










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The period of transition from childhood to adolescence is a critical stage in the life course, marked by physical, cognitive, and emotional growth and a readiness to adapt and reshape one's social environment. However, prioritizing research in this area is essential to ensure optimal developmental outcomes, as this period remains understudied regarding growth and nutrition interventions and policies (1,2). Recent studies indicate that dietary interventions alone may not lead to lasting weight management, especially given the increasing prevalence of obesity and associated health risks (3,4). Instead, psychological approaches are recommended alongside dietary interventions to prevent or mitigate obesity (4,5).
Research confirms that behavioral strategies, particularly those enhancing satiety awareness, improve eating habits (6,7). Mindfulness, in particular, is well-supported in adult studies for its positive impacts on psychological well-being, self-compassion, concentration, and mental clarity (8,9). Mindfulness in children has also shown effectiveness in enhancing mental and physical health by reducing test anxiety, improving concentration, fostering social-emotional development, and aiding in managing eating disorders (9,10).
Mindfulness-based interventions are a scientifically supported, safe, and cost-effective approach to managing stress, as chronic stress has been found to increase unconscious eating habits and energy-dense food consumption (11,12). In children, stress can manifest in emotional eating, binge eating, external eating, and mindless eating, which are often coping mechanisms. These behaviors share adaptive characteristics but, if left unaddressed, can lead to serious consequences. Thus, strategies to reduce stress in children are essential (5,8).
As adolescents begin to experience physical changes and an increased interest in diet, non-diet health approaches are gaining attention, particularly those that avoid focusing solely on weight loss (6,11). Through mindfulness, individuals can develop mindful eating practices, engaging fully in the eating experience without judgment, which research supports as promoting healthy eating habits, stress reduction, and self-compassion (7,10). Mindfulness encourages a positive relationship with food, fostering body acceptance and enhancing awareness of hunger and fullness cues. However, research on mindfulness, nutrition, and stress in children remains limited, and this study aims to examine the relationship between emotional eating and perceived stress in children, with mindfulness as a mediating factor.
METHODS
RESEARCH PLACE, TIME AND SAMPLE SELECTION
The study included 328 children. The sample was carefully selected to ensure accurate representation of the population. The survey questions collected a comprehensive range of data, including participants' sociodemographic information, anthropometric measurements, general health status, eating habits, number of main meals and snacks consumed daily, meal skipping status, reasons for skipping meals, and dietary motivations. The questionnaire also included the BAU Mindfulness Scale for Children (BAU-MSC), the Emotional Eating Scale for Children and Adolescents (EES-C), and the Perceived Stress Scale in Children (8-11 years) (PSS-C). The survey was administered in person and took approximately 15 minutes to complete.
ANTHROPOMETRIC MEASUREMENTS
Body weight was measured using a calibrated precision scale sensitive to 0.5 kg, and height was measured on the Frankfort plane with feet side by side, following the method described by Lohman et al. (13). BMI for age was evaluated according to the World Health Organization (WHO) z-score cut-off points, as outlined by de Onis et al. (14). Body mass index for age was evaluated using the World Health Organization cut-off points (< -3 SD, < -2 SD, > 1 SD, > 2 SD, > 3 SD) as of 2018.
MINDFULNESS SCALE FOR CHILDREN (BAU-MSC)
The items of the scale designed to create a mindfulness measure based on the fundamental elements of the concept, relying on Kabat-Zinn's (1994) definitions of mindfulness, were inspired by various sources such as publications on mindfulness and previously cited definitions of mindfulness (15,16). The Mindfulness Components Questionnaire was developed by Mellor and colleagues (17). The BAU-MSC applies this principle and is designed as a 3-point Likert scale (1 = never, 2 = sometimes, and 3 = always). All items in the study are understandable practices for children without mindfulness or meditation experience. High scores indicate high mindfulness. The 3-point Likert scale is claimed to be developmentally appropriate and reliable for children (17). The BAU-MSC applies this principle and is designed as a 3-point Likert scale (1 = never, 2 = sometimes, and 3 = always), making all items accessible to children without prior mindfulness experience.
