










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
The rapid spread of the coronavirus SARS-CoV-2 during the first quarter of 2020 forced countries around the world to take tough restrictive measures to contain the virus (Cohen & Kupferschmidt, 2020). In several countries, governments declared stay-at-home orders due to the public health emergency, limiting social activity and applying general home-confinement rules, usually excepting travel for essential jobs (Cohen & Kupferschmidt, 2020). The confinement and situation of stay-at-home orders have been associated with decreased mental health (Ausín et al., 2021; Brooks et al., 2020; Cuadrado et al., 2021; Cuadrado, Rich-Ruiz et al., 2023; González-Sanguino et al., 2021; Tull et al., 2020; Wang et al., 2020), with significant increases in stress and depression suffered by individuals. This decrease in mental health, in comparison to the pre-pandemic state, has been seen as a consequence of both social limitations and a decrease in the practice of healthy habits related to diet, physical exercise, and sleep during confinement (Ammar et al., 2021).
Far from returning the population to initial levels, different studies show that levels of stress and depression have remained high after the home-confinement periods ended, persisting several months after the end of confinement measures (Pieh et al., 2021; Pierce et al., 2021). The coronavirus crisis has been characterized by successive waves, restrictive measures to control cases, and negative information in the media that have undermined the mental health of the population. In this regard, Pierce et al. (2021) found that 23.1% of people significantly worsened their mental health during the pandemic. Of these people, almost half were unable to return to their pre-pandemic mental health status. In fact, 16.04% of the people that were affected in terms of mental health by the COVID-19 pandemic suffered an initial decrease in their mental health, with sustained elevated scores on poor mental health measures over time, while 31.0% of the affected individuals suffered a sustained decline in mental health over time.
Without underestimating the effects that confinement, restrictive measures, and distressing information about infection and death could have, an analysis of both the psychological protective and risk factors to mental health during the pandemic as well as the possible interaction between these potentially predictive factors, seems to be relevant, hence this study.
Perceived Risk, Perceived Efficacy, and Mental Health
COVID-19 has led to the death of 6,881,955 people worldwide to date (March 10, 2023) since it first appeared (Coronavirus Resource Center, 2023). Having lived for a long time with this disease may engender a high level of perceived risk-a subjective assessment that an individual performs on the level of risk associated with a specific situation (American Psychological Association, 2021)-in this case, the COVID-19 pandemic situation. The perception of increased risk could lead to worsening mental health in a pandemic situation (Bults et al., 2011). In the COVD-19 pandemic context, some investigations have obtained results that point in this direction. Risk perception and coronavirus fear have been associated with increased depression and stress among healthcare professionals (Yıldırım et al., 2020), as well as in the Chinese adult population (Li & Lyu, 2021). In this sense, we expected to find that people who perceive high risk related to COVID-19 would report higher levels of stress and depression, in comparison with individuals with lower COVID-19 perceived risk. Nevertheless, other researchers have found conflicting results. For example, Mækelæ et al. (2020) did not find that perceived risk of COVID-19 infection contributed to distress; they assumed that the distress of participants was probably related to concerns that were not specifically related to the health-related impacts of COVID-19, but were more to do with economic fear and worry about relatives.
