isokinetic, isometric, RM) or power (i.e., kinematics, kinetics) and, because of the lack of studies comparing changes in muscle activity, in this sense a narrative synthesis was made.
RESULTS
STUDY SELECTION
No systematic reviews with objectives similar to those of the present study were found. From the initial search, 164 articles were retrieved (Fig. 1), 114 of which were eliminated because they were duplicates. Six additional articles were identified from other sources. All the articles that assessed strength, power, and/or muscle activity presented a control group. After evaluating titles and abstracts, 44 articles were excluded because they did not meet the inclusion criteria, leaving 12 articles for full-text analysis.
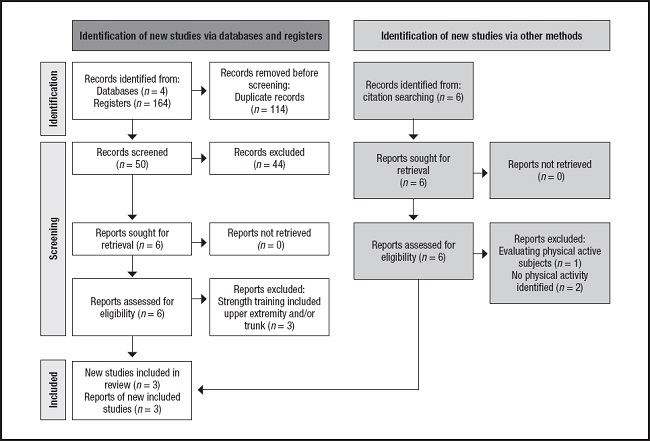
Of the 12 articles, four did not clearly establish the level of physical activity of the subjects; upon contacting the authors, one study continued to be included, one was eliminated for having evaluated physically active subjects, and another two were eliminated for not responding to the query. Of the remaining nine, after reading the full text, three articles were eliminated because their strength protocols were not related only to lower limbs. Thus, six articles were selected (24-29), their reference lists were checked, and no new articles were found.
STUDY CHARACTERISTICS
Table I shows the characteristics of the subjects included in the studies, table II shows the characteristics of the protocols applied, and table III shows the main findings per study.
Table I. Characteristics of participants per study.
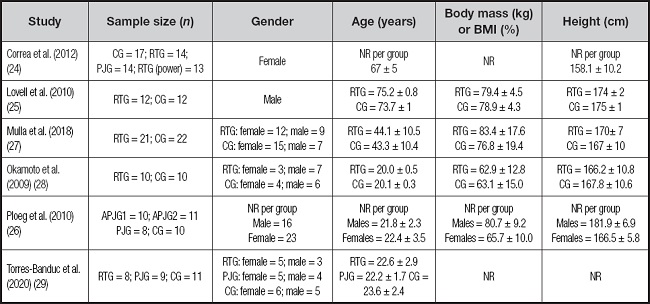
Age, mass and height data are reported as mean ± standard deviation.
BMI: body mass index; CG: control group; RTG: resistance training group; PJG: plyometric jump group; NR: non-reported; APJG: aquatic plyometric jump group.
Table II. Summary characteristics of the protocols per study.
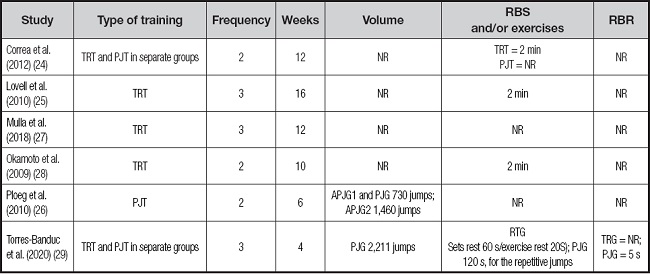
TRT: traditional resistance training; PJT: plyometric jump training; APJG: aquatic plyometric jump group; RBS: rest between sets; RBR: rest between repetitions; RTG: resistance training group; PJG: plyometric jump group; NR: non-reported.