EMOTIONAL EATING SCALE FOR CHILDREN AND ADOLESCENTS (EES-C)
The Emotional Eating Scale for Children and Adolescents is a highly effective tool for evaluating emotional eating in children and adolescents aged 10-18 (18). The scale consists of 26 items, with the happiness item excluded from scoring. The restless mood subscale is composed of items 1, 2, 3, 4, 15, and 25, while the depressive symptoms subscale includes items 5, 6, 12, 16, 18, 19, and 26. The anxiety-anger-disappointment sub-dimension is represented by items 7, 8, 9, 10, 11, 13, 14, 17, 20, 21, 22, 23, and 24. The scale yields a minimum of 25 and a maximum of 125 points, with evidence indicating that higher scores correlate with increased emotional eating in response to negative mood (19).
PERCEIVED STRESS SCALE IN CHILDREN (8-11 YEARS) (PSS-C)
White et al. (2014) developed a 9-item scale for evaluating stress levels in children (20). Each child is asked to rate the appropriateness of each item for the past week using a 4-point Likert scale (never = 1, sometimes = 2, often = 3, always = 4). Higher scores indicate higher stress levels. The scale yields a minimum of 9 and a maximum of 36 points, with no reverse-coded items. The original scale reports an internal consistency reliability coefficient of 0.76, as measured by Cronbach's alpha, and a test-retest correlation of 0.79 (20).
ANALYSIS OF DATA
Statistical analyses were conducted using the SPSS 23.0 software package (IBM SPSS Statistics). The findings were interpreted using frequency tables and descriptive statistics. Parametric methods were used for measurement values that were normally distributed. Independent two-sample t-test was applied when there were two groups, and one-way analysis of variance (ANOVA) was applied when there were more than two groups. Homogeneity of variances was assessed using Levene's test statistic. Multiple comparison tests were conducted on data that met the homogeneity of variances condition. For comparisons of three groups, LSD tests were used, while Bonferroni tests were used for comparisons of more than three groups. Tukey tests were used for comparisons of groups with equal sample sizes. Pearson correlation analysis was employed to investigate the relationship between measurement values. The correlation coefficients can be interpreted as follows: r = 0 indicates no relationship, r = 0.01-0.29 indicates a weak relationship, r = 0.3-0.7 indicates a moderate correlation, r = 0.71-0.99 indicates a high level of correlation, and r = 1 indicates an excellent relationship level. The analysis results were interpreted using a 95 % confidence level and a 0.05 significance level for comparison tests, and 0.05 and 0.01 significance values at 95 % and 99 % confidence levels for correlation tests.
RESULTS
Table I displays the demographic characteristics of the students and the distribution of their general health status. The data shows that out of 349 students, 128 (36.68 %) were male, 221 (63.32 %) were female, and 74.5 % were in the 6th grade. The students' average age was 10.6 ± 1.32 years, with girls at 10.7 ± 1.12 years and boys at 10.6 ± 1.21 years. The average weight was 47.1 ± 12.92 kg for girls and 44.8 ± 10.13 kg for boys, with a total of 45.6 ± 11.23 kg. The average height for all students was calculated to be 154.1 ± 10.10 cm, with girls at 154.1 ± 11.02 cm and boys at 154.1 ± 9.53 cm (Table I). BMI z-score lower value is 12.55 and upper value is 29.30; the lower BMI z-score value of boys was found to be 12.96 and the upper value was 26.26.
