










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Type 2 diabetes mellitus (T2DM) has become a chronic disease with a global epidemic and poses a significant challenge to public health (1). The dramatic rise in prevalence is the result of multiple factors, including unhealthy lifestyle habits, obesity, sedentary behavior, and genetic predisposition. As the global population ages and lifestyles change, the prevalence of T2DM is expected to continue to grow. According to a study published in the Lancet in 2023 (2), the number of people with diabetes worldwide is likely to surge to 1.31 billion by 2050, of which T2DM patients will make up the vast majority, more than 96 %.
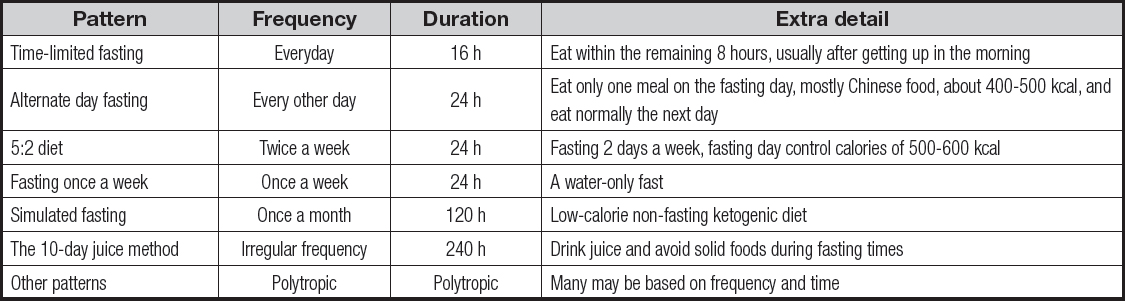
Fasting, or the restriction or avoidance of food intake for a specified period of time, can extend from 12 hours to three weeks (3). Numerous studies have shown that fasting can extend the lifespan of a variety of experimental organisms. In addition, a series of prospective clinical trials have also indicated that fasting can help reduce disease risk factors associated with aging, including cardiovascular disease, diabetes, and certain types of cancer. Fasting also increases the body's resistance to oxidative stress, such as during acute surgical stress. There are also studies showing that fasting may improve the effectiveness of some cancer treatments. A variety of dietary interventions have been tried to address a range of metabolic dysfunction, of which intermittent fasting (IF) stands out because of its popularity. Table I (4-6) details the different IF patterns and their respective characteristics.
Recently, researchers from the University of Utah, the University of Wisconsin-Madison and other institutions published a study (7) in the Journal of the American Medical Association. The study pooled meta-analyses of 11 published randomized clinical trials that assessed 104 unique associations between four types of IF (including alternate-day fasting, modified alternate-day fasting, 5:2 diet, time-restricted eating) and obesity-related health outcomes. In particular, high-quality evidence supports that 1-2 months of modified IF is associated with a modest reduction in body mass index in healthy adults and in people with overweight, obesity, or non-alcoholic fatty liver disease. The paper suggests that IF may play a positive role in improving weight and cardiometabolic outcomes, particularly in adults who are overweight or obese. As a dietary management strategy, IF has attracted a lot of attention in patients with T2DM. Numerous studies have shown that IF may confer a range of metabolic health benefits. Despite this, there is currently a lack of systematic reviews or meta-analyses incorporating randomized controlled trials (RCTS) to fully evaluate the safety and efficacy of IF in T2DM treatment. Given the controversial effects of IF on the improvement of blood glucose, blood lipids, HbA1c and body weight in T2DM patients, and with the continuous development of this dietary pattern in global T2DM studies, meta-analysis is particularly necessary. The gaps in the literature in this area highlight the need for rigorous research on IF as an adjunct therapy for T2DM. Therefore, the purpose of this study was to systematically evaluate the safety and effectiveness of IF in the treatment of T2DM, and to provide evidence-based medical evidence for dietary intervention programs for T2DM patients (8).