An additional explanation of these discrepancies could be that other variables might act as moderators in the relationship established between perceived risk and distress, making the relationship appear or disappear according to the levels of those potential moderators. In this sense, one variable that could potentially attenuate the negative effect of the COVID-19 health crisis on mental health is the perceived efficacy of COVID-19 prevention measures. In this context, perceived efficacy refers to an individual’s confidence that COVID-19 preventive measures will be effective to minimize infection and spread of the virus. Previous studies have found that this variable has a significant impact on mental health (Dai et al., 2021; Mækelæ et al., 2020), as individuals who perceive that health-prevention measures are efficient are more protected from the mental health point of view. Moreover, it has been shown that access to preventive measures, and therefore a lower perceived risk of infection, is associated with fewer depressive symptoms (Lam et al., 2020). In this sense, previous studies have found that when individuals perceive that the actions taken by governments are effective, they also report higher levels of well-being (Helliwell & Huang, 2008). Interestingly, Dai et al. (2021) showed that the negative consequences that intolerance to uncertainty during the COVID-19 pandemic had on mental health (namely, on negative emotions) were moderated by the perceived efficacy of restrictions: The less individuals tolerated uncertainty related to the pandemic, the more negative affect they reported, particularly when perceiving low levels of efficacy of the restrictions. This result seems to give some evidence of the potential moderating role of perceived efficacy of COVID-19 prevention measures in the relationship between risk perception and mental health. Moreover, the moderating role of perceived efficacy has been demonstrated in several studies. In this sense, a meta-analysis confirmed that perceived efficacy acts as a moderator in the relationship established between risk appraisal and protective behavior: Risk appraisal impacts protective behaviors more strongly when perceived efficacy is enhanced (Sheeran et al., 2014). Another example is the Serpas and Ignacio (2022) study in which the authors corroborated the moderating role of perceived efficacy in the relationship established between fear of COVID-19 and preventive behaviors. Moreover, although the focus was not perceived efficacy but self-efficacy, a recent study has found a moderating effect of self-efficacy in the link between fear of COVID-19 and depression (Mumtaz et al., 2021). Overall, all this refereed literature seems to give a strong basis to the hypothesis about the potential moderating role of perceived efficacy in the relationship between risk perception and mental health. In this sense, in congruence with the previous literature, it can be expected that a negative impact risk perception related to COVID-19 on stress and depression could be moderated by the perceived efficacy of COVID-19 prevention measures.
Consistent with the reviewed literature, this study aimed to explore the perceived efficacy of COVID-19 prevention measures as a moderating variable between the relationships that perceived risk related to COVID-19 establishes with both stress and depression. We expected that the more people perceive that prevention measures are efficient at controlling the COVID-19 spread, the lower will be the negative impact of their perceived risk related to COVID-19 on their stress and depression levels. The study hypothesis is that the perceived efficacy of COVID-19 prevention measures moderates the relationships established between (a) COVID-19 perceived risk and stress, and (b) COVID-19 perceived risk and depression.
Method
Participants
Study questionnaires were completed by 478 participants (66.9% females; age range = (18, 89), M = 36.30, SD = 15.32). To target the general population in Spain, the study’s inclusion criteria required participants to be adults (over 18 years old), reside in Spain, have access to the Internet to complete the study survey, and be fluent in Spanish. In addition, participants had to consent to participate in the study and be available and willing to complete a questionnaire. Participants who did not meet the aforementioned inclusion criteria were declined participation in the study. Sociodemographic data can be seen in Supplementary Table 1.
Instruments
COVID-19 Perceived Risk
To measure to what extent participants perceived that COVID-19 imposed a risk on themselves and their families, the COVID-19 Worries and Fears Scale (CoV-WoFe; Cuadrado, Arenas et al., 2023) was used. Participants responded to the scale’s six items (e.g., “I am worried about catching COVID”) with a 7-point Likert scale, ranging from 1 (“strongly disagree”) to 7 (“totally agree”). The Cronbach’s alpha in the original study for the scale was 0.86. The reliability of the scale in the present study was high (α = .88).
Perceived Efficacy of the COVID-19 Prevention Measures
To assess to what extent individuals perceived that the measures against COVID-19 were efficient at protecting themselves from catching and spreading the virus, the Perceived Efficacy on COVID-19 Measure Scale, designed for the purposes of this study, was used. Individuals were asked to respond to what extent they perceived that the specified measures would be efficient in helping them avoid infection. Participants responded to the 14 items (e.g., “To what extent is it effective to avoid contagion using a mask when we cannot keep the safety distance of 2 feet?” on a 7-point Likert scale. The reliability was high (α = .95).
