










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Probiotics were first described in the 1960s, but perhaps the definitive expression was offered in 2014, when the World Health Organisation defined probiotics as “live microorganisms which when administered in adequate amounts confer a health benefit on the host” (1).
After childbirth, the maternal flora predominates over environmental flora, playing an essential role in the development of the infant’s systemic and mucosal immunity. Bacteria promoting oxidative metabolism, such as Enterobacteriaceae, Streptococci and Staphylococci, are the first to proliferate in the gut.
It is widely accepted that breast milk should be the first feeding option for neonates, infants and, of course, premature infants. Breast milk is a complete food, from the nutritional, immunological and microbiological standpoint, and is a source of commensal or probiotic bacteria for the newborn’s intestine. Probiotic supplementation is considered a promising alternative means of simulating the microbiological characteristics of breast milk and thus achieving its associated beneficial effects. However, this belief must be based on solid scientific evidence of specific beneficial effects, obtained in properly designed clinical studies, in which the appropriate strain, dose and administration route are selected for the therapeutic goals addressed (2).
According to several recent studies, the composition of the neonate’s gut microbiota may be affected by gestational age and birth weight. Any alteration in this respect is an important risk factor for the development of necrotising enterocolitis (NEC), sepsis and increased mortality. Studies have also considered whether the appropriate supply of probiotics to premature infants reduces hospital stay and the time required to achieve complete enteral nutrition.
The aim of the present study is to compile evidence on the use of probiotics in preterm infants, and the impact on NEC, mortality, sepsis, and time to achieve complete enteral nutrition.
METHODS
This systematic review was performed via a search of websites presenting data on relevant clinical practice: the Cochrane Library, PubMed and MEDLINE databases. In PubMed, the MeSH terms used were “Infant, Premature”(Mesh) AND (“Infant, Very Low Birth Weight”(Mesh) OR “Infant, Premature/classification”(Mesh) OR “Infant, Premature/growth and development”(Mesh) OR “Infant, Premature/mortality”(Mesh) AND 2014(PDAT): 2021(PDAT) AND (English(lang) OR Spanish(lang)) AND (Clinical Trial(ptyp) OR Meta-Analysis (ptyp) OR Practice Guideline (ptyp) OR Randomized Controlled Trial (ptyp) OR Review (ptyp)) AND “Infant”(Mesh) AND “Probiotics”(Mesh).
Ethics committee approval was not required for this study.
The following selection criteria were applied: a) premature infants with less than 37 weeks’ gestational age or less than 2500 g birth weight; b) studies published during the period 2014 to 2021; c) studies focused on diagnosis or treatment; and d) comparison between intervention groups, with placebo or negative control.
The exclusion criteria were: a) articles in which there were no interventions with probiotics; b) articles in languages other than Spanish or English; c) studies dealing exclusively with animals; d) articles that presented insufficient data; and e) articles that did not differentiate between premature infants and other age groups.
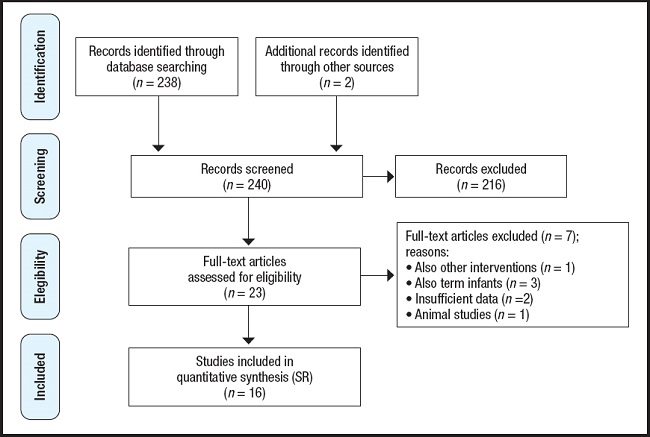
The probiotics identified in this review were various strains of Lactobacillus, Bifidobacterium, Saccharomyces, Streptococcus, Bacillus and others, used either in combination or in monotherapy, and compared with the administration of a placebo. The flow chart for the source selection process is shown in figure 1.
RESULTS
The literature search initially yielded 240 articles. After discarding duplicates and excluding unrelated articles (according to the document title and abstract), 25 papers remained, for which the full texts were obtained. Following application of the inclusion/exclusion criteria described, nine of these papers were excluded, leaving sixteen for the final analysis (Fig. 1).
The main results presented in these papers concerned the relation between the consumption of probiotics and the incidence of NEC, late sepsis, mortality, length of hospital stay and the time required to achieve complete enteral nutrition. The details of each study are summarised in table I.
Table I. Characteristics of the studies included in the systematic review.
