










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
One of the targets of the third entry in the Sustainable Development Goals (SDGs) is to ensure a healthy life and promote well-being for all people at all ages. One of them is improving maternal health and reducing the maternal mortality rate (MMR). SDGs target for MMR is to be 70 per 100,000 live births (1). The nutritional problem in pregnancy faced by Indonesian people is chronic energy deficiency (2). Malnutrition in pregnant women will cause impaired fetal development, premature delivery, impaired baby growth, and the risk of causing chronic disease (3). The direct causal factors for pregnant women at risk of chronic energy deficiency (CED) are insufficient nutritional consumption and infectious diseases (1).
Based on data sources for routine reports in 2022, collected from 34 provinces, it is known that there are 283,833 pregnant women with mid-upper arm circumference < 23.5 cm (CED risk) out of all 3,249,503 pregnant women measured, so it is known that the outcomes of pregnant women with CED risk are 9.7 %, while the 2021 target is 16 % (4). Based on data from the Central Bureau of Statistics for East Java Province in 2020 the prevalence of pregnant women with CED in East Java is 53,455 (11.5 %) of 618,207 pregnant women (5). Based on the Health Profile of Jombang Regency in 2020, in Jombang Regency 2,224 pregnant women (9.40 %) experienced CED out of 20,921 pregnant women (6).
During pregnancy, the mother must meet her nutritional needs so that her pregnancy is successful in a healthy behavior. Inadequate nutritional intake during pregnancy cannot only cause fetal growth disturbances but is feared to also reduce milk production (7). There are factors that affect the nutritional status of CED pregnant women such as diet, food consumption, economic status, health status, and internal factors such as excessive workload and poor nutritional knowledge (8). Pregnant women who have a good and quite diverse diet will certainly have their nutritional needs met during pregnancy, because the food consumed is in accordance with the nutrients needed (9).
Nutritional problems are a preventable cause of maternal and child mortality through nutrition management in Indonesia (10). Food selection and dietary habits are influenced by knowledge, attitudes toward food, and nutritional knowledge practices or the behavior that underlies food selection. Nutritional needs during pregnancy will increase by 15 % compared to normal women's needs (11). The nutritional needs of pregnant women are very complex, thus to meet such needs additional macro and micronutrients are needed. Almost all developing countries have provided macro and micro nutritional supplements to pregnant women. This administration is carried out singly, for example iron (Fe), zinc, calcium or a combination of iron and folic acid, as well as in additional food (12).
Developed in the 1950s by Godfrey Hochbaum, Irwin Rosenstock, S. Stephen Kegeles, and Howard Leventhal, the health belief model (HBM) is the most frequently used model and plays an important role in directing a person to engage in preventive health behaviors (13). Nutritional problems often arise because people have inadequate knowledge, beliefs, values or norms (14). Some dietary restrictions during pregnancy still exist, such as the belief that certain foods will result in difficult births for the fetal head, abortion, obese babies and stillbirth (15). The perceived susceptibility factor indicates pregnant women who perceive themselves as highly susceptible to experiencing negative health outcomes due to poor nutrition are more likely to engage in healthy eating behaviors (16). The perceived severity of the potential consequences of inadequate nutrition is also a significant predictor of nutritional fulfillment behavior (17). Related to perceived benefits research shows women who believe that healthy eating during pregnancy will lead to positive outcomes (e.g., a healthy baby) are more likely to adopt healthy dietary practices (18). Barriers to healthy eating, such as lack of access to healthy foods, financial constraints, or cultural food preferences can negatively impact nutritional fulfillment behavior (19). Cues to act on factors from research show that external cues like doctor's recommendations, family support, and educational programs can effectively motivate pregnant women to prioritize nutritional needs. The HBM concept is that health behavior is determined by individual beliefs or perceptions about diseases or health conditions, and the strategies available to reduce their occurrence (20). The HBM theory is based on six components, namely perceived susceptibility, perceived severity, perceived benefits of action, perceived barriers to action, self-efficacy, and cues to action.
REVIEW OF THE LITERATURE
Past research on pregnant women in Kalimantan showed that the factors associated with the incidence of anemia in pregnant women were pregnancy spacing, economic status, family support and nutrient intake (21). Previous research on mothers regarding the fulfillment of nutrition in children using the theory of health belief model shows that perceptions of vulnerability and perceived seriousness do not affect the behavior of mothers in meeting the nutritional needs of their children. The higher the perceived resistance, the worse the mother's behavior in fulfilling nutritional needs. The level of cues to action factors does not affect the mother's behavior in meeting the nutritional needs of her child nor does mother's self-confidence/ability (22). The conclusion of this study states that the mean score of the health belief model construct in pregnant women was moderate. Based on this finding, the study recommends implementing an educational program based on the health belief model to improve the health of mothers and their children. The program aims to enhance the sensitivity and perceived severity of health workers regarding the health of pregnant women, increase their self-efficacy and perceived benefits, and reduce perceived barriers (23). Some of the key findings of the study include the importance of community support and the role of traditional birth attendants in women's decision-making around seeking care. The study also found that women's beliefs and attitudes toward pre-eclampsia and eclampsia were shaped by their previous experiences with pregnancy and childbirth, as well as their social and cultural contexts. Finally, the study identified several barriers to care-seeking, including financial constraints, lack of transportation, and poor quality of care at health facilities (24). This study aims to analyze the factors related to the nutritional fulfillment behavior of pregnant women based on the theory of the health belief model.
