










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
While similar to eating disorders (EDs), disordered eating behaviors (DEBs) do not meet the criteria established in diagnostic manuals (1). They occur less frequently and intensely and have a shorter duration than the latter yet cause significant health problems and poor quality of life, in addition to being associated with the presence of other psychopathologies (2). Examples of DEBs include restrictive diets, binge eating, and the use of compensatory methods such as laxatives, diuretics, overexercising, anorexigenics, and self-induced vomiting.
Accordingly, instruments, questionnaires, and interviews have been designed and validated to obtain information on the prevalence of DEBs in Latin American children, adolescents, and youth. For example, Urzúa et al. (3) assessed disordered eating behaviors in Chilean students ages eight to eighteen through the Eating Attitudes Test-EAT-26 comprising twenty-six items. Encina et al. (4) used the Children’s Eating Behavior Questionnaire-CEBQ, consisting of thirty-five questions, in a sample of both Chilean children and their mothers/guardians, to determine whether they had positive or negative attitudes towards food intake. For their part, Cofré et al. (5) used the Three-Factor Eating Questionnaire (TFEQ-P19), adapted from the original version (6) to measure eating behaviors in a hundred Colombian children ages six to nine.
With regard to other instruments used to measure DEBs in children, in Mexico, Ponce de León et al. (7) validated the ChEAT (Children’s Eating Attitudes Test) in a sample of children and early adolescents with a mean age of eleven. However, this is an instrument developed in another culture, with twenty-six questions and six answer choices, which can prove hard for younger children to answer. Likewise, Platas and Gómez Peresmitré (8) designed and validated the Scale of Risk Factors Associated with Eating Disorders (EFRATA-II) in preadolescents aged nine to twelve, obtaining robust psychometric characteristics. However, this is an instrument with sixty-one questions with five answer choices, whose length makes it impossible to use in population studies.
The Brief Questionnaire for Measuring Disordered Eating Behaviors (BQDEB) was designed in 1997 to obtain information on the student population through the Survey on the Prevalence of Drug and Alcohol Use in the Student Population of the Federal District. It has been validated in adolescent girls (10), patients with eating disorders (9,11), adolescent boys and young men (12). It has been used to assess DEBs in six measurements of the Survey on Drug Use in Students, conducted in Mexico City (13-16), three editions of the National Health and Nutrition Survey (ENSANUT) (17-19) and one of the ENSANUT-continua (20). The need to measure DEBs in children ages eight to twelve led to the adaptation of the BQDEB, in which the number of questions was reduced, and answer choices simplified to make it easier to understand and answer.
The purpose of this study was therefore to obtain the reliability and exploratory and confirmatory factorial validity of the BQDEB in the version for children ages eight to twelve, 4th to 6th grade students at public elementary schools in the states of Campeche and Mexico. An additional objective was to report the percentage distribution of each of the questions in the questionnaire by sex.
MATERIALS AND METHODS
SAMPLE
The total sample comprised 386 children, eight of whom were eliminated, because they did not agree to participate, leaving a total of 378 (193 girls = 51.1 % and 185 boys = 48.9 %), elementary school students in the morning shift, at six schools in the federal school system of the Ministry of Public Education in the States of Campeche (249 girls = 51 %) and Mexico (129 girls = 51.2 %) in the period May-July 2022 through an Internet link. The mean age was 10.2 years (SD = 0.94), with no differences by sex.
INSTRUMENT
The BQDEB is a ten-item scale designed to assess disordered eating behaviors such as restrictive diets, binge eating, and the use of compensatory methods such as laxatives, diuretics, excessive physical exercise, anorexigenics, and self-induced vomiting (9,21).
