










 Servicios personalizados
Servicios personalizados
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
After the appearance of Sars-Cov-2 (COVID-19) at the end of the year 2019, the World Health Organization (WHO) declared a public health emergency due to the high number of infections and deaths in January of 2020 (Chen et al., 2020). The high rate of infection of the disease and low response capacity triggered the collapse of health systems in several countries and a health crisis not experienced in decades (Pallarés et al., 2020). Currently, thanks to the development of vaccines and immunization programs, the virus transmission chain have been majorly contained (Casas & Mena, 2021). In this context, countries in Europe and North America have relaxed their containment policies, especially the most restrictive ones (Hatef et al., 2021), and there is a gradual return to normality. However, the situation in South America is different, where three countries in particular (Brazil, Argentina, and Colombia) have high rates of infections and deaths, as well as a limited percentage of vaccination in their population (WHO, 2021). In addition, the variants of the virus (especially Delta and Omicron) have raised the alarms again and control measures are being taken again (Lazarevic et al., 2021).
In the case of Ecuador, in March of 2020 a health emergency was declared (Ministerio de Salud Pública (MSP), 2020). Some measures taken by the government were the suspension of all non-essential services, the restriction of mobility, and forced isolation. This, however, did not allow full control of the situation and triggered a social and economic crisis that impacted the quality of life (Sarasty et al., 2020). Currently, through the "Vaccination Plan 9/100", the rates of cases and deaths have gradually decreased (MSP, 2021). However, the fight against the disease is not over. Access to the vaccine, the predisposition to be vaccinated and the emerging variants continue to be a challenge to overcome. Currently, the impact of the health crisis in Ecuador is still under investigation, especially around the effects on mental health the general population had, has, and will have in the future (Caycho-Rodríguez et al., 2021; Moreta-Herrera et al., 2021a).
COVID-19 and mental health
Mental health is a key component for quality of life (Goldberg, 1978) since it not only implies the absence of disease but a full state of well-being (WHO, 2001), however, it is usually fragile in the face of significant variations at the typical context of development (Ferreira et al., 2021; Moreta-Herrera et al., 2018). Previous minor experiences in other pandemics (Ebola, SARS, H1N1, others) suggest the presence of stressful situations and psychopathology produced by quarantines, confinements, isolation, survival of the disease, among others (Brooks et al., 2020).
According to available evidence, current pandemic conditions and control measures have an impact on mental health (Ferreira et al., 2021; García-Espinosa et al., 2021; Gloster et al., 2020). The lack of social coexistence, the experience of the disease, and even the death of family and friends affect mental balance and can even aggravate pre-existing conditions (Menzies & Menzies, 2020). For example, people who suffered from COVID-19 presented adjustment problems, fear, uncertainty, and symptoms of anxiety, depression, and post-traumatic stress (Guo et al., 2020; Luchetti et al., 2020); while those who saw relatives and friends die generated feelings of helplessness, anxiety, and fear (Ahorsu et al., 2020).
In the same way, data indicate that the most affected groups are young people between 18 and 25 years old and adults between 26 and 60 years old (Ozamiz-Etxebarria et al., 2020), they present symptoms of anxiety, depression, post-traumatic stress, anguish, insomnia (Salari et al., 2020); increase in suicide attempts and alcohol and drug use (Brooks et al., 2020; Goyal et al., 2020; Chiappini et al., 2020), and high levels of stress and depression with clinical symptoms with a prevalence of 11% and 25% respectively (Gloster et al., 2020). However, this varies from country to country depending on the conditions of the pandemic and their health policies. In Paraguay, for example, 21.3% presented moderate anxious-depressive symptoms and 15.9% severe anxiety and depression (Ferreira et al., 2021). In Colombia, levels of depression were found with a prevalence of 47.08% and anxiety with a prevalence of 27.06%. (García-Espinosa et al., 2021). In Ecuador, there is evidence of the prevalence of anxiety (19.4%), depression (10.3%), and stress (13.5%) in the adult population (Tusev et al., 2020; Zumba-Tello & Moreta-Herrera, 2022). Hence, it is important to explore this phenomenon to have a better approximation of future effects.