MATERIALS AND METHODS
RESEARCH QUESTION
What are the factors related to the behavior of meeting the nutritional needs of pregnant women based on the theory of the health belief model?
SAMPLE AND SETTINGS
The population is all pregnant women in the Working Area X Regency in December 2022, totalling 280 people. This study used simple random sampling with a total sample of 164 pregnant mothers in the Megaluh area with the stages of identifying the population then determining the sample size using the Slovin formula (25) with a confidence interval of 0.05, then using the lottery method to determine the sample taken, and finally taking data from the sample.
VARIABLES/INSTRUMENTS
The demographic data questionnaire consists of eight questions including mother's age, mother's education, mother's occupation, gravidity, mother's gestational age, husband's education, husband's occupation and husband's income. Then the nutritional status of the mother is calculated from the body mass index. The health belief model questionnaire uses a questionnaire from Hupunau with a total of 33 questions consisting of six sections, namely six questions on perceived susceptibility, six on perceived severity, five on perceived benefits, five on perceived barriers, six on self-efficacy, and five on cues to action using a Likert scale with answer choices consisting of statements that strongly disagree, disagree, agree, and strongly agree (22). The behavioral questionnaire for fulfilling nutritional needs in pregnant women using the Hupunau questionnaire consists of 10 questions with the answers always, often, sometimes and never. All questionnaires used have been tested for validity with the product moment correlation formula with a value of r > 0.5 and reliability test with Cronbach's alpha coefficient > 0.8.
DATA COLLECTION
The research data collection was carried out during the class activities for pregnant women at the X public health center when the respondent was doing antenatal care, then the respondent filled out the questionnaire that had been provided.
DATA ANALYSIS
After the data collection was completed, each questionnaire was checked visually for completeness. Data were entered, cleaned, and coded using SPSS version 16. Normality testing was conducted using the Kolmogorov-Smirnov test and the results indicated a non-normal distribution of data. Therefore, the Spearman rho test was employed. The results are presented descriptively with a frequency table and analytically with the Spearman rho statistical test at a significance level of α ≤ 0.05.
RESULTS
Data on the demographic characteristics of these respondents explained the characteristics of the respondents studied, as many as 164 people. The data discussed included mother age, level of education, occupation, gravidity, gestational age, and nutritional status, while data regarding the husband includes level of education, work, and income.
Based on table I, regarding the characteristics of the respondents, the age of the majority of respondents was in the range of 20-35 years, with 121 mothers (73.8 %). Mother education level shows that most of the 110 mothers are high school graduates (67.1 %). Most of the respondents are housewives, with 104 mothers (63.4 %). The first pregnancy or primigravida condition was met by 100 mothers (61.0 %). More than half of the mothers were in the second trimester of pregnancy (88 mothers, 53.7 %). Most mothers also had a good nutritional status (95 mothers, 57.9 %). Based on table I, regarding husband characteristics, most were high school graduates (94 people, 57.3 %). Having employment status as private employee corresponded to as many as 65 people (39.6 %). Most family incomes were less than the regional minimum wage in this city, which affected as many as 109 people (66.5 %).
