










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Anxiety and depression are the most prevalent mental disorders and the main causes of disability (1). The World Health Organization (WHO) estimates that 970 million people worldwide had a mental disorder in 2019 (1,2), constituting data that had significant growth during the COVID-19 pandemic (3-8). This mainly occurred in the first year (2020) (3), highlighting an increase of 27.6 % in depression cases and 25.6 % in anxiety cases (9).
The COVID-19 pandemic changed the physical activity (PA) level and diet of the population. As a result, changes in body mass index (BMI) were noticed, and anxiety and depression were intensified (10-14), which led to a strong call for interventions aimed at promoting mental health. New scenarios such as the COVID-19 pandemic can show unexpected patterns in people’s behavior (15). While some people may have sufficient autonomous regulation of PA to pursue alternative activities (i.e., on-line fitness classes, other physical activities at home), others may reduce their PA due to lack of available social support or concerns about contracting the virus in an outdoor environment (10-14). In addition to regular PA, this condition can compromise the maintenance of a healthy and varied diet and strongly interfere with the body composition and health of the population (16-20).
Practicing PA can play an important role in maintaining body composition, can contribute to controlled food intake and can reduce anxiety and depression symptoms (21-28); in addition, it can act as a protective factor for the onset of these mental disorders in all age groups and in all geographic regions (22,25).
The human body was born to be active and quickly and negatively adapts to a sedentary lifestyle and poor diet, resulting in negative changes in body composition and health problems (21,23,24,27). There is conclusive evidence that physical inactivity plays a role in most chronic diseases, and if a bad sedentary habit persists, it will result in substantial reductions in longevity and quality of life (21-25,27). Studies that have investigated the role of PA in mental health have shown that even light PA, such as walking, can contribute to reducing anxiety/depression symptoms, and that moderate and vigorous PA can maximize the reduction in symptoms (26,28,29). Practicing PA can also reduce anxiety and depression symptoms related to body weight (16-20). However, the mediating role of PA in the relationship between body composition and anxiety/depression symptoms needs to be better investigated (16-20). Therefore, this investigation aims to contribute to developing strategies to promote mental health in adults.
Thus, the objective of the study was to verify the mediation of the PA level in the relationship between BMI and anxiety/depression symptoms in Brazilian adults.
METHODS
The present study was conducted in accordance with the Declaration of Helsinki, complied with the research rules involving human beings of the Brazilian National Health Council, and was approved by a local university research ethics committee (CAAE: 30750220.1.0000.0102, date: June 9th, 2020).
This is a descriptive correlational study of an epidemiological nature carried out with Brazilian adult men and women, ≥ 18 years of age. The sample was selected for nonprobabilistic convenience. The recruitment process took place through dissemination in digital communication media/media (such as WhatsApp®, Telegram®, Facebook®, Twitter®, e-mails), where interested parties had access to the questionnaire “Questionnaire on the habits of PA practice: dietary and psychological aspects due to social distance derived from the new Coronavirus (COVID-19)”, through the Google Drive form. Participants only accessed the questionnaire to check the informed consent form authorizing the use of data collected in scientific works resulting from the results of this study proposal, which was on the initial page.
To verify or determine the sample’s aesthetic power in verifying a study hypothesis, an a posteriori calculation was performed, considering a 95 % confidence level (α = 0.05) and a power of 80 % (β = 20), a prevalence of PA three times a week during isolation of 21.1 % (own sample), observed in 2000, during which it is possible to identify causes of prevalence above 1.28 as risk and below 0.75 as protection. The calculations were performed using the G*Power version 3.1.9.4 calculator.
First, 2145 adults completed the questionnaire of this research, but only those who were under 18 were excluded. Participants who did not present their positive informed consent form, as well as those who answered the questionnaires incorrectly, were considered as missing data (n = 145). Thus, the final sample of this study included 2000 Brazilian adults.