DATA AND METHODS
INCLUSION AND EXCLUSION CRITERIA
Inclusion criteria
1) Study design: RCT in Chinese/English; 2) Subjects: diagnosed with T2DM, ≥ 18 years old, no other complications; 3) Intervention measures: the intervention group implemented IF; 4) Outcome measures: the main measures were blood glucose results (HbA1c, fasting plasma glucose (FPG), postprandial plasma glucose (PPG)), cholesterol, and triglycerides. Secondary outcome measures were anthropometric measures (including body weight, BMI, waist circumference), systolic blood pressure (SBP), diastolic blood pressure (DBP), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C).
LITERATURE SEARCH STRATEGY
Two researchers (HX and HG) independently searched the databases of PubMed, The Cochrane Library, Web of Science, MEDLINE and CNKI from their setup to September 2024, using a combination of subject words and free words. The terms were as follows: diabetes mellitus, type 2 diabetes mellitus, T2DM; intermittent fasting, IF, intermittent energy restriction, intermittent caloric restriction, time restricted feeding; randomized controlled trial, RCT.
LITERATURE SCREENING AND DATA EXTRACTION
Two researchers (HX and HG) independently screened the literature and extracted data according to established inclusion and exclusion criteria. In the event of disagreement, the differences are resolved through discussion or, if necessary, the intervention of a third researcher to make a final judgment. In the literature selection process, the EndNote literature management software was first used to eliminate duplicates, and then a preliminary screening was conducted by reading the title and abstract of the article to eliminate the literature that did not meet the inclusion criteria. For literature that is considered likely to be eligible after initial screening, the researchers will further read the full text to make a final decision. Excel 2019 software was used to extract literature data, and the extracted information included key data such as first author, publication year, study location, sample size, intervention methods and outcome indicators.
LITERATURE QUALITY EVALUATION
Two investigators (HX and HG) will independently evaluate literature quality according to Cochrane Randomized Controlled trial literature quality evaluation criteria. In case of disagreement during the evaluation process, a third researcher or domain expert will decide. The specific evaluation criteria are as follows: If the study fully meets the evaluation criteria, it indicates that the possibility of various biases is low, and the quality of the literature is rated as grade A. If the part of the study meets the evaluation criteria, it indicates that the possibility of bias is moderate, and the literature quality grade is B. If the study does not meet the evaluation criteria at all, it indicates that the possibility of bias is high, and the quality of the literature is set at grade C (9).
STATISTICAL METHODS
In this study, the RevMan 5.3 software was used for meta-analysis. First, heterogeneity among included studies was assessed by chi-square tests and I2 statistics. If the I2 value is less than or equal to 50 %, heterogeneity between studies is low, and the fixed effect model is selected for the meta-analysis. If the value of I² is greater than 50 %, it indicates that there is significant heterogeneity among the studies, and then a random effects model is used for analysis. For the data of continuous variables, when the measurement units used in different studies were the same, we used the weighted mean difference (WMD) and its 95 % confidence interval (CI) to represent the results. When the units of measurement did not agree, the results are presented using the standardized mean difference (SMD) and its 95 % CI.
RESULTS
BASIC CHARACTERISTICS OF THE INCLUDED LITERATURE
A total of 148 papers meeting the requirements were preliminarily retrieved, and 16 were finally included through layer by layer screening. The basic characteristics of the included references are shown in table II (10-25).