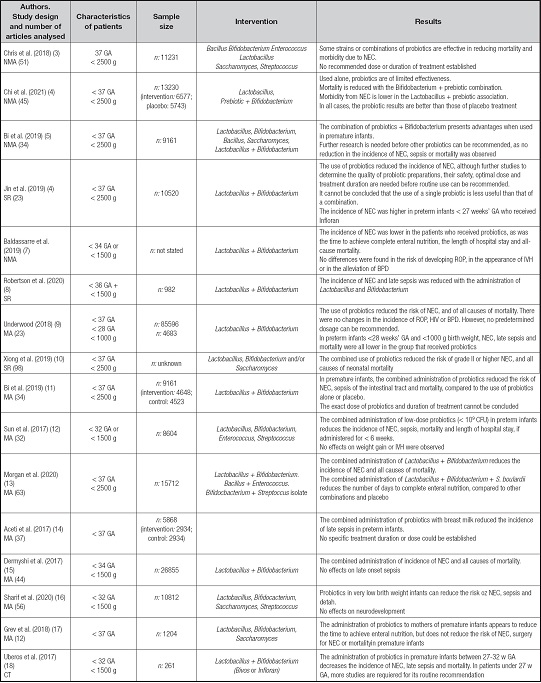
NMA: network meta-analysis. SR: systematic review. MA: meta-analysis. CT: clinical trial. GA: gestational age (weeks). NEC: necrotising enterocolitis. IVH: intraventricular haemorrhage. ROP: retinopathy of prematurity. BPD: bronchopulmonary dysplasia.
The meta-analyses reported by Chris et al. in 2018 (3) and Chi et al. in 2020 (4) described 96 studies and analysed the following variables: mortality, NEC, late sepsis and time to achieve complete enteral nutrition. Chris et al. (3) analysed 51 studies. In four of these (representing a total study population of 830 pre- mature infants), mortality decreased following the use of different strains of Bifidobacterium, Lactobacillus and S. thermophilus, with a relative risk (RR) of 0.17. The presence of grade II or higher NEC was reduced, with a RR that was significantly lower for seven treatments in which different strains of Lactobacillus and Bifidobacterium were combined. The RR for late sepsis was significantly lower with the Lactobacillus + Bifidobacterium combination, compared to placebo treatment. Similarly, the time required to achieve complete enteral nutrition was reduced when the following probiotics were supplied: L. reuteri; the combination of B. bifidum, B. infantis, B. longum and L. acidophilus; and the combination of B. longum and L. rhamnosus GG.
In 2020, Chi et al. (4) conducted a meta-analysis of 45 trials conducted between 2002 and 2018, with a total population composed of 12,320 premature infants with less than 37 weeks’ gestational age or less than 2500 g birth weight. The administration of Bifidobacterium and Lactobacillus reduced mortality rates (RR 0.56) and NEC (RR 0.47) compared to the placebo treatment.
The reviews by Bi et al. (5) and Jin et al. (6) both evaluated the impact on NEC in preterm infants given probiotics. The first of these reviews analysed 34 studies with a total population of 9,161 patients and reported that the risks of NEC (OR 0.38, 95 % CI 0.27-0.54), gastro-intestinal sepsis (OR 0.82, 95 % CI 0.69-0.98) and mortality (OR 0.54, 95 % CI: 0.42-0.71) were all significantly reduced after the administration of a combination of probiotics, especially those with Lactobacillus and/or Bifidobacterium, versus placebo treatment. Furthermore, there was a significant decrease in mortality in the preterm infants who received a combination of probiotics, compared to placebo treatment (OR 0.49, 95 % CI 0.32-0.69). In the second of these reviews, Jin et al. (6) examined various experimental studies, with a total population of 10,520 infants, and observed great variability in terms of the probiotic strains, doses and administration times described. These authors concluded that the combination of Lactobacillus rhamnosus GG and Bifidobacterium lactis Bb-12/B94 was effective in reducing NEC. Despite clinical heterogeneity, the conclusion of this cumulative meta-analysis was that probiotic treatment decreased the incidence of NEC (RR 0.53; 95 % CI 0.42-0.66). However, one of the trials in this review, focused on premature infants with less than 28 weeks gestational age, concluded that the routine use of “Infloran®” was associated with an increase in grade II or higher NEC (13.3 % vs 5.9 %, p = 0.010).
Baldasarre et al. (7) conducted an extensive literature search concerning the management of intestinal dysbiosis with probiotics, and the resulting impact on NEC. The results obtained indicate that the use of probiotics (Lactobacillus + Bifidobacerium) reduces the incidence of NEC in premature infants with less than 34 weeks’ gestational age or less than 1500 g birth weight, and also reduces the time to achieve complete enteral nutrition, as well as the incidence of late sepsis.