Fear, anxiety, and stress as risk factors
Preventive measures taken by countries to contain COVID-19 have an impact on the normal development of human life. Social distancing, one of the main policies, produces changes in daily routines and has harmful effects (Ribot et al., 2020), for example, in some adults, there is evidence of stress, domestic violence, and child abusive behavior (Galea et al., 2020; Su et al., 2021). In addition, other measures such as information regarding the pandemic increase fear of contagion, anxiety, and daily stress, which may explain the increase in psychological affectation. Fear is an emotion that acts as a warning sign and increases when a threat, such as COVID-19, is perceived (Nikopoulou et al., 2020; Moreta-Herrera et al., 2021a). if the emotion continues, it constitutes a risk factor (Kokou-Kpolou et al., 2020; Reznik et al., 2020). Evidence shows how COVID-19 is related to symptoms of anxiety, depression, and stress (Liu, 2020; Qiu et al., 2020).
Another factor is anxiety about COVID-19. The experience of living within the pandemic contributes to the appearance of specific anxiety conditions about the disease (Peteet, 2020; Monterrosa-Castro et al., 2020) and affects symptomatic manifestations (Caycho-Rodríguez et al., 2021; Lee, 2020). There is evidence of positive correlations between anxiety to COVID-19 and psychological distress (Landi et al., 2020). In particular, it is related to somatization disorders, generalized anxiety, depression, insomnia (Chaturvedi, 2020; Lee, 2020; Menzies & Menzies, 2020), and others.
Stress is the third factor. The lack of stress coping strategies produced by social isolation and poor adaptation to the changes derived from the pandemic is well known (Franco & Leví, 2020), these deteriorate mental health and produce an increase in psychological symptoms (Wu et al. al., 2020). This usually happens due to the extensive and long periods of stressful situations that people experience in events such as natural disasters or wars (Fan et al., 2015). The current pandemic is not an exception and causes a decrease in people's ability to resist, thus, several psychological effects derived from stress are revealed, such as sleep problems (insomnia, early awakening, waking up during the night, nightmares), anxiety, and obsessive-compulsive symptoms (Rojas & Mazón, 2021), somatization disorders (Shangguan, 2021), in addition to worry and suicidal ideation (Killgore et al., 2020) for example.
Therefore, according to the existing academic literature, both fear and anxiety about COVID-19, as well as stress affect mental health. However, several aspects are not fully clarified, especially the variability of symptoms among people who have suffered the disease. Likewise, and due to the relatively short time of the pandemic, little is known about the predictability of these variables in mental health or the existence of explanatory models that allow a deeper understanding of the effect of the context of the COVID-19 pandemic. Finally, although there is research in Ecuador on the subject, it is still limited in the field of psychology and is not focused on hospital patients. For these reasons, research is required to clarify the current state of the art, as well as to respond to the gaps in knowledge aforementioned and the generation of proper solutions.
Objectives and hypotheses
The objectives of this study are a) To estimate the prevalence of fear and anxiety about COVID-19, perceived stress and psychological discomfort in a sample of hospital patients in Ecuador; b) To determine the relationship between fear and anxiety of COVID-19 and perceived stress in Mental Health; c) To develop a predictive model of mental health based on fear and anxiety of COVID-19 and perceived stress, using SEM.
Method
Design
This study applied a descriptive, comparative, and explanatory design (Ato et al., 2013) assessing fear and anxiety of COVID-19, stress, and the perception of mental health in hospital patients of Ecuador.
Participants
The sample corresponds to 460 participants, 38.9% are men and 61.1% women, between 18 and 79 years old (M = 36 years old; SD = 14.48), 84.6% reside in the urban area and 15.4% in rural areas, 51.7% have permanent work, 15.7% temporary work and 32.6% are unemployed. Regarding educational levels, 74.6% have higher education, 21.7% have secondary education and 3.7% have primary education. Concerning marital status, 41.1% of the sample is single, 37.4% married, 9.1% in unmarried cohabitation, 8% divorced, and only 1.3% widowed.
The participants are primary care outpatients belonging to the psychology area, who are referred from the internal medicine area (no patient was referred from the psychiatry area), who attended various hospital centers in the cities of Ambato and Quito. 60.4% attended to hospital centers of the Instituto Ecuatoriano del Seguro Social (IESS), 36.3% attended to public hospitals of the Ministerio de Salud Pública del Ecuador (MSP), and 3.3% attended private hospital centers. Regarding the variables associated with COVID-19, 30.1% reported that they had the disease or suspected that they had it, while 69.6% indicated that they had not had it or do not believe they have been infected yet. In addition, 73% had relatives infected with COVID-19 and 82% had close friends infected with the disease.