For the present study, the questionnaire was adapted through cognitive laboratories with fifteen children ages eight to twelve to check the understanding of the terms included in the questions, the meaning of the latter, and the answer choices. This evaluation resulted in a seven-item instrument with three ordinal response options (No = 0, Sometimes = 1, Yes = 2) that evaluate behaviors in the last three months: 1) Have you been worried about gaining weight? 2) Have you sometimes overeaten or binged? 3) Have you lost control over what you eat (do you have the feeling of being unable to stop eating)? 4) Have you vomited after eating to try to lose weight? 5) Have you skipped breakfast, lunch, or dinner to try to lose weight? 6) Have you stopped eating certain types of food to try to lose weight? 7) Have you exercised to try to lose weight? A pilot study was subsequently conducted with the proposed version in which understanding of the items was tested in a group of ten children within the age range.
PROCEDURE
The researchers contacted local school authorities, who, after agreeing to participate in the study, liaised between the former and school principals. Questionnaires were administered by sending Internet links via WhatsApp, initially to the school principals, and subsequently to 4th to 6th grade elementary school teachers, who then forwarded them to parents. Teachers sent the internet link to parents, explaining that before answering the questions, they should read the informed consent form and decide whether they wished their children to participate. If they chose not to, that would indicate the end of their participation. Given that the children were asked to provide their informed consent, parents were asked to help them if they had problems understanding and answering the consent form, although the questionnaires were answered exclusively by the children.
DATA ANALYSIS
Frequency and percentage analyses were conducted, together with measures of central tendency of demographic variables and of each of the scale items. Reliability and exploratory and confirmatory factor analyses were also conducted.
Item-total correlations were obtained, considering that items with a value of less than .20 should be eliminated. An exploratory factor analysis was conducted based on Yela’s criteria; also a confirmatory factor analysis was conducted. The sample was randomly divided into two parts, yielding an initial sample of 197 subjects (ninety-six girls and one hundred and one boys) and a second sample with 181 subjects (ninety-seven girls and eighty-four boys), so that the exploratory analysis could be undertaken with one and the confirmatory analysis with the other, in both cases, the quota of five to twenty participants per item was achieved, and the minimum requirement of 150 subjects was met to conduct the confirmatory factor analysis. Reliability was obtained with ordinal alpha with the total sample (n = 378). The SPSS program version 21, the statistical program Factor, and the JASP program version 13 were used for the data analysis.
The protocol was approved by the Research Ethics Committee of the National Institute of Public Health on April 13, 2021, approval number 1542. Parents’ or guardians’ informed consent and children’s assent were included in the links to the questionnaires sent to parents.
RESULTS
DISORDERED EATING BEHAVIORS
The analysis by sex of DEBs in the “yes” answers showed that 3.1 % of girls and 11.9 % of boys are worried about gaining weight, 1 % of girls and 2 % of boys had binged, 2.1 % of girls and 5 % of boys had felt a loss of control when eating, 2 % of girls and 0 % of boys had avoided meal times to lose weight, 2.1 % of girls and 2 % of boys had stopped eating certain foods and 12.5 % of girls and 5.9 % of boys had exercised to lose weight. In the “sometimes” category, the answers were 40.6 % and 39.6 % in girls and boys, respectively, for concern over gaining weight; 44.8 % and 55.4 % in girls and boys, respectively, for binge eating; 24 % and 25.7 % in girls and boys, respectively, for feeling a lack of control when eating; 8.3 % in girls and 5 % in boys for avoiding meal times; 18.8 % in girls and 12.9 % in boys for refraining from eating certain foods; and 40.6 % in girls and boys for doing exercise. No statistically significant differences were found by sex.