Another study, by Robertson et al. (8), examined the results obtained for a sample of 982 infants during a ten-year period (five before the routine use of probiotics in preterm infants, and five after their introduction), for NEC, late sepsis and mortality. The rate of NEC fell from 7.5 % (35/469 neonates) in the first period to 3.1 % (16/513 neonates) in the second (HR = 0.44, 95 % CI 0.23 to 0.85, p = 0.014), regardless of any other covariates, including breastfeeding. Similar, the rate of late sepsis decreased from 22.6 % to 11.5 % (p < 0.0001). With the introduction of routine probiotic administration, mortality (all causes) also fell, from 14.3 % to 9.2 %. Finally, the NEC-reducing effect was most pronounced during the two weeks of postnatal life.
In 2018, Underwood et al. (9) reviewed nine meta-analyses of controlled trials, from which they concluded that the use of probiotics reduced the incidence of NEC and mortality, but had no beneficial effect in preventing intraventricular hemorrhage (IVH), bronchopulmonary dysplasia (BPD) or retinopathy of prematurity (ROP). They also reported that in a subgroup of 4,683 extremely low birth weight neonates (< 1000 g), the administration of probiotics produced a significant reduction in NEC, mortality and late sepsis (HR for NEC 0.48, death 0.59, late sepsis 0.83). Similar findings were reported by Xiong et al. (10), who reviewed 98 articles in this context and observed a moderate decrease in the incidence of NEC (stage II or greater) and mortality after the administration of a combination of probiotics.
Bi et al. (11) analysed 34 studies with a total population of 9,161 patients. These authors found that different strains of Lactobacilli, Bifidobacteria, Bacillus, Saccharomyces and a combination of probiotics significantly reduced the incidence of NEC after the administration of probiotics, compared to placebo treatment (from 6.23 % to 3.54 %) (RR = 0.58, 95 % CI 0.48-0.69, p < 0.05).
For the probiotic combination group, the incidence of NEC (2.48 %) was approximately 40 % that of the placebo group (6.33 %) (RR = 0.40). Lactobacilli and Bifidobacteria, administered separately, also reduced the incidence of NEC compared to the placebo. In addition, the risk of sepsis was significantly reduced (probiotics group 15.59 %; placebo group 17.95 %), as was mortality (5.23 % and 7.41 %, respectively) (RR = 0.72, 95 % CI 0.61 to 0.85).
A meta-analysis by Sun et al. (12) of studies of preterm infants with less than 1500 g birth weight or less than 32 weeks’ gestational age reported that infants given probiotics achieved a 37 % reduction in NEC, 37 % in late sepsis and 20 % in mortality, as well as 3.8 days’ reduction in the length of hospital stay. These authors also reported that probiotics were more effective when taken with breast milk, when they were consumed for at least six weeks, when a dose of less than 109 CFU was administered, and when multiple strains were administered.
In 2020, Morgan et al. (13) reviewed 63 clinical trials of probiotic supplementation versus placebo treatment, finding that the combination of one or more strains of Lactobacillus spp. and Bifidobacterium spp. reduced all-cause mortality (OR 0.56, 95 % CI 0.39 to 0.80). Combinations of one or more strains of Lactobacillus spp. and one or more strains of Bifidobacterium spp., Bifidobacterium animalis subspecies lactis, Lactobacillus reuteri or Lactobacillus rhamnosus significantly reduced severe NEC. It was also observed that combinations of Lactobacillus spp. and Bifidobacterium spp and Saccharomyces boulardii reduced the number of days required to achieve full enteral nutrition (mean reduction: 3.30 days). The review found moderate or high-quality evidence that, compared to placebo, a single strain of B. animalis subspecies lactis or L. reuteri significantly reduced the length of hospital stay (mean reductions: 13 days, 95 % CI, 22.7 to 3.3 days; and: 7.9 days, 95 % CI 11.6 to 4.2 days, respectively).
In 2017, Aceti et al. (14) analysed the relationship between type of diet (breast milk or artificial milk) and probiotic supplementation, evaluating data from 5,868 neonates. Regardless of the type of diet, fewer cases of late sepsis were observed in the probiotic group (13.6 %) than in the placebo group (17.24 %) (RR 0.79). Moreover, the breastfed neonates who received one of the probiotic combinations showed fewer cases of late sepsis. In this review, the following probiotics were considered: Lactobacillus rhamnosus, Lactobacillus reuteri, Lactobacillus sporogenes.
Also, in 2017, Dermyshi et al. (15) reviewed 30 clinical trials and 14 observational studies and concluded that the administration of probiotics in premature infants reduced rates of NEC (grade II or higher) and all-cause mortality. In addition, the risk of sepsis fell by 12 % in the experimental studies and by 19 % reduction in the observational studies. By probiotic groups, the following results were obtained: Lactobacillus GG and Bifidobacterium lactis significantly reduced the incidence of severe NEC stage II-III; however, neither L. reuteri, B. breve nor Saccharomyces boulardii alone achieved a significant reduction in severe NEC. Subgroup analysis showed that combinations of two or more strains of probiotics were most beneficial in reducing the risk of NEC.