MUSCLE STRENGTH OUTCOMES
In the six studies that explored muscle strength outcomes (24-29), the pooled number of participants was 212 (67.5 % females) (Table I), with an age range varied from young to older adults. The median sample size per study was 29 (range 20-55 participants) (Table I). The interventions lasted from four to 16 weeks. Training frequency was from two to three days per week. Traditional strength training was performed in five studies (24,25,27-29) (two of them included plyometric training in separate groups), and one (26) performed plyometric training exclusively (Table II). In order to evaluate muscle strength, three studies used isometric strength tests (25,27,29), two used isotonic strength tests (24,28), and one used isokinetic test (26).
MUSCLE POWER OUTCOMES
In the two studies that explored muscle power outcomes (26,29), the pooled number of participants was 67 (58 % females) (Table I). The mean sample size per study was 34 (range 28-39 participants). The interventions lasted from four to six weeks. Training frequency was from two to three days per week. Plyometric training was performed in two studies (26,29) (one of them included traditional strength training in separate groups) (Table II). In order to evaluate muscle power, one study used an isokinetic test (26), and one used cinematic analysis with a mobile app to obtain it (29). Of note, this variable was only studied in young subjects (i.e., between 18 to 25 years).
MUSCLE ACTIVITY OUTCOMES
One study explored muscle activity outcomes (24), the number of participants was 58 (100 % females), with an age of ≥ 65 years (Table I). The intervention lasted 12 weeks. Training frequency was two days per week. Plyometric training and traditional strength training were done in separate groups (Table II). In order to evaluate muscle activity (e.g., maximum activity and latency), the study used surface electromyography.
EFFECTS OF STRENGTH INTERVENTIONS ON MUSCLE OUTCOMES
Regarding muscle power, one of the studies that contrasted TRT and PJT of the same duration and frequency (29) found significant improvements (i.e., p < 0.05) in vertical jump and countermovement jump power after four weeks of PJT with a frequency of three times per week, and a total volume of 2.211 jumps, the same significant effect found in the group to which TRT was applied (Table III). However, between both groups the improvement was similar, so there would be no differences between the benefits of applying one or another type of training in sedentary and/or physically inactive subjects. In contrast, the second study that investigated muscle power (26) did not find significant differences in the isokinetic power of knee flexors and extensors in any of the PJT modalities (i.e., aquatic and firm surface) carried out for six weeks, twice a week, with a total volume between 730 to 1.460 jumps.
Table III. Main findings of the included studies.

RTG: resistance training group; NR: non-reported; TRT: traditional resistance training; PJT: plyometric jump training; CMJ: countermovement jump; SJ: squat jump; ↑: significant improvement; ↓: significant detriment.
In the case of muscular activity, the study that investigated it (24) found significant improvements (p < 0.05) in maximal muscle activation (+44 % average) and onset latency (-31 % average) for vastus lateralis, vastus medialis, and rectus femoris (Table III), after six weeks of TRT with a frequency of two times per week. The same study, following six more weeks of different types of strength training protocols (i.e., TRT and PJT), found a significant (p < 0.05) increase in the onset latency, and reaction time only for the rectus femoris muscle, being these neuromuscular improvements in greater magnitude for the PJT than 12 weeks of TRT alone.
Finally, with regard to muscle strength, all the studies that implement TRT (24,25,27-29) with program duration varying from four to 16 weeks and a frequency of two to three times per week, found significant (p < 0.05) improvement in this outcome (Table III), the same result found for a PJT of four to six weeks, with a weekly frequency of two to three days (24,29). However, one study that implemented PJT (26), after six weeks with a frequency of two times per week, did not find significant improvement in training. Improvement generated by both training modalities (i.e., PJT and TRT) has only been investigated in thigh mus- cles (i.e., flexors and extensors). Of note, only in PJT programs, the training volume was reported.