FACTOR ANALYSIS
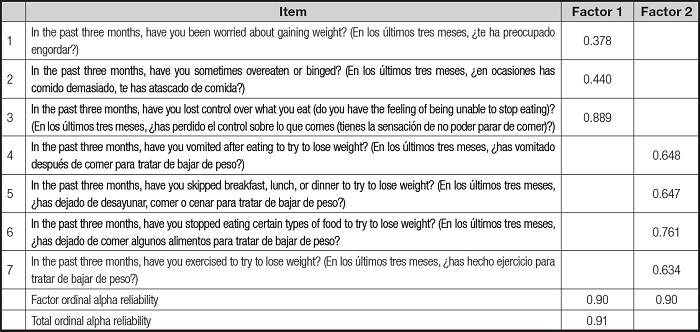
An exploratory factor analysis was performed with the seven items from the complete scale. The item-total correlations of the scale were obtained using ordinal alpha, showing that all the questions obtained loads higher than 0.20, except for question four: “Have you vomited after eating to try to lose weight?”, which would indicate the need to eliminate this item from a strictly psychometric perspective. However, due to its theoretical importance and mainly because it is a worrying behavior from a diagnostic point of view, it was decided to keep it for the confirmatory factor analysis without considering the psychometric values obtained in the item-total correlations.
With the remaining six items, exploratory factor analysis was conducted using unweighted least squares (ULS) type with Promin rotation. A configuration in two factors that explained 63.7 % of the variance, with a significant Bartlett’s test of sphericity (B = 176.60, df = 21; p < 0.001) and a value of 0.60 in the Kaiser-Meyer-Olkin (KMO) test. Factor 1, containing questions on compensatory behaviors or food restriction, obtained an ordinal alpha of 0.90, while Factor 2 contained questions on binge eating and feeling a lack of control while eating with an ordinal alpha of 0.90, and a total ordinal alpha reliability of the scale of 0.91 (Table I).
Tabla I. Factor weightings for the exploratory factor analysis of the Brief Questionnaire to Measure Disordered Eating Behaviors in Children.
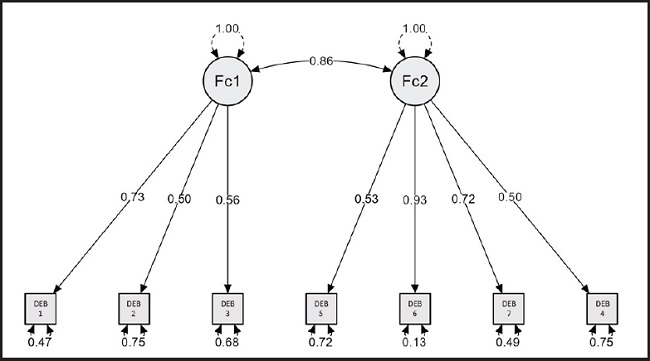
Confirmatory factor analysis was conducted with the JASP program, estimating discrepancies using the diagonally weighted least squares method (suitable for ordinal measurement levels). To conduct this analysis, item 4 was re-examined, to assess its fit with the final model. First, it was observed that discrepancies were not statistically significant. In addition, goodness of fit proved adequate, with values of RMSEA ≤ 0.08, CFI ≥ 0.95, TLI ≥ 0.90, GFI ≥ 0.90 and SRMR ≤ 0.08 being obtained.
Confirmatory factor analysis (Fig. 1) generally showed adequate goodness-of-fit indices (RMSEA = 0.000, 90 % CI [< 0.034]; CFI = 1.00; TLI = 1.02; GFI = 0.99; SRMR = 0.07; Chi² (χ2 = 7.16, df = 13, p = 0.89). Factor covariances are statistically significant (estimate = 0.85, Z = 8.5, p < 0.001) and there were no modification or residual covariance indices.
DISCUSSION
Although DEBs and EDs mainly occur in adolescence, they currently already occur at an early age between the ages of five and twelve (22). In addition, DEBs are extremely common in overweight and obese people, which increases the risk of developing EDs (23). Although there are instruments for EDs, it is necessary to have a self-applicable instrument for evaluating DEBs in children that is brief, easy to administer, and specifically designed for the Mexican population. This instrument was adapted from the version for the adolescent and adult population, which has been widely administered and validated in Mexico (13-20).