Stress
To measure to what extent participants suffered from stress, participants responded to four questions (e.g., “During the last 4 weeks, how often have you felt stressed?”) on the stress scale promoted by the Reference Center for Work Organization and Health-ISTAS, in its second version (CoPsoQ-ISTAS 21; Moncada et al., 2014). Participants responded to the four items with a 7-point Likert scale. Previous studies (Mendoza-Llanos & Moyano-Díaz, 2019) reported adequate reliability of the instrument (α = .76). The reliability of the scale in the present study was high (α = .90).
Depression
To measure to what extent participants felt depressed, the depression factor of the validated Spanish version of the Hospital Anxiety and Depression Scale (HADS; Herrero et al., 2003) was used. The HADS is a 7-item Likert scale that assesses the frequency of depressive symptoms, such as "I feel as if I am slowed down." The Spanish-validated version used in this study demonstrated high reliability (α = .90). The Cronbach's alpha coefficient in the present study was acceptable (α = .70).
Procedure
A retrospective cross-sectional and correlational design was employed. The sample was obtained through a combination of convenience and snowball sampling methods (Goodman, 1961), by sharing a link to an online questionnaire among university students at the University of Córdoba and on social media networks (mainly WhatsApp). Both participation and circulation of the questionnaire were solicited. Respondents completed the questionnaire between May 16, 2021 (in which 5,087 new COVID-19 cases and 78 new deaths were confirmed in the 7-day moving average in Spain; Coronavirus Resource Center, 2023), and June 6, 2021 (in which 4,189 new COVID-19 cases and 41 new deaths were confirmed in the 7-day moving average; Coronavirus Resource Center, 2023).
The study was conducted in accordance with the ethical principles for medical research involving human subjects of the World Medical Association of the Declaration of Helsinki and approved by the Ethics Committee of the University of Córdoba through code CEIH-22-4. Informed consent was obtained after participants were told about the study objectives and the voluntary and anonymous nature of their participation.
Data Analysis
To confirm the moderation hypotheses, moderation analyses were performed with the first model of the PROCESS for SPSS macro (Hayes, 2013), with a confidence interval of 95% and 10,000 bootstrap resamples. The variable perceived risk of infection was introduced in the model as the independent variable (IV), perceived efficacy of the prevention measures as the moderating variable (MV), and stress and depression as the dependent variables (DVs).
Results
Moderation Analyses
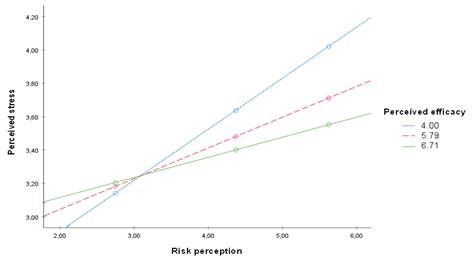
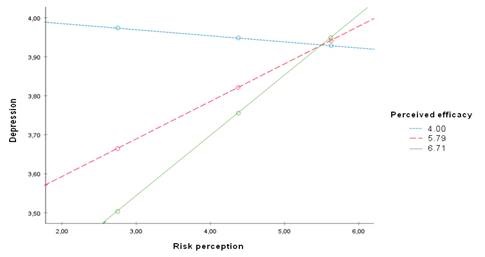
As expected, and as can be observed in Table 1 and Figure 1, perceived efficacy significantly moderated the relationship between (a) perceived risk and stress, R2 = .07; F(3, 474) = 11.92, p < .001, and (b) perceived risk and depression, R2 = .08; F(3, 474) = 13.99, p < .001. The moderated effects can be observed in Figure 1. Figure 1a represents the moderating role of perceived efficacy in the relationship established between perceived risk and stress. Figure 1b represents the moderating role of perceived efficacy in the relationship established between perceived risk and depression.
Figure 1. Observed Moderated Effects of Perceived Efficacy on the Risk Perception-Mental Health Relationship
Table 1. Results of the Moderation Analyses.