SOCIODEMOGRAPHIC AND HEALTH FACTORS
Sex (male or female), age (years), body weight (kg) and height (m) were self-reported by participants. BMI was calculated from the ratio between body weight (kg) and the height squared of the participants (m2). Nutritional status was determined following the WHO criteria (30): < 25 kg/m2 (“not excess weight”) or ≥ 25 kg/m2 (“excess weight”). Participants were asked about their health status with the questions: “Do you have cardiovascular disease/diabetes/hypertension/respiratory disease?”, “Do you smoke tobacco or consume alcohol?”. These questions offered dichotomous options for answering (yes or no).
DAILY PHYSICAL ACTIVITY (PA)
The practice of daily PA was assessed during social isolation caused by COVID-19 through the question: “What is your average daily exercise during social isolation?”. Participants were asked to answer this question in minutes per day.
PSYCHOLOGICAL ASPECTS
Psychological aspects were assessed using the K10 instrument (31). The instrument consists of ten questions, assessing anxiety (first four questions) and depression (last six questions) in the last 30 days. The questions are as follows: “During the past 30 days, how often did you feel… exhausted for no good reason?”, “… nervous?”, “… so nervous that nothing could calm you down?”; “…hopeless?”, “… restless or agitated?”, “… so restless that you could not stand still?”; “… depressed?”, “… so depressed that nothing could cheer you up?”; “…worthless?”. Finally, the last question was “During the past 30 days, how often did you feel that everything was an effort?”
The different answers consist of a Likert scale (never, a little, part of the time, most of the time and all the time). From the ten questions, the answers were added, establishing a final score, which could vary from 10 to 50. For the purposes of analysis, the variables were used continuously (32).
DATA ANALYSIS
Descriptive statistics were expressed as the mean and standard deviation for continuous variables and numbers and percentages for categorical variables. Statistical normality of the variables was verified using the Shapiro-Wilk test. Student’s t test was used to verify mean differences in continuous data between sexes. BMI, daily PA and K10 test score had skewed distributions and were transformed prior to analyses. To aid interpretation, a two-step approach was used to transform non-normally distributed continuous variables into normally distributed variables. Additionally, we created four different categories related to BMI and PA to show the differences across them: a) active/decreased BMI; b) active/increased BMI; c) insufficiently active/decreased BMI; and d) insufficiently active/increased BMI. Bivariate and partial correlation coefficients (r), adjusted by potential confounders, were calculated to verify the relationships between changes in BMI, daily PA and anxiety/depression. Analyses of covariance (ANCOVA) were used to assess the differences between means of K10 test score across groups of changes in BMI (increased BMI and decreased BMI) and daily PA (active and insufficiently active). Pairwise post hoc comparisons were examined using the Bonferroni test. Initial analyses revealed no significant interactions between sex and mean differences in changes in BMI and PA (changes in BMI p = 0.173; and PA p = 0.606); hence, all analyses were carried out with both women and men together to increase statistical power. To verify whether the association between BMI and anxiety/depression was mediated by daily PA, linear regression models were performed using bootstrapped mediation procedures included in the PROCESS SPSS macro (version 3.5). The first equation regressed the mediator (daily PA) on the independent variable (changes in BMI). The second equation regressed the independent variable (changes in BMI) on the dependent variable (anxiety/depression). The third equation regressed the anxiety/depression dependent variable on both the independent (changes in BMI) and the mediator variable (daily PA).
The following criteria were considered to establish mediation: a) the independent variable is significantly associated with the mediator; b) the independent variable is significantly associated with the dependent variable; c) the mediator is significantly associated with the dependent variable; and d) the relationship between the independent and dependent variables is diminished when the mediator is introduced in the regression model.
The data collected from the Google Drive form were moved to Microsoft Excel 2016 (Microsoft Corp, Redmond, WA, USA) and, after that, to the software SPSS (IBM Corp, Armonk, NY, USA) for Windows (version 24.0). All the analyses performed were adjusted by age, sex, chronic diseases (cardiovascular disease, diabetes, hypertension, and respiratory disease), smoking and alcohol consumption. Finally, a value of 5 % was considered to establish statistical significance.