Table II. Basic features of the included articles
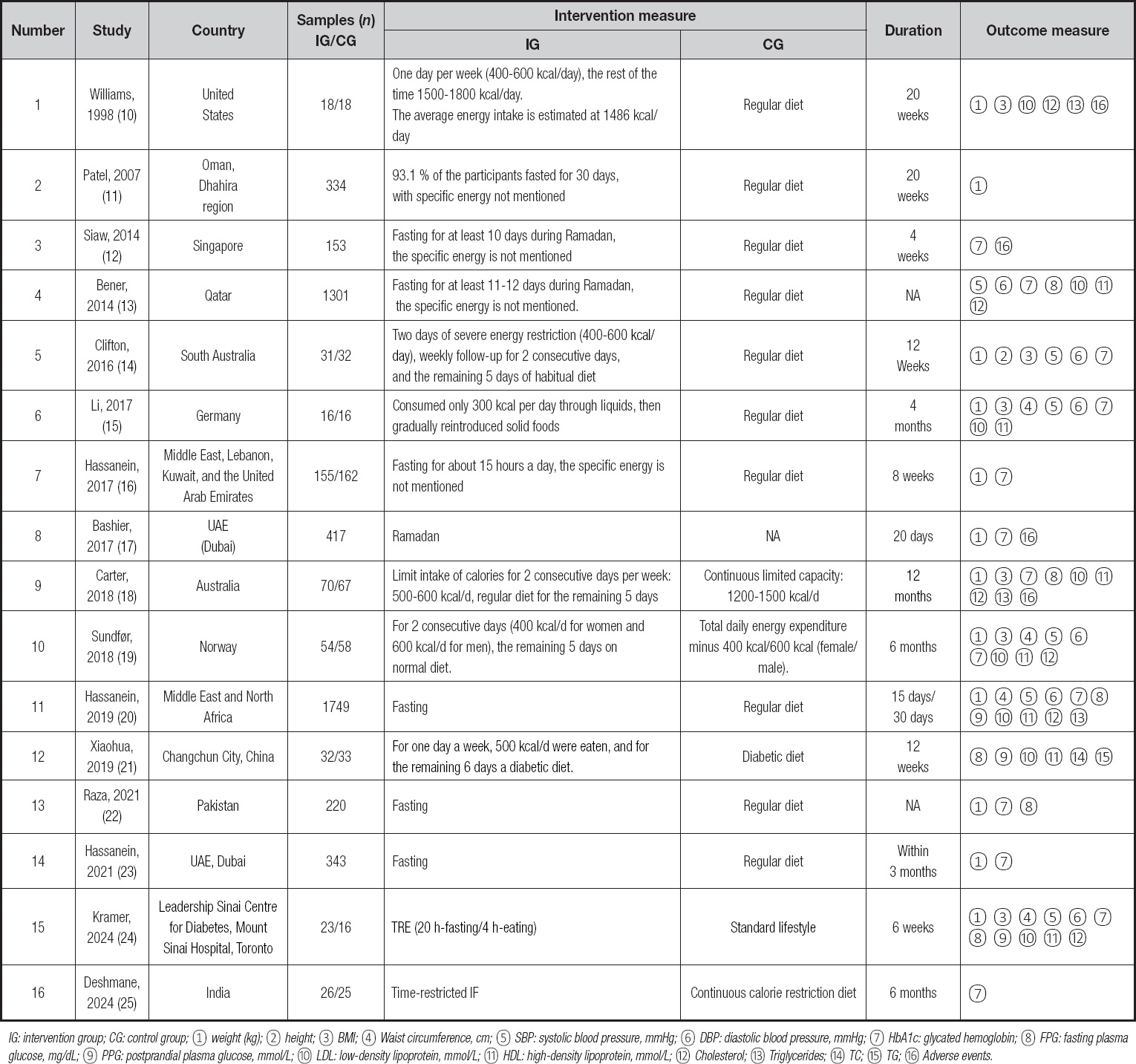
IG: intervention group; CG: control group; ① weight (kg); ② height; ③ BMI; ④ Waist circumference, cm; ⑤ SBP: systolic blood pressure, mmHg; ⑥ DBP: diastolic blood pressure, mmHg; ⑦ HbA1c: glycated hemoglobin; ⑧ FPG: fasting plasma glucose, mg/dL; ⑨ PPG: postprandial plasma glucose, mmol/L; ⑩ LDL: low-density lipoprotein, mmol/L; ⑪ HDL: high-density lipoprotein, mmol/L; ⑫ Cholesterol; ⑬ Triglycerides; ⑭ TC; ⑮ TG; ⑯ Adverse events.
RESULTS OF THE META-ANALYSIS
On a global scale, modern humans are facing a number of complex chronic health challenges, including obesity, diabetes, metabolic diseases, and cardiovascular disease. Over the past decade, large-scale clinical trials have demonstrated that IF can reduce body weight and body fat, improve insulin sensitivity, lower blood sugar and insulin levels, reduce blood pressure, improve lipid levels, and reduce biomarkers of inflammation and oxidative stress. This meta-analysis included 16 randomized controlled trials involving a total of 5369 patients.