METHODOLOGICAL QUALITY
The average score on the PEDro scale was as follows: four studies were classified as being of fair methodological quality (24-26,29) and two were considered of good methodological quality (27,28). Scores on all items of the checklist are reported in table IV. In general, enough statistical information to make results interpretable was the aspect most achieved (two of a maximum of two points). Regarding external validity (i.e., generalizability or applicability of the study) five studies obtained the point associated with this item except one (28). Internal validity was the least achieved aspect in all studies (i.e., four of a maximum of eight points), indicating a poor validity of the results since it is not possible to ensure that the studies are free of biases or systematic errors. Consequently, the results of the studies included in this review should be taken with caution.
Table IV. Results of the methodological quality assessment using PEDro score.
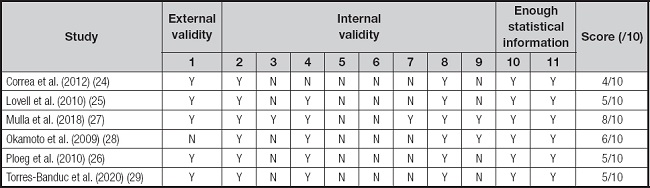
Y: yes; N: no.
Items considered for rating: 1) eligibility criteria were specified (this item is not used to calculate the PEDro score); 2) subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received); 3) allocation was concealed; 4) the groups were similar at baseline regarding the most important prognostic indicators; 5) there was blinding of all subjects; 6) there was blinding of all therapists who administered the therapy; 7) there was blinding of all assessors who measured at least one key outcome; 8) measures of at least one key outcome were obtained from more than 85 % of the subjects initially allocated to groups; 9) all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat”; 10) the results of between-group statistical comparisons are reported for at least one key outcome; and 11) the study provides both point measures and measures of variability for at least one key outcome.
DISCUSSION
The aim of this review was: a) to establish the level of evidence from studies assessing the effects of different lower limb strengthening protocols on muscle activity, strength, and power in sedentary and physically inactive subjects; and b) to determine the effectiveness of lower extremity strengthening protocols on muscle activity, strength, and power in sedentary and/or physically inactive subjects. The main findings of this review were: a) the articles included in this review have a “fair” or “good” methodological quality, mainly due to their low scores associated with the internal validity criteria, indicating poor validity of their results, since it is not possible to ensure that the studies are free of biases or systematic errors; and b) the protocols used to improve lower limb strength in sedentary and/or physically inactive subjects are effective in improving the strength, power and muscular activity of some lower limb muscle groups. However, it was not possible to establish a measure of effectiveness due to the heterogeneity in the methods used to quantify force (i.e., isokinetic, isometric, RM) or power (i.e., kinematics, kinetics), and because of the lack of studies comparing changes in muscle activity. Considering the above, strength training in the lower limb seems to improve the levels of strength, power, and muscular activity in sedentary subjects, though due to the limited number of articles, methodological variability, and training methods used, it is necessary to develop new studies that control these variables.
MUSCLE ACTIVITY
We found that PJT and TRT produced improvements in neuromuscular variables of thigh muscles (i.e., increased amplitude and reduced onset latency), and that these changes were more pronounced in subjects under PJT. Of note, only one study included in this review explored this variable, in women over 65 years of age who performed TRT prior to PJT.
Similar to our findings, a recent review establishes that PJT may improve muscle activation in a healthy trained and untrained population (4), but offers conflicting results for methodological and inadequate PJT prescription. PJT may improve muscle activity due to an increased neural drive to the agonist muscles (i.e., onset latency and amplitude) (30), which can explain why in the study by Correa et al. (24) the improvements were found in the onset and amplitude of the thigh extensor muscle (i.e., Knee agonist of the PJT implemented). It has been stablished that muscle activity (i.e., amplitude and timing) of leg muscles during gait commenced declining at age 60 (31). Therefore, the application of strength training protocols in lower limbs could help this population maintain functional independency (i.e., sit to stand and gait). However, considering the lack of studies and the limited external validity of the results, it is important to continue investigating the effects of PJT and other resistance training on muscle activity in sedentary and/or physically inactive subjects.