The selection of the participants was carried out through a non-probabilistic sampling with the following inclusion criteria: a) being older than 18 years; b) attending one of the hospital centers of the study; c) voluntary participation, and d) having an email account or be registered on the social network Facebook or Whatsapp to carry out a digital evaluation.
Instruments
The Fear of COVID-19 Scale (FCV-19S; Ahorsu et al., 2020) in the Spanish version and adapted to the Ecuadorian population (Moreta-Herrera et al., 2021a). It assesses the perception of fear of COVID-19 contagion, through 7 items on a five-option Likert scale (1 = Strongly disagree and 5 = Strongly agree). It has a bifactorial structure with two specific factors, Emotional response (items 1, 2, 4, 5) and Physiological reaction (items 3, 6, and 7)), and a general factor. Norm-referenced scores for the scale are not presented but scores greater than 21 can be considered as a risk. Regarding the psychometric properties, the scale has an adequate internal consistency between items in the Ecuadorian population ω = .89 (.88 - .90), while for the present study it is α = .86.
Coronavirus Anxiety Scale (CAS; Lee, 2020) translated and adapted to Spanish (González-Rivera et al., 2020; Moreta-Herrera et al., 2022). The scale assesses symptoms of anxious thoughts related to the exposure of information about COVID-19. The instrument is a Likert-type scale made up of 5 items (0 = none and 4 = almost every day). High scores reflect the existence of greater anxiety symptoms towards COVID-19 (scores greater than 10 are considered risky). Regarding reliability, the original version found a Cronbach's alpha of α= .93 (González-Rivera et al., 2020), while in this study an internal consistency of α = .87 was obtained.
Perceived Stress Scale (PSS-14; Cohen et al., 1983) translated into Spanish (Remor, 2006), and adapted to an Ecuadorian context (Larzabal-Fernandez & Ramos-Noboa, 2019). The scale assesses perceived stress in everyday situations. The instrument is made up of 14 items with 2 dimensions: perception of stress (items 1, 2, 3, 8, 11, 14) and coping with stress (items 4, 5, 6, 7, 9, 10, 13 (reverse items)), with a five-option Likert scale from 0 (never) to 4 (very often). High global scores (between 39 and 56 points) determine the presence of severe stress (cut-off point corresponds to 28 points). The scale presents a Cronbach's alpha of α = .61 in the Ecuadorian population, while in the present investigation the test obtained a Cronbach's alpha of α = .83.
General Health Questionnaire (GHQ-28; Goldberg, 1978). In its 28 items version, it measures psychological alterations within a primary care context. The Ecuadorian adaptation presents a bifactorial structure with 4 specific factors: a) somatization, b) anxiety-insomnia, c) social dysfunction, and d) depression, plus a general factor (Moreta-Herrera et al., 2021c). It is a four-option Likert scale with several scoring methods, one of them is the binary method, which assigns 0 points for the answer options “Not at all” and “No more than usual”; and one point for the answer options “Rather more than usual” and “Much more than usual”, cut-off points for this method are > 3 for the factors and > 14 for the global scale. In a study with an Ecuadorian sample, the test obtained an internal consistency of α = .92 for somatization, α = .96 for anxiety-insomnia, α = .95 for social dysfunction, and α = .98 for severe depression (Moreta-Herrera et al., 2021b). In this study, the internal consistency for the somatization factor is α= .81, α = .88 for anxiety-insomnia, α = .82 for social dysfunction, α = .88 for severe depression, and α = .93 for the global scale.
Procedure
We selected the assessment tools to measure COVID-19 fear and anxiety, stress, and health perception. For the administration of the tests, we developed a self-administered digital template distributed through email and social networks (Facebook and WhatsApp). Previously, we carried out a pilot test with 30 participants to determine the application time and the effectiveness of the template. To collect the information, the tests were applied during the interview with the mental health professional in charge of the project, while they were attended (those who did not have their cell phones were sent the tests by email so that they could answer it at home). This study was carried out from April to June, at which time the country was in confinement due to accelerated contagion and affectation of priority attention groups that produced the new variants of COVID-19, there was vehicular and human mobility restriction. Meetings were held with a maximum capacity of five people and the hospital care centers attended regularly in all their services by 30%. All educational institutions, both colleges, and universities were in virtual classes. As for funeral rites, they were allowed, but only relatives of the deceased could attend.