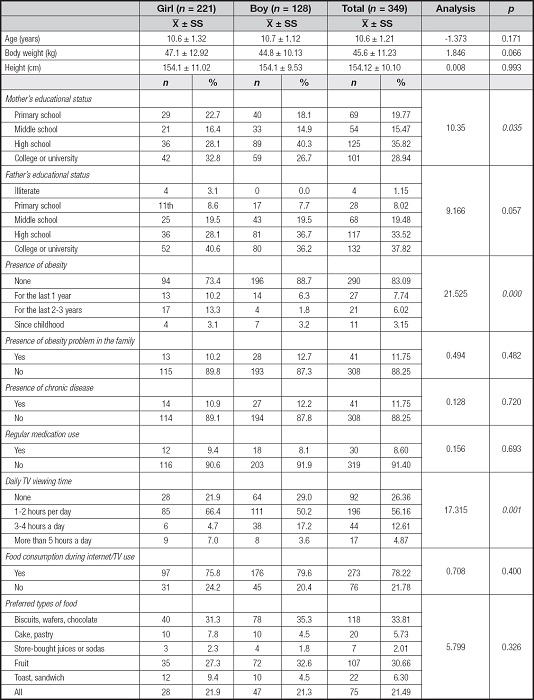
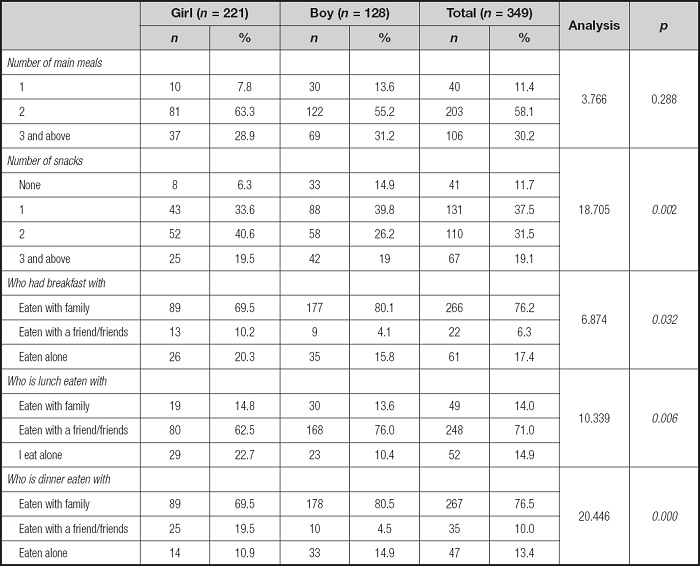
In all, 58.17 % of the participants had two main meals, while 30.2 % had three or more. Additionally, 37.5 % reported consuming one snack, and 31.5 % reported consuming two. In terms of meal locations, 68.77 % reported eating breakfast at home, 50.4 % reported eating lunch in the school canteen, and 69.6 % reported eating dinner at home (Table II).
Descriptive findings consisting of students' answers to the measurement tools are given (Table III).
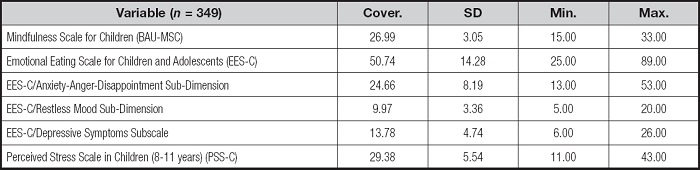
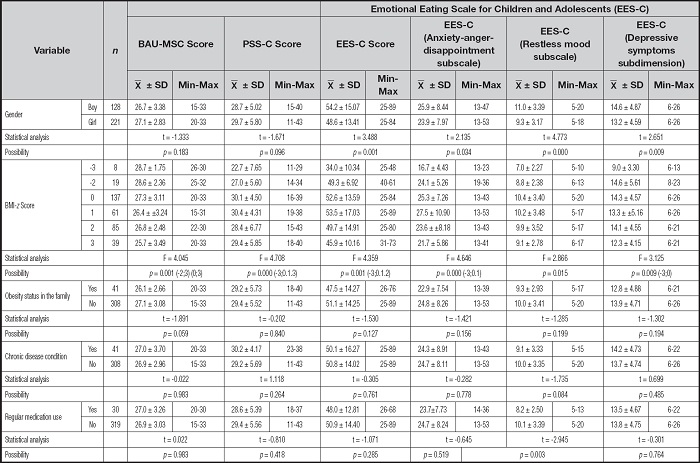
Table IV presents the participants' scores on BAU-MSC, EES-C, and PSS-C, including their subscales, as well as the analysis results regarding gender, BMI class, family history of obesity problems, chronic disease diagnosed by a doctor, and regular medication intake. The results indicate a statistically significant difference in the scores of all sub-dimensions of EES-C based on gender (t = -3.488; 2.135; 4.773; 2.651, p < 0.05). Statistically significant differences were found in terms of body mass index groups and all scale scores (F = 4.045; 4.708; 4.359; 4.646; 2.866; 3.125, p < 0.05). A statistically significant difference was found only in terms of the availability of regular medication and the EES-C/restless mood subscale scores (t = -2.948, p < 0.05) (Table IV).