In 2020, Sharif presented a systematic review (16) of the use of probiotics to prevent NEC in very low birth weight preterm infants. This review examined 56 trials with a total population of over 10,000 infants. The most widely used probiotics were combinations of Bifidobacterium spp., Lactobacillus spp., Saccharomyces spp. and Streptococcus spp. The administration of probiotics reduced the risk of NEC, although at least 33 patients had to be treated for this beneficial effect to become apparent (NNTB 33, 95 % CI 25 to 50). On the other hand, this analysis concluded that probiotics may have little or no effect on severe neurodevelopmental impairment.
In 2018, in a related study, Grev et al. (17) conducted a review of probiotic supplementation for mothers aimed at preventing morbidity and mortality in preterm infants. The studies included in this review considered populations of pregnant women who received probiotics supplements from 36 weeks of gestation, or earlier, until delivery. The probiotics examined belonged to the Lactobacillus, Bifidobacterium and Saccharomyces genera. No significant differences were observed in the incidence of NEC or mortality, but in this case the quality of the scientific evidence generated was very low.
In 2017, our research group published a quasi-experimental study (18) on the use of probiotics in premature infants with less than 32 weeks of gestational age. The study aim was to determine whether routine supplementation with probiotics -L. rhamnosus GG (LGG) or L. acidophilus + B. bifidum- was associated with a reduced risk of severe NEC, in preterm infants with less than 32 weeks’ gestation. The results obtained showed that routine supplementation with LGG or L. acidophillus + B. bifidum was associated with a reduced risk of severe NEC, late-onset sepsis and mortality in preterm infants with less than 32 weeks’ gestation.
DISCUSSION
Current scientific evidence confirms the utility of different combinations of probiotics in the prevention of NEC and late neonatal sepsis in very low birth weight preterm infants. Achieving a good balance in intestinal microbiota can inhibit intestinal dysbiosis and regulate the immune response (19). The fact that preterm infants have a less developed immune system increases the risk of infections, NEC and morbidity-mortality (20).
Breast milk is the best nutrition for neonates, especially premature infants (21), protecting them against NEC and sepsis, and this effect is increased with probiotic supplementation. Very low-weight preterm infants may be immunologically more vulnerable, and so information regarding the efficacy, safety and possible side effects of the different strains used must be available before their routine use. However, the use of lactobacillus and bifidobacteria does not cause concern, because these strains normally reside in the gastrointestinal tract of healthy infants (2). Careful selection of the strain or strains used in probiotic supplementation will minimise the risk of side effects.
Evidence suggests that rates of NEC, late sepsis and mortality, and length of hospital stay and time required to achieve complete enteral nutrition all decrease with the use of probiotics. However, other variables such as IVH, ROP and BPD are not affected by this supplementation (7,9,12).
The meta-analysis by Chris et al., in 2018 (3), examined the use of different types of strains of Bacillus, Bifidobacterium, Enterococcus, Lactobacillus, Saccharomyces and Streptococcus, but was unable to establish the most suitable combinations or doses to reduce the incidence of NEC, mortality, length of hospital stay or time to achieve enteral nutrition. However, these authors did observe that the most commonly used probiotics were combinations of Lactobacillus and Bifidobacterium. Another meta-analysis, by Bi (5), concluded that although a combination of probiotics with Bifidobacterium seems to reduce the incidence of NEC, more studies are needed to determine which probiotic strain is ideal in preterm infants, as was also concluded by Jin (6). The use of Lactobacillus and Bifidobacterium during the first two weeks of postnatal life is a safe and inexpensive option, which also reduces the incidence of NEC (8). Studies have shown that 109 CFU seems to be a sufficient dose to achieve a beneficial effect (12), and that the combination of several strains of probiotics is the most effective means of reducing the risk of late sepsis and NEC (13,15-17).
The main limitation of the present study is the lack of detailed information regarding the analysis of each gestational age group, beyond the inclusion of premature infants with less than 37 weeks’ gestational age or less than 2,500 g birth weight. Without more extensive data, it is hard to determine the real benefit obtained from the use of probiotics in extremely low-weight newborns.
Nevertheless, it can be concluded that the administration of probiotics is safe and effective in reducing the risk of NEC, late sepsis and mortality, as well as the length of hospital stay and the time required to achieve complete enteral nutrition in premature infants. Furthermore, combinations of several strains of probiotics seem to be more effective than the administration of single strains. Those most commonly used are Lactobacillus and Bifidobacterium. At present, there is no clear evidence as to which strains should most appropriately be administered, nor for how long or at what doses.