Before the application of the tests, the participants signed informed consent (6 participants refused to collaborate in the study), in addition, we provided information about the objectives, nature, and purpose of the study, they were also informed about the right to stop in any stage of the investigation and the confidentiality of their answers was guaranteed. They also received information on the care they should take to strengthen mental health and the use of prevention measures for mental health problems associated with external stressors (including COVID-19). The evaluation was carried out in an approximate time of 15 minutes. Once the survey was completed, all the information was refined and digitized to analyze it statistically and test the hypothesis. This research adhered to the ethical care criteria for human research based on the Helsinki convention.
Data Analysis
Data analysis was performed in four blocks. The first is a descriptive analysis, which includes the arithmetic mean (M), standard deviation (SD), skewness (g1), and kurtosis (g2). The percentage of risk cases that exceed the cut-off points of the tests is also added. The second block is a comparative analysis of the levels of fear and anxiety to COVID-19, the perception of stress, and general health. We compared the subjects who had COVID-19 versus those who did not, as well as participants who had family members infected versus those who did not. To achieve this analysis, we used the student's t-test (t) for independent samples to know if there are significant differences (p < .05). As a complementary analysis, we calculated the adjusted Hedges test (g) to obtain the effect size.
The third block includes an analysis of correlations between the variables of fear and anxiety of COVID-19, perceived stress, and general health. This process was carried out through the Pearson correlation coefficient (r) to know the strength of association between the variables under analysis. Finally, the fourth block is an analysis using SEM to analyze a predictive model of mental health based on fear and anxiety of COVID-19 and perceived stress. The analysis is performed using confirmatory factor analysis (CFA) and Diagonally Weighted Least Squares (DWLS) estimator, which is the most appropriate estimator for categorical variables (five or fewer options) (Li, 2016). The statistical analysis was carried out through the R programming language in version 3.6.1 (R Core Team, 2019) using foreign, lavaan, and psych packages.
Results
Descriptive Analysis
Table 1 shows that Fear of COVID-19 presents moderate levels with a prevalence of 40.2% for risk cases. Regarding anxiety, the levels presented are low and with a prevalence of 10.4% for risk cases. As for perceived stress, the presence of this phenomenon is moderate and there is a prevalence of risk cases of 22.8%.
Regarding mental health, symptoms of anxiety-insomnia and somatization are the ones with the greatest prevalence, while symptoms of social dysfunction and depression have the lowest incidence. Broadly speaking, general mental distress is low. Regarding the prevalence of risk cases, those of anxiety/insomnia present the highest incidence (21.1%) and depression the lowest incidence (6.1%). Regarding general health, 10.2% of the participants can be considered as risk cases.

Comparative Analysis
Table 2 shows that there are differences in the variable Fear of COVID-19, the participants that never had the disease feel greater fear when compared to people who have already gone through the disease (p < .05) with a small effect size (g > 0.2). Likewise, regarding the perception of health in general, people who already had COVID-19 report more symptoms of somatization when compared to people who were never infected (p < .05), the effect size is still low.
Regarding the perception of stress, the anxiety of COVID-19, and other factors of the GHQ-28, no statistically significant differences were found between the groups analyzed (p < .05), however, those who already suffered from the disease show a slight increase in mental health symptoms when compared to the uninfected.
Table 2: Comparative analysis between people who were infected versus people who were not infected with COVID-19.