Table IV. Analysis of the scores of BAU-MSC, PBB-C, EES-C and its sub-dimensions and some demographic information.
p < 0.05.
X̅: mean; SD: standard deviation.
*Parametric methods were used for measurement values that comply with normal distribution. In accordance with parametric methods, “Independent Sample-t” test (t-table value) is used to compare the measurement values of two independent groups; “ANOVA” test (F-table value) method was used to compare three or more independent groups. LSD and Bonferroni correction were applied for pairwise comparisons of variables with significant differences for three or more groups.
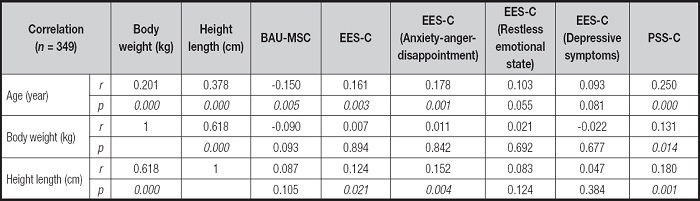
Table V examines the relationship between participants' scores on BAU-MSC, EES-C, PSS-C, and their subscales, and the variables of age, body weight, and height. Additionally, a moderately statistically significant positive relationship was found between body weight and height (r = 0.618; p = 0.000). A weak but statistically significant positive correlation was observed between height and the anxiety-anger-disappointment sub-dimensions of the EES-C, as well as the EES-C scores (r = 0.124; r = 0.152; r = 0.180; p = 0.021; p = 0.004; p = 0.001) (Table V).
DISCUSSION
This study offers comprehensive insights into the factors influencing emotional eating, mindfulness, and the impact of media usage on eating behaviors among children and adolescents. Emotional eating has been well-documented as a strategy to cope with stress, with high EES-C scores often indicating increased food intake as a response to emotional distress (18). Numerous studies have found that emotional eating is more prevalent among females, potentially due to greater emotional sensitivity and societal pressures related to body image and eating habits (21,22). However, our findings show that boys scored higher across all EES-C sub-dimensions, challenging traditional understandings and suggesting that age and other sociodemographic factors may play a significant role. Geliebter & Aversa (2003) have noted similar age-related variances in emotional eating patterns, highlighting the complex interplay between developmental stage and eating behavior (23).
Additionally, the relationship between BMI and emotional eating remains intricate. In previous studies, emotional eating scores often correlate positively with higher BMI values (19,24), suggesting that individuals prone to emotional eating may consume more calorie-dense foods, leading to weight gain over time. However, in this study, children with normal BMI-z scores demonstrated higher emotional eating tendencies than their obese peers. This deviation could be attributed to psychological factors that influence emotional eating independently of BMI or body composition, such as social support and coping strategies, which have been identified as potential mediators (25). Bryant et al. (2007) also argue that external influences, including family dynamics and stress management resources, can shape eating behaviors in ways that are not always reflected in BMI (26).