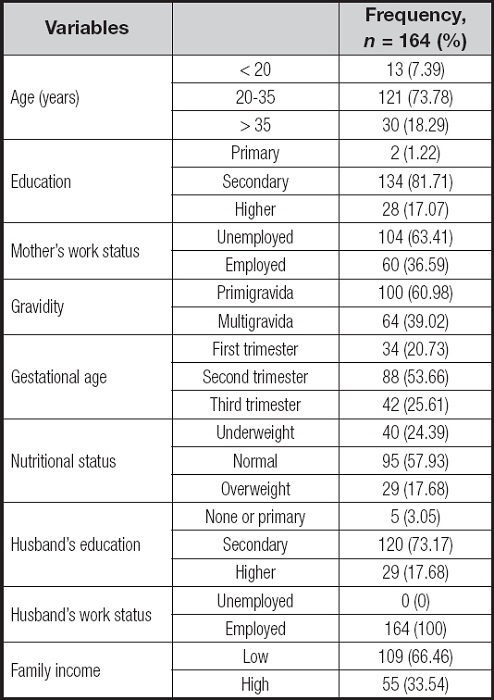
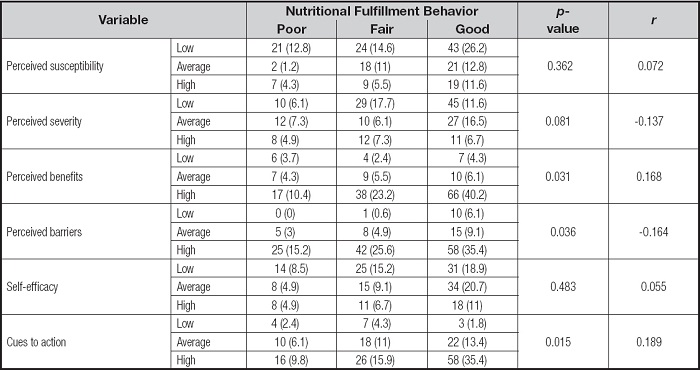
Table II shows the results of the statistical analysis using Spearman's rho correlation test with a significance level of < 0.05; the variables related to nutritional fulfillment behavior are perceived benefits (p = 0.031, r = 0.16), perceived barriers (p = 0.036, r = -0.164) and cues to action (p = 0.015, r = 0.189).
DISCUSSION
The results showed that there was a significant relationship between the nutritional needs fulfillment behavior of pregnant women and their perceived benefits. That is, the higher the level of fulfillment of nutritional needs carried out by pregnant women, the greater their perception of the benefits they get from meeting these nutritional needs. Previous studies have shown that meeting proper nutritional needs during pregnancy has a positive impact on maternal health and fetal development (26). However, even though knowledge about the importance of nutrition during pregnancy is expanding, not all pregnant women apply it in their daily lives. Higher perceived benefits can be a motivating factor for pregnant women to consistently involve themselves in behavior to fulfill nutritional needs. They may feel motivated to eat healthy foods, follow nutritional advice provided by medical professionals, or take recommended supplements during pregnancy. Perceived benefits of this can influence the attitudes and behavior of pregnant women related to meeting nutritional needs.
High perceived benefits means that respondents feel there are benefits from the behavior of fulfilling their nutritional needs, but, in this study, even though the perceived benefits are high, the behavior of meeting their nutritional needs is still lacking. Perceived benefits are the belief that someone will get benefits if they take health actions for a particular disease. The greater the benefits felt from a preventive action, the greater the chance for someone to take action to prevent disease (27).
However, from the findings of researchers on respondents who have high perceived benefits, it is found that the behavior of pregnant women is good in fulfilling their nutritional needs. This may be caused by several factors, including personal experience. This is in accordance with research conducted by Aristi, which states that a person's response to a stimulus will be different because it is influenced by several factors such as personal experience, culture, people who are considered important and the mass media (28). If people believe that certain actions will reduce vulnerability to malnutrition or reduce the seriousness of disease, they are more likely to engage in the behavior, regardless of objective facts about the effectiveness of the behavior.
The results of this study indicate that there is a significant relationship between the nutritional fulfillment behavior of pregnant women and perceived barriers. The importance of meeting nutritional needs during pregnancy is a crucial factor in maintaining maternal health and fetal development. However, many pregnant women face barriers or perceived barriers in carrying out optimal nutritional fulfillment behavior. Perceived barriers refer to individuals' subjective perceptions of the barriers or obstacles they may face in carrying out certain behaviors. In this context, perceived barriers refer to the obstacles faced by pregnant women in fulfilling their nutritional needs. Pregnant women who face high perceived barriers tend to be more likely to experience difficulties in carrying out optimal nutritional fulfillment behaviors. Factors such as limited accessibility to nutritious food, lack of knowledge about nutritional needs during pregnancy, and social barriers such as lack of support from the family or the surrounding environment can be significant perceived barriers.
From the data, it can be seen that, even though the respondents have high perceived barriers, there are still more people who have good nutritional needs fulfillment behavior. According to Glanz, perceived barriers are anything that hinders individuals from making certain behavioral changes (29). In HBM theory, it is explained that everything that hinders this can be seen in terms of high costs, benefits, unsatisfactory and enjoyable health services and support from family and others (22).
Respondents who have high perceived barriers is because most of the respondents are housewives and family's income of most is low. The higher a person's income, the higher the level of life, especially in terms of fulfilling pregnancy nutrition (30,31). Hupunau's research shows that the most common difficulties or obstacles experienced by a person in providing healthy food are high food prices (cost), remote access to purchases (distance), and limited available products (22). The level of income can affect a person's healthcare because someone with a high income can carry out health maintenance activities (32).