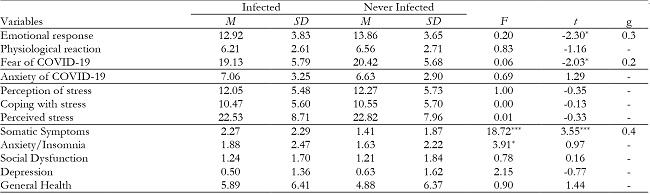
Note:*p < .05;
**p < .01;
***p < .001;
M: Mean; SD: Standard Deviation; F: Levene test; t: t-test; g: Hedges' g
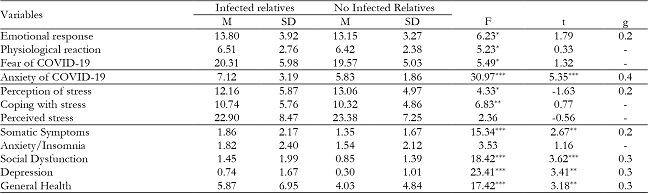
On the other hand, Table 3 shows that levels of anxiety of COVID-19 are significantly higher in participants with relatives who had been infected with COVID-19 than in those without infected relatives (p < .05). Likewise, regarding the perception of general health, greater symptoms were found among participants with relatives who had already suffered from COVID-19 than in those without infected relatives (p < .05), except for symptoms of anxiety and insomnia. In all cases with statistically significant differences, the effect sizes are small (g > 0.2). Both for fear of COVID-19 and stress, there were no significant differences between the groups.
Correlation analysis
Table 4 shows the results of the correlation analysis, where the perception of stress and anxiety to COVID-19 have a moderate and positive relationship with the perception of general health. Also, Fear of COVID-19 has a low and positive relationship with discomfort in the perception of general health. Fear and anxiety of COVID-19 have a moderate and positive relationship with somatic symptoms and anxiety/insomnia, while perceived stress has a moderate relationship with somatic symptoms, anxiety/insomnia, social dysfunction, and depression. Finally, Fear of COVID-19 and Anxiety of COVID-19 have a positive and moderate relationship, but a low and positive relationship with perceived stress.
Table 4: Analysis of correlations between Fear and Anxiety of COVID-19, Perceived Stress and General Health.

Note:**p < .05;
FCV-19S: Fear of COVID-19; CAS: Anxiety of COVID-19; PSS-14: Perceived stress; F1: Somatic Symptoms; F2: Anxiety/Insomnia; F3: Social Dysfunction; F4: Depression; GHQ-28: General Health
Multiple linear regression analysis
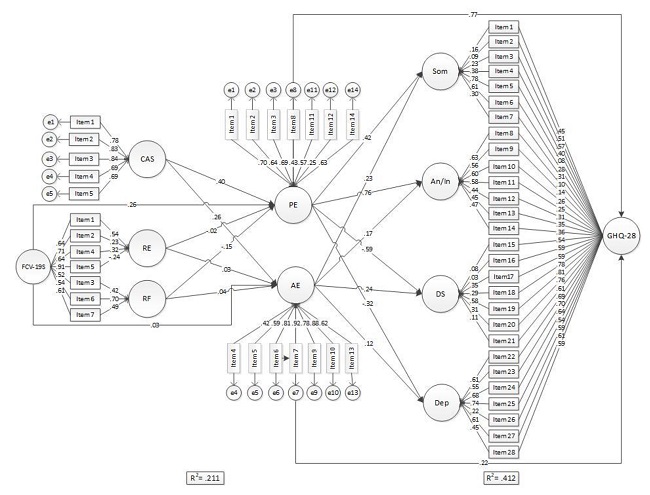
Figure 1 shows a predictive model using SEM where fear and anxiety of COVID-19 are predictors of perceived stress (first regression) and, in turn, perceived stress is a predictor of symptoms of psychological distress (second regression). The means of the independent variables achieve an explained variance of 21.14% in the first regression and 41.2% in the second regression. Likewise, CFA analysis shows this predictive model has a good fit and adequate factor loadings between the items, which indicates that the model fits the sample adequately.
Discussion
The objectives of the study were to identify the prevalence of Fear and Anxiety of COVID-19, perceived stress and psychological distress in a sample of hospital patients in Ecuador; the relationship between these variables, and the development of a predictive model of Fear and Anxiety of COVID-19 in perceived stress, and this, as a predictor of mental health.
Regarding the psychological affectation due to the pandemic (Table 1), the participants present moderate levels of Fear of COVID-19 and low levels of Anxiety of COVID-19. These results are consistent with previous similar studies inside and outside of Ecuador (Caycho-Rodríguez et al., 2021; Moreta-Herrera et al., 2021a). There are also moderate levels of stress since situations associated with pandemics, lockdowns, and quarantines have an impact on mental health; this converges with Brooks et al. (2020); and also, with studies about the current pandemic (Ferreira et al., 2021; García-Espinosa et al., 2021). This is due to prolonged exposure to stressful agents derived from the situation (Fan et al., 2015). In addition, other psychological symptoms are presented, in which somatic symptoms and anxiety/insomnia prevail. These findings are consistent with similar preliminary reports from the current pandemic (García-Espinosa et al., 2021; Gloster et al., 2020; Salari et al., 2020;) including Ecuador (Tusev et al., 2020; Zumba- Tello & Moreta-Herrera, 2022).