Mindfulness as a tool for emotional regulation has gained considerable attention, particularly for its application in managing emotional eating. The high BAU-MSC scores observed in this study suggest that children who practice mindfulness may have greater self-awareness and control over their emotional responses, reducing their reliance on food as a coping mechanism. Mindfulness-based interventions, such as those discussed by Kristeller & Wolever (2010) and Katterman et al. (2014), have shown significant promise in reducing binge eating and emotional eating in both adolescents and adults, with benefits extending to improved emotional resilience and self-regulation (27,28). Kumar et al. (2017) found that adolescents participating in a mindful eating program experienced reductions in BMI and emotional eating after structured sessions, supporting the view that mindfulness can serve as a protective factor against emotional dysregulation (29).
The integration of mindfulness into school curriculums provides a promising avenue for promoting healthier emotional and eating behaviors. Embedding mindfulness practices in classroom settings, as demonstrated by Bockmann et al. (2016), can enhance executive functioning, attention, and emotional regulation, which are crucial for developing resilience to stressors (30). The results from this study align with the findings of Kabat-Zinn (1994), who highlighted that mindfulness practice enhances the ability to navigate emotional experiences without resorting to maladaptive coping strategies (15). Given that mindfulness programs can be adapted for different age groups and educational settings, expanding these interventions to more schools could be beneficial in fostering healthier lifestyle choices and psychological well-being in children.
Media and technology use is another critical factor influencing eating behaviors, with increasing screen time being linked to higher consumption of calorie-dense snacks (31,32). The findings in table II reflect that a large proportion of children frequently consume packaged snacks such as biscuits and chocolate while engaged in screen-based activities. Media exposure, particularly advertising, has been shown to influence children's preferences for unhealthy foods, contributing to unhealthy snacking habits and, potentially, long-term health risks like obesity (33). Robinson et al. (2017) emphasize that the combination of media exposure and snacking disrupts regular eating patterns and could interfere with the development of mindful eating habits, particularly among younger children who may have limited awareness of advertising influence (32).
The limitations of this study, including its cross-sectional design and relatively small sample size, must be acknowledged. As this study captures a snapshot of emotional eating, mindfulness, and media usage at a single point in time, it does not allow for causal inferences. Expanding future research to include longitudinal methods would provide a more in-depth understanding of how these behaviors evolve over time. Larger sample sizes and diverse demographic groups would also improve generalizability, as indicated by Twenge & Nolen-Hoeksema (2002), who advocate for comprehensive samples in behavioral studies (34). Additionally, incorporating diagnostic assessments of psychological health could deepen insights into the psychological drivers behind emotional eating and stress coping mechanisms in children.
These findings underscore the importance of a multifaceted approach to addressing emotional eating and its associated risk factors. The incorporation of mindfulness-based interventions, coupled with awareness around media usage and healthier snack alternatives, could form the basis of effective public health strategies aimed at reducing emotional eating and promoting overall well-being among young populations. Further research will be invaluable in refining these strategies and understanding their long-term impact on children's mental and physical health.
CONCLUSIONS
Mindfulness-based studies will undoubtedly make significant contributions to the literature in the field of child and adolescent nutrition. It is crucial to emphasize the importance of research with larger sample groups. Integrating mindfulness-based eating interventions into the school curriculum is an effective way to promote healthy eating habits and support children's cognitive and emotional development. Limiting media and technology use and encouraging healthy habits can help prevent obesity and emotional eating behaviours. Parents and educators must support children by informing them about this issue. Providing psychological support and counselling services to children and adolescents for the management of emotional states such as stress, anxiety and depression is also crucial. This will reduce emotional eating behaviours and increase their overall psychological well-being. These recommendations will contribute to promoting healthy eating habits among children and adolescents and developing strategies to manage emotional eating behaviours.
Ethical approval:
ethical approval (Decision No: 177) was obtained from the Ankara Medipol University Non-Interventional Ethics Committee on December 25, 2023, and necessary permissions were obtained from the Provincial Directorate of National Education. The participation of each child and their family in the research was voluntary.