Blood glucose results (Fig. 1)
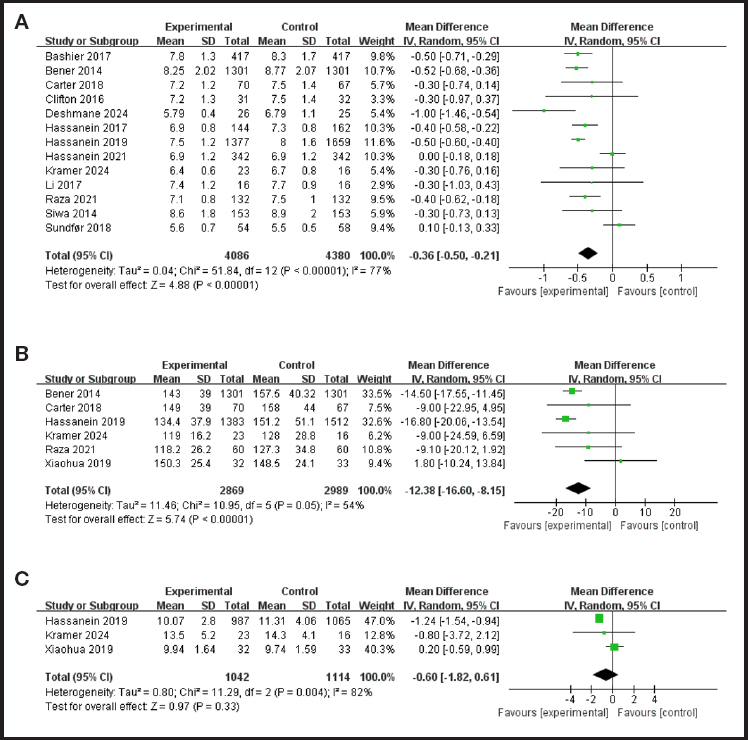
Figure 1. Meta-analysis of blood glucose status and IF in T2DM patients: A. HbA1c. B. Fasting plasma glucose. C. Postprandial plasma glucose.
Thirteen studies evaluated the effect of IF on controlling HbA1c in T2DM patients. Heterogeneity testing showed that there was heterogeneity among the studies (p < 0.0001, I2 = 77 %). Random effects model analysis showed that, IF significantly improved HbA1c levels (WMD = -0.36, 95 % CI = -0.50, -0.21, p < 0.0001).
Six studies evaluated the effect of IF on fasting plasma glucose in T2DM patients. There was heterogeneity among studies (p = 0.05, I2 = 54 %). The random effects model analysis showed that IF could significantly improve FPG levels (WMD = -12.38, 95 % CI = -16.6, -8.15, p < 0.0001).
Three studies evaluated the effect of IF on postprandial plasma glucose control in patients with T2DM. There was heterogeneity among the studies (p = 0.0004, I2 = 82 %). Random effects model analysis showed that there was no statistically significant difference in postprandial plasma glucose reduction between the IF group and the control group (WMD = -0.60, 95 % CI = -1.82, 0.61, p = 0.33).