RESULTS
Table I shows the descriptive characteristics of the participants. Men reported a higher K10 test score (p < 0.001) in all aspects: global, anxiety and depression scores. Conversely, women showed greater age, body composition and daily PA (p < 0.001 for all variables).
Table I. Characteristics of the analyzed sample according to sex (N = 2000).

BMI: body mass index; PA: physical activity.
Table II reports the bivariate and partial correlations among daily PA, changes in body composition and anxiety/depression. Daily PA was inversely related to both changes in body composition and anxiety/depression. In contrast, changes in body composition showed a positive association with anxiety/depression. Notwithstanding, all these correlations were low.
Table II. Bivariate and partial correlations among body composition, anxiety/depression and daily physical activity (N = 2000).
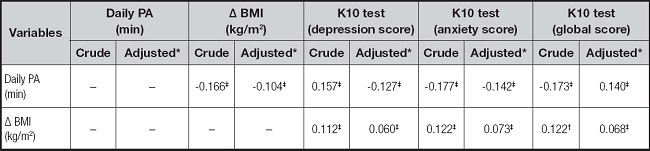
PA: physical activity; BMI: body mass index.
*Adjusted by sex, age, chronic diseases, alcohol consumption and smoking. Delta (Δ) indicates the change in BMI.
†p < 0.050;
‡p < 0.001.
ANCOVA showed the lowest score in anxiety/depression in the insufficiently active/increased BMI group. Likewise, we found significant differences between active/decreased BMI and insufficiently active/increased BMI (p = 0.007) for anxiety/depression after adjusting for age, sex, chronic diseases, alcohol consumption and smoking (Fig. 1).
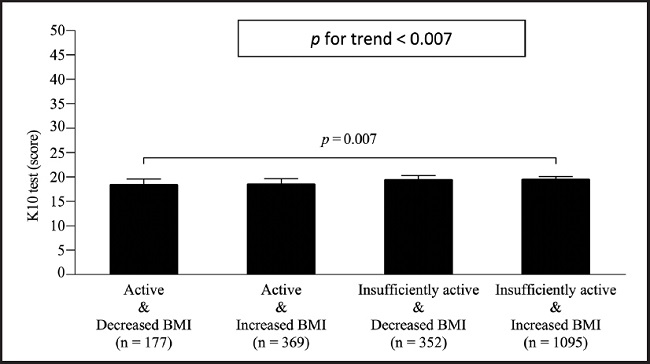
Figure 1. Combined effects of body mass index (BMI) and daily physical activity on anxiety/depression. Estimated mean (bars) and 95 % CI (error bars) represent values after adjustment for age, sex, chronic diseases, alcohol consumption and smoking.
Estimated mean (bars) and 95 % confidence interval (CI) (error bars) represent values after adjustment for age, sex, chronic diseases, alcohol consumption and smoking.
On the other hand, when we tested the mediating role of daily PA in the association between changes in body composition and anxiety/depression, in the first regression equation, changes in body composition were negatively associated with daily PA unstandardized beta coefficient [β] = -3.720; p < 0.001).
In the second equation, changes in body composition were positively related to anxiety/depression (β = 0.541; p < 0.050). Last, in the third equation, when changes in body composition and daily PA were simultaneously included in the model, daily PA showed an inverse relationship with anxiety/depression (β = -0.032; p < 0.001), and although changes in body composition remained positively associated with anxiety/depression, this association was slightly ameliorated (β = 0.117; standard error [SE] = 0.041 [0.050, 0.211]) (Fig. 2).

DISCUSSION
This study presents some important relationships about the role of PA in relation to body composition and mental health (anxiety and depression). The results suggest that the effect of body composition on mental health was partially mediated by daily PA, which reinforces the importance of staying active daily (19,20) and intensifies the attention of researchers, public policy makers and the population to the role of PA in body composition and mental health (2,28,33).
The present study showed that a low daily PA level and having overweight and obesity (through BMI) were related to higher anxiety and depression levels, which agrees with studies in the area (1,2,21,23,24,27,28). The literature has shown that nutritional status and having overweight or obesity can trigger high stress levels when compared to individuals classified as normal weight (16-20,30).