Cues to action refer to external factors that influence a person to adopt certain health behaviors. In this context, cues to action refer to the factors that encourage pregnant women to carry out behavior to fulfill nutritional needs. The results of this study indicate that there is a significant relationship between the behavior of fulfilling the nutritional needs of pregnant women and cues to action based on the health belief model. Strong cues to action, such as effective educational messages, positive social support, or influence from medical personnel or nutritionists, can encourage pregnant women to be more active in meeting their nutritional needs during pregnancy (33). According to the health belief model, when pregnant women feel exposed to strong cues to action, they tend to have a higher perception of the severity of health risks associated with inadequate nutrition during pregnancy, they feel more vulnerable to these risks, they believe that nutritional fulfillment can help reduce these risks, and they feel they have high benefits from nutritional fulfillment. This can encourage pregnant women to adopt more optimal nutritional needs.
From the data, it can be seen that respondents who have high cues to action will have good nutrition fulfillment behavior. Fulfillment of nutrition for pregnant women is influenced by several factors, namely support from husband, family, and community. Without the support of the closest people, a goal will not be achieved properly, such as material support to meet the nutritional needs of pregnant women. Economic limitations will also affect the adequacy of the nutritional status of pregnant women (34).
The results of the study show that cues to action are significantly related to the behavior of fulfilling nutritional needs. This is due to family factors and health workers who influence it. Family involvement during pregnancy really supports the health of babies and pregnant women (35). Families are expected to always provide support to pregnant women to improve nutrition fulfillment behavior such as inviting and involving the family to participate in antenatal care visits and classes for pregnant women. In addition to family support, the support of health workers is also influential because the majority of pregnant women are always present to attend classes for pregnant women held by the local village midwife. Health workers are health service providers who have a very large role in supporting mothers' ability to recognize, understand, and change the behavior of pregnant women to optimize nutrition during pregnancy (36).
STRENGTHS AND LIMITATIONS
The study utilizes the health belief model (HBM) as the guiding framework, which provides a comprehensive understanding of the factors influencing the nutritional fulfillment behavior of pregnant women. This strengthens the theoretical basis of the study. Conducting the study in Jombang, Indonesia, allows for insights into the specific cultural, social, and environmental factors that may affect the nutritional behaviors of pregnant women in that region. This localized approach enhances the study's relevance and applicability to the target population. The study included a diverse sample of pregnant women from different socioeconomic backgrounds, educational levels, and demographic characteristics. This diversity enhances the generalizability of the findings to the broader population of pregnant women in Jombang. Limitations of the study are the study's sample was recruited from specific healthcare facilities or communities, which may limit the generalizability of the findings to the entire population of pregnant women in the region. The results should be interpreted with caution when extrapolating to other contexts. The study relied on self-reported data, such as questionnaires or interviews, to assess nutritional fulfillment behavior and factors influencing it. The limitation of this study is that it does not examine confounding factors, so it does not know the causal factors. Therefore, further research can analyze confounding factors.
IMPLICATION FOR PRACTICE
This research provides strong evidence about the importance of perceived benefits, perceived barriers, and cues to action in influencing the behavior of meeting the nutritional needs of pregnant women. The implication of this research is the importance of an approach that focuses on increasing perceived benefits, overcoming perceived obstacles in an effort to increase the fulfillment of the nutritional needs of pregnant women and the importance of strengthening cues to action factors. In this context, interventions that target increasing knowledge and awareness about the benefits of meeting nutritional needs, increasing the accessibility of nutritious food, providing social support, or providing clear and easy-to-understand information about nutrition during pregnancy can help reduce perceived barriers and involve medical personnel or a nutritionist in providing guidance or advice can be an effective strategy to improve the behavior of fulfilling the nutritional needs of pregnant women. This study, focusing on factors influencing pregnant women's nutritional needs, directly contributes to several Sustainable Development Goals by highlighting the importance of family involvement, public health support, and the development of interventions based on the Health Belief Model to improve maternal health and nutrition, promoting gender equality and fostering partnerships for achieving these goals. The study's findings suggest several actions for the government to improve maternal health and nutrition. Investing in nutritionist training and resources at public health centers, promoting family involvement in supporting pregnant women, addressing barriers to accessing nutritious food and healthcare, and developing targeted interventions based on the Health Belief Model are crucial. Public awareness campaigns emphasizing the importance of good nutrition during pregnancy and the role of healthcare providers and families are also essential. By implementing these recommendations, the government can create a more supportive environment for pregnant women, leading to improved maternal and child health outcomes.
CONCLUSIONS
Factors related to the behavior of fulfilling nutritional needs are perceived benefits, perceived barriers, and cues to action. Family involvement is needed in providing support for pregnant women and increasing the role of the public health center, especially nutritionists at every antenatal care visit. Future research is expected to develop a health belief model factor for intervention to improve behavior in fulfilling nutritional needs in pregnant women.