Anthropometry and other general information (Fig. 2)
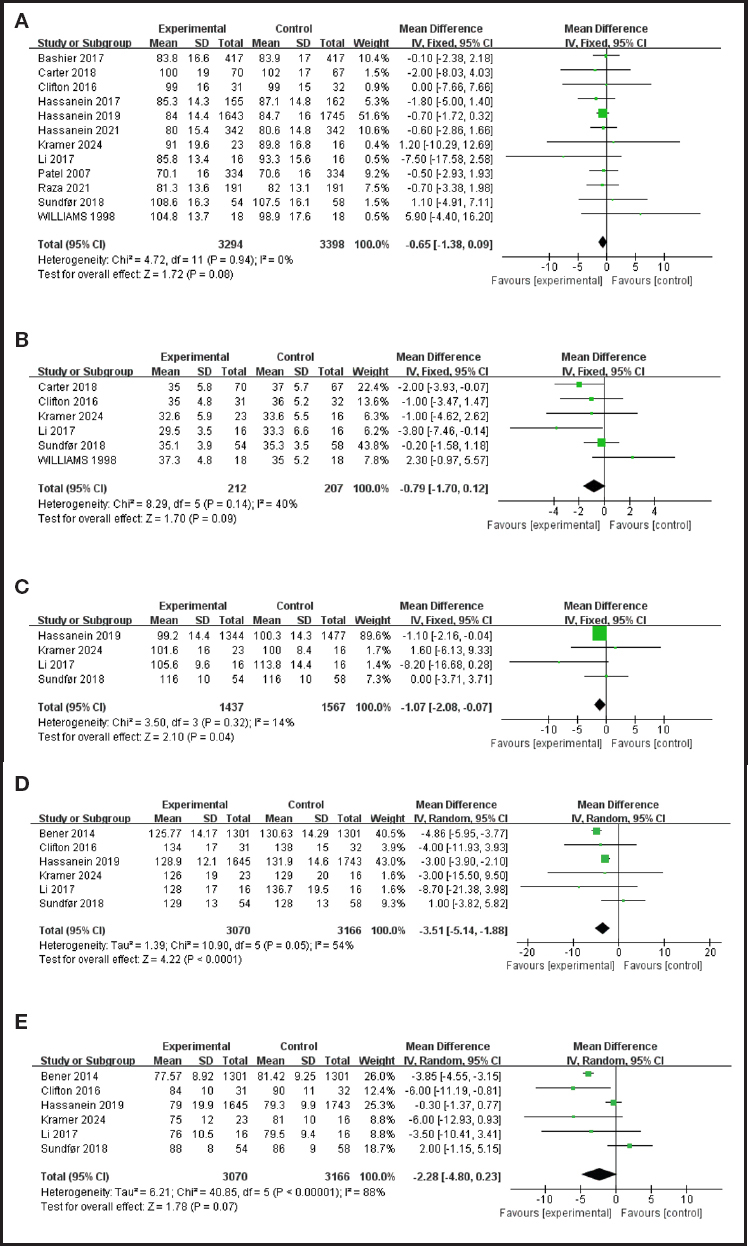
Figure 2. Meta-analysis of anthropometry and other general information and IF in T2DM patients: A. Weight; B. BMI; C. Waist circumference (continues on next page).
Twelve studies evaluated the effect of IF intervention on body mass in T2DM patients. There was heterogeneity among the studies (p = 0.94, I2= 0 %). The fixed-effect model analysis showed that IF could improve body mass (WMD = -0.65, 95 % CI = -1.38, 0.09, p = 0.08).
Six studies evaluated the effect of IF intervention on BMI in T2DM patients. There was heterogeneity among studies (p = 0.14, I2 = 40 %). Fixed-effect model analysis showed that IF could improve BMI level (WMD = -0.79, 95 % CI = -1.70, 0.12, p = 0.09).
Four studies evaluated the effect of IF on waist circumference in patients with T2DM. There was heterogeneity among studies (p = 0.32, I2 = 14 %). The fixed-effect model analysis showed that IF could improve waist circumference (WMD = -1.07, 95 % CI = -2.08, -0.07, p = 0.04).
Six studies evaluated the effect of IF intervention on blood pressure in T2DM patients. When it comes to the effect of IF on SBP in T2DM patients, there is heterogeneity among studies (p = 0.05, I2 = 54 %). Random effects model analysis shows that IF can significantly improve SBP (WMD = -3.51, 95 % CI = -3.82, 5.82, p < 0.0001).
Six studies evaluated the effect of IF on DBP in T2DM patients, and there was heterogeneity among the studies (p < 0.0001, I2 = 88 %). Random effects model analysis was used, and the results showed that IF could significantly improve DBP (WMD = -2.28, 95 % CI = -4.80, 0.23, p = 0.07).
This meta-analysis showed that IF significantly reduced SBP and DBP. The reduced blood pressure may be attributed to significant weight loss. It is well known that there is a strong association between weight and blood pressure in obese patients. IF is expected to improve the lifestyle of patients with pre-diabetes and T2DM. Future RCTS with higher quality and longer follow-up are needed to confirm the findings (26).