Note.X = independent variable; W = moderator; Y = dependent variable; RP = risk perception; PE = perceived efficacy; DV = dependent variable; UI = unconditional effect; SE = standard error; p() = p-value; LLCI = lower level for 95% confidence interval; ULCI = upper Level for 95% confidence interval.
Discussion
The outbreak of COVID-19 and the implementation of severe containment measures, especially home confinement, has had a strong impact on the daily lives of citizens. This study analyzed the mental health impact of the COVID-19 health crisis in Spain through the perceived efficacy of pandemic containment measures as a moderator of the relationships between COVID-19 perceived risk and stress, and COVID-19 perceived risk and depression.
The pandemic has had serious consequences related to mental health (Ausín et al., 2021; Brooks et al., 2020; Cuadrado et al., 2021; Cuadrado, Rich-Ruiz et al., 2023; González-Sanguino et al., 2021; Meng et al., 2023; Sicouri et al., 2023; Tull et al., 2020; Wang et al., 2020). The question is, can the perceived efficacy of COVID-19 prevention measures act as a moderating variable of these effects, specifically in the face of stress and depression?
Results confirmed this hypothesis, cohering with previous studies showing that the mental health of individuals is worse with decreased efficacy perception of the prevention measures against COVID-19 (Dai et al., 2021; Mækelæ et al., 2020) and increased risk perception (Bults et al., 2011), the latter having been demonstrated also in the pandemic context (Li & Lyu, 2021; Yıldırım et al., 2020; Yıldırım & Güler, 2021). Higher risk perception levels were related to higher levels of stress, but they were not related to depression. Indeed, a previous study (Mækelæ et al., 2020) found no relation between perceived risk and distress and proposed that this might indicate that an individual’s distress could be related to concerns not strictly related to the health-related impacts of COVID-19, as for example economic fears. However, the moderation analyses performed in the present study showed that the relationship between perceived risk related to the health-related impacts of COVID-19 and depression was not linear but depended in part on perceived efficacy levels. Although other studies have found that perceived efficacy often works as a moderating variable, no previous study explored its moderating role in the relationship between perceived risk and mental health outcomes. Therefore, the present study presents novel findings relevant from both theoretical and practical points of view.
In this sense, as we expected, the perceived efficacy of COVID-19 prevention measures moderated the relationships that perceived risk establishes with stress and depression. The observed effects demonstrate that the perceived efficacy of measures dampened feelings of stress and depression during the pandemic. These results align with previous studies,’ showing that the perceived efficacy of measures can act as a moderator on the relationship between intolerance of uncertainty and negative affect (Dai et al., 2021; Meng et al., 2023).
Regarding stress, the results demonstrate that the more individuals perceive risks related to COVID-19, the more they feel stressed, with additional stress associated with low levels of perceived self-efficacy. However, with high levels of self-efficacy, the perceived risk does not influence stress as much: The stress levels of people with a high level of perceived efficacy regarding health-prevention measures increase to a lesser extent as the risk perception levels go up. Therefore, individuals who perceive that prevention measures are efficient at avoiding COVID-19 infection and spread seem to be less affected by the stress caused by COVID-19 risk perception. Thus, perceived efficacy of prevention measures might be a powerful protective factor regarding stress in a pandemic situation, even for people who present with high-risk perception, a risk factor for stress.
Similarly, the results shows that the more individuals perceive risk related to COVID-19, the more they feel depressed, but only with moderate and low efficacy levels; results in this study showed a higher slope with moderate efficacy levels than with high efficacy levels. Moreover, when perceived risks were high, no differences appeared in depression levels between individuals with low, moderate, and high perceived efficacy. In contrast, when perceived risks were low or moderate, higher levels of perceived efficacy of the health-prevention measures acted as a protective factor for depression. In fact, when people perceived that the prevention measure were not effective at protecting them and preventing the spread of the virus (low perceived efficacy levels), their depression levels were high, independent of the perceived risk levels, with similar depression levels to those who reported low versus high risk. In general, it could be that with low and moderate perceived risk, the more individuals perceive that a pandemic’s prevention measures are effective, the less depressed they feel. Therefore, individuals who perceive that prevention measures are efficient at preventing COVID-19 infection and spread might be less affected by depression caused by low and moderate COVID-19 risk perception, as in this study. Also, this study’s results suggest that individuals who perceive that prevention measures are ineffective might still be strongly affected by depression, independent of the COVID-19 health-related risks they perceive. Overall, the perception that individuals have about the effectiveness of prevention measures appears to be a relevant protective factor for mental health during a pandemic.