MUSCLE STRENGTH
We found that TRT and PJT can induce significant improvements in muscle strength, however, the volume (i.e., total jumps) seems to be important for the PJT since a total volume of 1,460 jumps was not capable of inducing strength improvement on lower limb muscle as was established in the results of Ploeg et al. (26). Similar to our findings, contradictory information regarding the effects of PJT on lower limb strength in athletic and non-athletic population has been found (30). This contradictory information may be attributed to non-adherence to guidelines about the intensity and volume recommended when PJT is applied, an issue also established in other reviews investigating the effects of PJT programs (4,32).
Regarding TRT, findings similar to ours described that it is capable of improving lower limb strength (33) in a non-athletic population. The strength of a muscle depends on neural, architectonics, and mechanical factors. These, in turn, depend on training frequency and duration, and it has been established that TRT and PJT may improve muscle architecture (i.e., increase in cross-sectional area, and change stiffness in components of the muscle-tendon complex) and neural factors like rate coding and/or motor unit synchronization (5,30,34). Accordingly, in the studies included on this review the duration and frequency of training (i.e., four to 16 weeks, two to three days per week) has already been shown to generate the aforementioned adaptations (5,32). Of note, the total volume was not reported in the studies conducting TRT, though this issue must be taken into account considering that overweight sedentary subjects improved strength and body composition only in programmed resistance training (19).
MUSCLE POWER
Despite the lack of data (i.e., only two studies examined this variable), we found evidence that TRT induces significant improvements on muscle power, and that evidence for PJT is contradictory. The contradiction in the muscle power results during the PJT may be due to the difference in the weekly frequency and/or the 44 % of difference in the total volume between the two studies that examined the effect of PJT on muscle power (26,29). Indeed, recent reviews establish the relevance of training volume control in resistance programs (5,35) and specifically in PJT programs (32), because this may provoke distinct results in expected muscle outcomes. In fact, if the goal is to augment the muscle strength (basis of muscle power), augmentation of training volume is recommended (35). The total volume in bodyweight resistance exercise (i.e., PJT) is likely related to enhanced neural drive, improvements in the stretch reflex, increased reutilization of stored elastic energy, improved muscle activation strategies with greater motor-unit recruitment, and better inter and intra-muscular coordination (36,37), all of them factors that can explain the augmented lower limb muscle power.
Of note in the studies that included both genders, male versus female analyses were not performed. This is relevant since it has been established that women are less active (38) and fall more often than men, and that there is a relationship between sedentary habits and decreased strength levels in the lower limb; consequently, it is relevant to compare the effects of strength training between sexes in a sedentary population. Another aspect not addressed in the studies included in this review is the effect of resistance programs in the intersegmental dominance or the preferential use of one limb, since differences in neuromuscular control and levels of muscle mass in the dominant limb have already been found in sedentary subjects (39). Moreover, high levels of asymmetry have been associated with a greater risk of injury (40) and alterations of functional patterns (41,42), therefore, it is relevant to investigate this aspect in sedentary subjects. Future research of high methodological quality is needed to determine the effectiveness of lower extremity strengthening protocols, especially on muscle activity, and power in the aforementioned population, distinguishing between gender, intersegmental dominance and age.
LIMITATIONS AND STRENGTHS
The strength of this review lies in the comprehensive search for studies conducted across the primary four databases associated with training research, without imposing any date restrictions until 2021. This approach provided a broad perspective of the current information available. Nonetheless, a significant limitation of our analysis of the effects of lower limb strengthening protocols on muscle activity was that it was based solely on one study involving a sample of 58 females. Furthermore, there was substantial heterogeneity in the analysis of muscle strength. Nevertheless, it is noteworthy that all studies included in this review demonstrated a preference for traditional resistance training. The variation in the effects of plyometric jump training may be attributed to the differences in training volumes applied. Given the scarcity of research and the limited external validity of the results, some findings of this review should be interpreted with caution.
CONCLUSION
The findings of this systematic review indicate that the quality of studies assessing the effects of different lower limb strengthening protocols on muscle activity, strength, and power in sedentary and physically inactive subjects was fair to good. Moreover, the available information did not allow a measure of effectiveness and was of low internal validity.