The present study showed that maintaining an average of 30 minutes/day of PA was associated with lower anxiety and depression levels, even for those with overweight or obesity, and suggests that the relationship between BMI and mental health (anxiety and depression) was partially mediated by daily PA (30 minutes/day). Similar effects were observed with PA and anxiety and depression symptoms when evaluating the minimum overall recommendations for PA in a week (34-36). Evidence has shown inverse associations between PA and depressive symptoms even during the COVID-19 pandemic, which demonstrates well-established inverse associations with mental health (22,25,26,28,29,37-39). The present findings support concerted efforts to promote opportunities for daily PA to preserve mental health among previously physically active adults and potentially improve mental health among physically inactive adults (1,2,22,26).
Scientific evidence points to replacing passive sedentary behaviors with mentally active behavior, light PA or moderate to vigorous PA (26). Exercise should be offered as an evidence-based treatment option with a focus on supervised, group exercise with moderate intensity and aerobic exercise to produce moderate to large effects on symptoms (28). The recommendation for PA at different intensities had a significant impact on young adults, highlighting the following: PA at an intensity of 6 < 9 Mets had a greater effect on anxiety than on depression; interventions of eight weeks or less and less than four times a week performed better than longer interventions; and the overall effect of a single 30-minute intervention was more effective than that of 60-minute interventions (29).
Additionally, potential approaches may include telehealth interventions, social media, or public airtime devoted to promoting/implementing home-based PA to facilitate activity among vulnerable and isolated populations (40). In addition to the recurring discourse that people should include PA in their daily context, it is important to remember that initiatives to promote PA require humanized approaches that consider the unequal living conditions of Brazilians (38,39).
Regarding changes in body composition, it is likely that weight loss takes time, as many factors are associated with weight loss (18); however, this does not mean that individuals are not obtaining health benefits from practicing PA, such as anxiety and depression reduction, which may appear before weight reduction and serve as a driver for weight loss (13,14,21,23,24,27,28). Regarding average daily PA, it is important to remember that any PA is better than none (39). Using strategies that facilitate adherence to the practice is fundamental:
Start with ten minutes of daily aerobic PA.
Then, increase to 15 minutes/day.
As you feel more comfortable, increase the volume until you reach 30 minutes/day of aerobic PA.
Performing fractional PA (periods of ten minutes) is an option.
Gradually include other types of PA, such as strength and stretching exercises, which are as important as aerobic PA (40).
The practice of daily PA is associated with resilience, as studies on the subject have shown that it is associated with all resilience factors (31); specifically, light PA predicted control, and vigorous PA predicted self-efficacy and optimism (40). People who regularly engaged in vigorous exercise during the first week of confinement for COVID-19 were more likely to cope better with day-to-day demands (15,16,40) and had greater resilience when compared to those with low resilience scores, and people with high resilience scores tended to have more positive emotions in stressful situations and to have more emotional flexibility in response to a stressful psychological task (40).
Some limitations must be pointed out for a better understanding of the results. Reverse causality, a common feature in studies with a cross-sectional design, does not enable investigating a cause and effect relationship or determining the direction of relationships. However, this study design was carried out in several studies such as this one. The invitation to participate was sent to all regions of the country (through social networks); however, the response was different for each region, which does not allow for a representative sample of each region. The use of self-reported data depends on the veracity and power of the responses in the registered record. Nonetheless, the use of questionnaires was the best alternative at that time, as it is a large study and because of the special isolation conditions in the vast majority of countries in the world due to COVID-19.
The results of this study suggest that 30 minutes of daily PA can mediate the relationship between body composition and anxiety and depression symptoms (mental health). Education regarding the daily practice of PA should be promoted as a public health message, as it leads to physical and mental benefits. Future studies should aim to prioritize these areas of research to better inform the public about the reduction of anxiety and depression symptoms from the daily practice of PA, even for short periods such as 30 minutes throughout the day.