A relevant implication of these findings is the special attention that governments and policy makers should put on positive risk communication and on reliable information about effective prevention strategies against COVID-19 infection and transmission. So-called fake news about the pandemic has been common, as has been incongruous information about the efficacy of prevention measures (Hrynick et al., 2020; Mouso, 2021; van der Linden et al., 2020). Nevertheless, both fake news and incongruous information about the efficiency of prevention measures can reduce the perception of the effectiveness of prevention measures (van der Linden et al., 2020), which, as we have seen in this study, will affect the mental health of people in a pandemic context. Thus, by considering the relevance for mental health of the perceived efficacy that people have for prevention measures against COVID-19 and on the health-related COVID-19 risks they perceive, healthcare professional, including psychologists, should pay special attention to those variables, and authorities and governments should design policies to improve them, with adequate and positive risk communication and coherent and congruous information about the effectiveness of prevention measures, as well as with implementation of effective measures against fake news.
Limitations and Future Research
Some of the limitations inherent to any scientific work should be noted. First, the snowball strategy of sample recruitment through social media networks may not have been sensitive to populations that either do not have access to social media or do not use it. On the other hand, it must be noted that the sample was random and not controlled. Perhaps the study could be replicated with a representative sample, according to an even distribution of participants per regional territories, age, sex, and other sociodemographic variables. It should also be noted that no sociodemographic variables, beyond the descriptive ones, were considered in the analyses presented here. Additional variables can be analyzed in future research. The scarcity of specific scientific literature has also been an obstacle in comparing our study with others on similar topics. In any case, the results should be considered with caution and investigators might continue to work along these lines.
In future research, it would also be relevant to discover which strategies for regulating stress and mitigating the symptoms of depression were addressed by the general population, on their own, in the face of the confinement situations during the peaks of COVID-19. In this line, it could be relevant to explore if different strategies to cope with stress might also play a moderating role, along with the perceived efficacy of COVID-19 prevention measures that acted as a moderating variable in this study. Moreover, as resilience seems to be a relevant variable that might result in lower individual levels of stress and depression, the moderating role of perceived efficacy of COVID-19 prevention measures in the relationships established between resilience and mental health could also be explored.
Conclusion
This study explored the moderating role of the perceived efficacy of health-prevention measures in the relationship between COVID-19 perceived risk and mental health, thereby minimizing the negative effect that perceived risk can have on stress and depression. The results showed that stress increased when the perceived risk was higher, and even more so with low perceived efficacy of prevention measures. Conversely, higher levels of perceived efficacy minimized the negative effect of moderate and high-risk perception on stress. In the case of depression, it also increased considerably when perceived risk increased, but with low and moderate perceived risk levels, a higher level of perceived efficacy minimized individual depression levels. Remarkably, at low levels of perceived efficacy, depression was always at a maximum level, independent of the perceived risk level.
In sum, this study highlights the potential relevance of high perceived efficacy of health-prevention measures as a protective factor against mental distress during a pandemic, when interacting with perceived risk. These findings lead us to understand and treat perceived efficacy as an opportunity to minimize stress and depression in times of home confinements related to pandemics. Governments, organizations, and institutions should consider this fact to reduce negative impacts on the mental health of local populations in situations with restrictive measures, such as those experienced during COVID-19. Misinformation should be avoided, and proper communication about the effectiveness of pandemic prevention measures seems to be particularly relevant.