Lipid profile (Fig. 3)
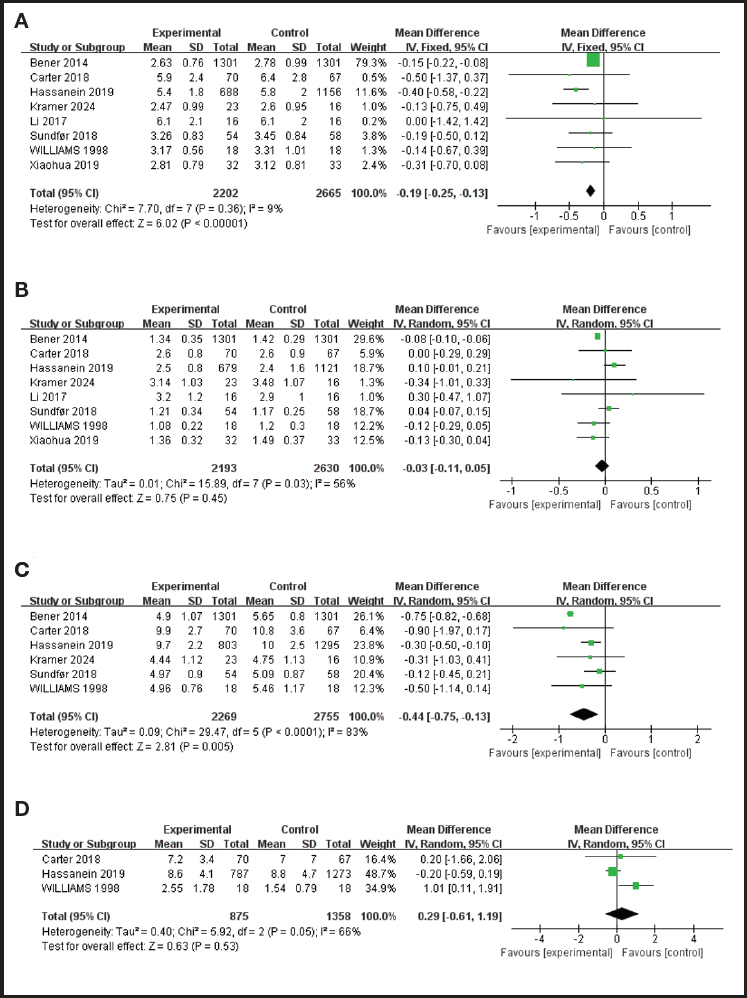
Figure 3. Meta-analysis of lipid profile and IF in T2DM patients: A. LDL. B. HDL. C. Cholesterol. D. Triglycerides.
Eight studies evaluated the effect of IF on LDL in T2DM patients, and there was heterogeneity among the studies (P=0.036, I2=9%). Fixed-effect model analysis showed that IF could significantly improve LDL (WMD = -0.19, 95 % CI = -0.25, -0.13, p < 0.0001).
Eight studies evaluated the effect of IF on HDL in T2DM patients, and there was heterogeneity among the studies (p = 0.03, I2 = 56 %). Random effects model analysis was used, and the results showed that there was no statistically significant difference in HDL reduction between the IF group and the control group (WMD = -0.03, 95 % CI = -0.11, 0.05, p = 0.45).
Six studies evaluated the effect of IF on cholesterol in T2DM patients, and there was heterogeneity among the studies (p < 0.0001, I2 = 83 %). Random effects model analysis showed that IF could significantly improve cholesterol (WMD = -0.44, 95 % CI = -0.75, -0.13, p = 0.0005).
Three studies evaluated the effect of IF on triglycerides in T2DM patients, and there was heterogeneity among the studies (p = 0.05, I2 = 66 %). Random effects model analysis was adopted, and the results showed that there was no statistically significant difference in the reduction value of triglycerides in the IF group compared with the control group (WMD = 0.29, 95 % CI = -0.61, 1.19, p = 0.53).