When DEBs were evaluated, the most frequent behavior that emerged was concern over gaining weight, with 3.1 % of girls answering “yes” and 40.6 % “sometimes,” 11.9 % of boys answering “yes” and 39.6 % “sometimes.” This concern has been reported in other studies. In ENSANUT 2012, in the group ages ten to thirteen, it occurs in 11.4 % of boys and 11.3 % of girls (17). In another study of children ages eight to twelve with obesity in the United States, 31.7 % of subjects, including 25 % of boys and 37.7 % of girls have this characteristic (24). In regard to binge eating, 1 % of girls answered “yes” and 44.8 % “sometimes”; 2 % of boys answered “yes” and 55.4 % “sometimes” In ENSANUT 2012 (17), 10 % of boys and 9.9 % of girls reported binge eating. In regard to loss of control when eating, 2.1 % of girls answered “yes” and 24 % “sometimes”; 5 % of boys answered “yes” and 25.7 % “sometimes;” in the ENSANUT 2012 (17), 5.8 % of girls and 7 % of boys did so. The ENSANUT 2018 found that 3.9 % and 0.4 % of the group ages ten to eleven showed a moderate or high risk of eating disorders respectively (25). In Jalisco, Mexico, in a study with non-probabilistic, intentional sampling (26), the set of abnormal behaviors and attitudes as regards eating in children with an average age of 10.9 years was present in 13.8 % of subjects, being higher in those with overweight, 22.9 %, and obesity, 15.9 %. Other behaviors and attitudes found in studies of children ages eight to twelve show the presence of the thin ideal in 42 % of boys and 53 % of girls. Thirty-two per cent would prefer to be thinner, even those with normal weight, and 18.5 % were attempting to lose weight (27). Eating food without being hungry, having a high BMI, weight-related cognitions, and negative affect in childhood predict the presence of binge eating disorders in adolescence (28). The presence of DEBs reported in several studies varies partly as a result of the questionnaire administered and the age of the subjects. A number of studies have confirmed that the older the subjects and the higher their BMI, the greater the presence of DEBs (26-29).
Our reliability analysis was satisfactory for all the questions with the exception of question four, “Have you vomited after eating to try to lose weight?” However, the item was retained because of its theoretical importance. The seven questions were grouped into two factors unlike the version for adolescents and adults, comprising three factors. Factor one (compensatory behaviors-restriction) contains questions on compensatory behaviors or food restriction, whereas factor two (binge eating) comprises questions on binge eating and feeling a lack of control when eating, and concern over gaining weight. Results are consistent with DEBs that occur more frequently in the nine-to-twelve-year age group, since those under thirteen engage less in compensatory behaviors, binge eating, and the use of pills and laxatives than those over thirteen (30). The confirmatory factorial analysis performed yielded adequate goodness-of-fit indices and all items presented statistically significant loads in their factors.
Early cases of eating disorders or psychological risk factors probably go undetected in the child population, meaning that cases fail to receive medical attention until they are severe (31). Moreover, various screening studies for EDs in the child population have found the lack of validated instruments for this specific population group to be a major limitation (32-33). It is therefore essential to have instruments that can be used in epidemiological studies to detect DEBs at an early age, since research has found both avoidant and restrictive food intake disorder (ARFID) and other EDs among the pediatric population (32,33). These instruments should also be able to significantly decrease the presence of serious problems in adolescence.
Limitations of the study included the fact that the sample was neither random nor representative of the child population ages eight to twelve in Mexico, and the questionnaire is not sufficient to establish a diagnosis, validations of the scale should be undertaken on its self-reported version in other contexts, which would shed more light on the risk of DEBs in the child population, as well as convergent, divergent, predictive, test-retest validation and a comparison with clinical samples. Nevertheless, the version of the BQDEB for children constitutes a useful instrument for determining the extent of DEBs in children. One of the greatest advantages of the BQDEB for children in relation to other instruments used to detect DEBs is that it is a brief, specific, ideal for epidemiological studies and designed for the Mexican population, enabling one to determine prevalence, attend cases in a timely manner, and undertake preventive actions with better results.