There are statistically significant differences (p< .05) between groups (table 2), the non-infected participants present more fear (especially emotional response) than those who have been infected; while those who were infected presented greater somatic symptoms. Participants who have relatives who were infected or died of COVID-19 have more fear (emotional response), anxiety to COVID-19, somatic symptoms, social dysfunction, depression, and general mental health discomfort than those who do not have infected relatives (Table 3). This is consistent with previous findings by Ahorsu et al. (2020); who report that personal experience or from relatives around COVID-19 disrupts psychological stability. In addition, personal experience of contagion decreases the feeling of fear; however, post-contagion increases somatic and anxious symptoms. This aspect, in particular, is consistent with data reported by Luchetti et al. (2020); However, there are no previous data on the fact that the experience of having relatives infected with COVID-19 produces a worse psychological response (more fear, anxiety, and other symptoms) than the experience of personal contagion. This is an interesting finding because it seems that impotence, lack of control, and mastery of the situation further unbalance people's mental state.
Regarding the relationship between the analyzed variables (Table 4), Fear of COVID-19 is related to symptoms of anxiety-insomnia, somatization, social dysfunction, and general psychological discomfort. This is consistent with previous work that shows how Fear of COVID-19 increases mental disorders (Liu, 2020; Kokou-Kpolou et al., 2020; Qiu et al., 2020; Reznik et al., 2020). The same happens with Anxiety of COVID-19, which is especially related to somatic symptoms, anxiety-insomnia, social dysfunction, and depression to a greater degree than Fear of COVID-19. By experiencing a more intense condition, people could be more affected, as has been reported in similar studies (Peteet, 2020; Monterrosa-Castro et al., 2020; Caycho-Rodríguez et al., 2021). Finally, the impact of stress on mental health (consistent with previous reports (Rojas & Mazón, 2021; Shangguan, 2021; Killgore et al., 2020)) turned out to be much greater than the Fear and Anxiety of COVID-19. Likely, the combination of these previous elements with the usual stress load of participants contributes to a greater association of psychological alterations.
Given this mechanism, it was speculated that Fear and Anxiety of COVID-19 predict stress and the perception of stress predicts mental health. For this reason, a predictive model was developed using SEM (see Figure 1) to determine its fit. The fit indicators (CFI, TLI, RMSEA, others) were found to be adequate, and the model was found to explain changes in mental health variance by 41.2%, preceded by an explained variance of 21.1% in stress, which reveals the impact that these variables have on the phenomenon of interest. It should be noted that there are no preliminary studies to help confirm this finding, so these results should be taken with caution. However, they are a benchmark for the study of mental health in Ecuador and open space for analysis to learn about the role of psychological responses to COVID-19 and its implications for mental health.
This study is important at a theoretical level because it provides information on the psychological response to COVID-19, from two important aspects, the first one on the context of COVID-19 from a psychological perspective and the second one through stress and how it influences mental health. At a methodological level, the use of a sequential explanatory model through SEM stands out, which allows a more comprehensive interpretation of the phenomenon of mental health and COVID-19, which has not previously been studied. At a practical level, these results would allow the development of psychological intervention mechanisms in a future post-pandemic context. This may affect the development of specific intervention programs for direct and indirect victims of COVID-19 and even have supplies for future similar health emergencies; this could also help to include the mental health factor in health policies associated with the pandemic and that are not fully included in the country.
Limitations
Among the main limitations of the study, it should be mentioned that it was exclusively aimed at primary care patients in public and private hospitals, so these results should not be generalized in other population segments. We recommend carrying out similar studies in the future in the general population and in other types of patients such as children and adolescents, to have a more comprehensive view of the problem. Also at a methodological level, although there is an explanatory model that details the phenomenon of mental health concerning the context of COVID-19, these results do not explain causality between the variables, so future studies of structural relationships should consider longitudinal studies with at least three measurements or experimental designs. However, these results open the door to an important advance in the study of mental health and COVID-19.