Security and compliance
Adverse events during the study were reported in four articles. Of these, no serious adverse events occurred in 3 studies. One study reported a 78/417 incidence of hypoglycemic events, but these adverse effects improved after the intervention. Wliiiams and other studies included in this study showed that the compliance of the subjects was 86.11 % at 5 months; Carter et al. showed that the compliance of the subjects was 72.86 at 12 months. Thus, IF is safe and feasible.
DISCUSSION
IF IS BENEFICIAL FOR BLOOD GLUCOSE CONTROL IN T2DM PATIENTS
Multiple studies have shown that IF can significantly improve blood glucose control in patients with T2DM. Specifically, IF is able to reduce FPG and HbA1c levels. In addition, IF also helps to improve insulin sensitivity and reduce insulin resistance, which is an important benefit for people with T2DM, as insulin resistance is one of the core features of the disease. IF is also able to help people with T2DM lose weight, which has a positive impact on improving blood sugar control and promoting overall health.
IF IS BENEFICIAL FOR T2DM PATIENTS TO REDUCE BODY WEIGHT, BMI, WAIST CIRCUMFERENCE AND LDL-C LEVEL
In recent years, IF as a dietary pattern has received a lot of attention in terms of health promotion and disease management. The study by Professor Gong Tingting's team points out that for adults who are overweight or obese, IF may have a range of health benefits, including reduced waist circumference and body fat mass, improved lipid levels, and lower fasting insulin levels. In an RCt-based umbrella review that analyzed 351 unique associations, it was found that IF significantly reduced waist circumference, body fat mass, LDL, triglycerides, and blood pressure levels. In addition, some studies have observed that IF improves cardiovascular health indicators, such as lowering blood pressure and cholesterol levels, and these findings are consistent with our findings. In patients with T2DM, IF may help improve blood sugar control. It is important to note that the effects of IF may vary from individual to individual, so before trying IF, patients are advised to consult a professional physician or dietitian for personalized advice and guidance. In addition, future studies are needed to further evaluate the effects of IF on various health outcomes and explore its potential mechanisms of action (27).
IF IS SAFE AND FEASIBLE IN T2DM PATIENTS
Common IF patterns include the 5:2 pattern (restricting caloric intake for two days a week and eating normally for the remaining five days) and time-restricted eating (eating only during certain periods of time each day) (28). Different IF patterns may have different effects on blood sugar control. Overall, as a diet management strategy, IF has shown potential to improve blood sugar control and overall health in patients with T2DM. However, because there may be differences between individuals, it is recommended that patients try IF under the guidance of a healthcare professional.
COMPARISON WITH OTHER STUDIES
Different from previous studies, which mainly focused on the effects of IF on body weight and blood glucose level, this meta-analysis specifically focused on the effects of IF on blood pressure. To our knowledge, this is the first meta-analysis of this relationship. In this meta-analysis of ten studies, we found that IF significantly reduced systolic blood pressure and similarly significantly reduced diastolic blood pressure in patients who had reached 12 weeks of intervention. These findings are significant because they offer a new perspective on lowering blood pressure. While there is plenty of evidence in basic and clinical research to support the multiple health benefits of IF, there is still room for further research in the following areas. First, this study found that the effects of IF on heart rate and lipid levels were not significant, which is a difference from the results of basic studies, suggesting that more convincing clinical study data is needed to clarify this. Second, future studies need to consider how to generalize the conclusions of this study to groups of patients at high risk of prediabetes and T2DM to more fully assess the potential of IF in blood pressure management (29).
LIMITATIONS AND PROSPECTS
The literature review showed that IF was able to reduce body weight by 3-5 kg over 12 weeks, an effect comparable to sustained energy restriction. However, it is not clear what the best dietary strategy should be during fasting. Common IF patterns include the 16:8 pattern (fasting for 16 hours a day) and the 5:2 pattern (restricting calorie intake two days a week). The interaction between IF and lifestyle factors such as skipping breakfast and using medications may have an impact on physical and mental health, especially in the adolescent population. Although short-term IF has shown some benefit in animal models and human studies, its role in non-obese individuals and its impact on risk factors for type 2 diabetes in adolescents needs further study. It is important to note that low-carb diets may increase risk factors for type 2 diabetes in adolescents compared to low-fat, high-carb diets promoted by adult guidelines. Overall, although IF has shown some advantages in weight management and health, more rigorous research is urgently needed to identify best practice approaches and assess their potential risks (30).
Although the IF model has received a lot of attention as an emerging weight loss method, there are still many key questions that need to be answered. Currently, there is insufficient information on the safety, acceptability and effectiveness of IF strategies in the wider population. In addition, most of the existing study samples are mainly from Western populations, which limits the general applicability of the findings. Although multiple studies have explored IF, there is no consensus on the ideal dietary pattern for fasting days. Previous studies have mainly described caloric restriction on fasting days, such as recommending consuming 75 % of recommended calories on fasting days (31), but have lacked clear guidance on dietary patterns on non-fasting days. In addition, it is unclear whether a high-protein diet is recommended during fasting. Some previous studies have pointed out that a high-protein diet may help enhance sustained satiety, thereby reducing the hunger associated with prolonged fasting. What's more, whether the recent popularity of meal replacement products can provide additional health benefits for IF is also a question that deserves further research. In conclusion, in order to fully assess the potential benefits and risks of IF, future research needs to explore the long-term effects and best practices of IF in different population and cultural contexts.
Previous research (32) has shown that long-term light or moderate fasting, such as IF, can have a positive effect on health and may extend life. In addition, proteomic analysis of white blood cells revealed that short-term intensive fasting not only increased neutrophil degranulation, but also promoted cytokine secretion. This suggests that short-term intensive fasting can enhance immune function, especially innate immune function, at least in part by altering the expression profile of white blood cells. As a popular dietary intervention, IF is considered relatively easy to adhere to and has been associated with multiple health benefits, including promoting weight loss and improving blood sugar levels. Although the specific mechanism behind the beneficial effects of IF is not fully understood, it may be related to the regulation of the gut microbiome.
There are several limitations to this study that need to be taken into account when interpreting the results. First, there was a degree of heterogeneity between the included trials and the dietary regimen, and the length of the intervention may have been the main cause of this heterogeneity. To address this issue, a random effects model was used for data consolidation and sensitivity analysis was performed for possible sources of heterogeneity. Secondly, the number of RCTS that met the inclusion criteria was limited, and the sample size was generally small, especially for T2DM patients. In addition, this study focused on alternative outcome measures (such as HBA1c, FPG, etc.) with intervention spans ranging from 8 weeks to 12 months, which limits our ability to draw definitive conclusions about the effects of IF on blood glucose control. Although there may have been some selection bias in the current study, as the relevant studies were not registered in a public database, we still strictly followed the steps of the systematic review, following a pre-set flow chart. Longer-term clinical trials are needed in the future to evaluate the long-term effects and safety of intermittent fasting in different populations. Delve into how intermittent fasting can promote health by altering the gut microbiome or other biological pathways. Explore the differences in individual responses to intermittent fasting and how to tailor a personalized eating plan based on an individual's genetic background, lifestyle, and health status. Research on optimal eating patterns during non-fasting periods and how to combine high-protein diets or meal replacement products to enhance the health benefits of intermittent fasting. Expand the study to include populations in diverse cultural and geographic contexts to assess the universal applicability and cultural adaptation of intermittent fasting (33).
CONCLUSION
So far, there have been few experimental studies using IF in people with type 2 diabetes, because not all people with diabetes are suitable for IF diet therapy. In addition to improving blood sugar and promoting weight loss, the IF diet may also help improve other risk factors for T2DM, including insulin resistance and high blood sugar levels. Although further research is needed to validate these findings, the IF diet strategy provides clinicians with a range of intervention options to recommend to younger patients at risk for T2DM. Future studies should further explore the long-term impact of IF on risk factors for type 2 diabetes in adolescents and assess its applicability in different populations and cultural contexts to develop a better dietary pattern for T2DM patients to manage and control blood sugar, lipids, and body weight, leading to a better quality of life for people with diabetes (34).

