










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
The COVID-19 pandemic -a disease caused by the SARS-CoV-2 virus- has caused multiple repercussions worldwide, including millions of infections and deaths, prolonged confinement of the entire population, closure of educational, work and recreational environments, increased incidence of mental disorders (e.g. stress, anxiety, depression or insomnia) and substance abuse (Deng et al., 2021; Kola et al., 2021; Kumar & Nayar, 2021; World Health Organization, 2022).
The accelerated number of infections has led to an over-demand for health care services, which in turn has led to an increasing workload of health personnel. These professionals have been forced to perform their functions under strict sanitation and virus containment measures, which can be stressful and exhausting. These consequences are exacerbated when they experience fear of being infected or their loved ones, concern for their patients, and an increasing physical and psychological exhaustion (Chersich et al., 2020; Paiano et al., 2020; Walton et al., 2020). Working under the aforementioned conditions has produced symptoms of generalized anxiety and depression, especially in women, as well as, substance use in men; in both sexes, health personnel (HP) have reported the need for psychological care, due to burnout symptoms and the increased risk of developing acute stress disorder or post-traumatic stress disorder, compared to administrative staff (da Silva Neto et al., 2021; Raudenská et al., 2020; Robles et al., 2021).
During this health emergency, the relevance of HP mental health has been highlighted, since any psychological impairment may affect their professional activities (Lai et al., 2020), such as lower physical performance in patient care (Muller et al., 2020). In this regard, Quality of Work Life (QWL) is a psychological construct that refers to work performance and biopsychosocial well-being of different populations (Nowrouzi et al., 2016). Castro et al. (2018) define it as the individual's perception of his/her work, the satisfaction of his/her personal needs and expectations in the work and professional environment, through creative, healthy and safe work, guaranteeing personal, family and social fulfillment; as well as a means to preserve his/her health and economy. It has been proposed that this construct is made up of two dimensions, an objective one, referring to the worker's reality at work, this means, physical and social environment, and a subjective one, characterized by the satisfaction of well-being, productivity and positive self-experience (Michalos, 2014; Rodríguez-Marín, 2010).
The study of the QWL in HP has identified a positive association between the construct with organizational climate and job satisfaction (Pérez-Zapata et al., 2014; Pérez-Zapata & Zurita, 2014); as well as a negative association with burnout (Pérez-Zapata & Zurita, 2014; Saygili et al., 2020), number of hours worked (Alharbi et al., 2019), stress (Hipólito et al., 2017), exhaustion (Hall et al., 2016), intention to resign (Mosadeghrad, 2013) and work stress (Killian, 2005).
However, the operational definition of QWL in HP has been diverse and limited, since there are psychometric scales that do not consider the objective and subjective dimensions of the construct, and/or do not have acceptable psychometric indexes (Patlán, 2020). According to Windle et al. (2011) the assessment of psychometric quality involves reliability indexes (α = ≥ .80, ω = ≥ .70), validity (content, structure, construct, convergent and incremental), floor-ceiling effect (respondents in the lowest and highest scores: ≤ 15%) and the interpretation of scores (σ of significant groups); which are rarely calculated and/or reported by the authors. As an example of this, in the first scale to evaluate QWL in HP by Ferrans and Powers (1985; United States) the authors reported no structure evidence, convergent or incremental validity, nor floor-ceiling effects. The same applies to the scales of Martín et al. (2004; Spain), Herrera and Cassals (2005; Cuba), Vega & Martínez (2009; Chile), Calderón et al. (2008; Argentina), González et al. (2010; Mexico), Blanch et al. (2010; Spain), Toledo et al. (2010; Chile), Hernández-Vicente et al. (2017; Mexico) or Rivera-Ávila et al. (2017; Mexico).
Although there is a clear conceptual definition of the construct, its operational definition is characterized by heterogeneity and deficiencies in the psychometric quality of the scales used to measure QWL in HP. Therefore, developing a scale with an acceptable psychometric quality will allow to adequately evaluate the construct, in addition to identifying the areas in which HP perceive a low QWL, so psychological interventions and/or public policies can be implemented to improve the working conditions and mental health of this population, especially in situations of long-working hours, such as the pandemic of COVID-19. Therefore, the aim of this study was to develop and examine the psychometric properties of a psychological scale to measure quality of work life in Mexican health personnel.
Method
Design
Instrumental and cross-sectional study (Ato et al., 2013). In order to meet the stablished objectives, the study was conducted in two phases (development and validation).
Phase I. Scale development
The development of items was carried out by the main authors, who proposed items after participating in the following activities: 1) understanding of a conceptual definition of the construct (Castro et al., 2018) and its dimensions (Granados, 2011); 2), analysis of items of other scales that assess the same construct (Herrera & Cassals, 2005; Van Laar et al., 2007); 3) interview with experts (health personnel) and 4) focus groups (carried out with eight HP) (Escobar & Bonilla-Jiménez, 2017). Integrating the information from the four different sources, each author proposed the items of one dimension. Then, they were evaluated in terms of relevance, clarity and concordance by the rest of the authors. Based on these procedures, 63 items were developed and tested by different five experts in the field, in order to obtain content validity (Calleja, 2022). Aiken's V ≥ .90 was obtained, and 3 items were eliminated because they obtained a coefficient < .70. The response options were proposed on a 7-point Likert-type scale ranging from "Strongly disagree" to "Strongly agree" (Maeda, 2015).
Participants
To obtain psychometric validation and gather evidence of the questionnaire's structure and reliability, the principles of Classical Test Theory (Geisinger et al., 2013) were followed. The sample size was determined based on the classical principle of psychometrics, which recommends a minimum sample of 300 participants to minimize variance error (Boateng et al., 2018; Nunnally, 1978). The participants were HP recruited online, with a minimum schooling of a technical career and an employment contract in a public or private health institution. Two samples of participants were recruited, one for exploratory factor analysis (EFA) and the other for confirmatory factor analysis (CFA).
Instruments
Mexican Quality of Work Life Scale (MQWLS). Developed in Phase I. It measures the individual's perception of his/her work and the different contexts experienced by HP (Castro et al., 2018). It is composed by 60 items divided into seven dimensions (Relationship between Partners (RP), Resources and Technology (RT), Contract and Salary (CS), Work-Life Balance (WLB), Relationship with Manager (RM), Work Satisfaction (WS) and Professional Achievement and Work Relationships (PAWR)), whose definition is shown in supplementary material. It has a Likert scale of seven options going from strongly agree to strongly disagree.
Quality of work life scale (Martínez, 2019). Scale that evaluates the link between the employee and the institution, the needs of workers and the activities presented by the organization. It was adapted and validated in the study population obtaining a version made up of 17 items divided into 4 factors (personal development, autonomy, job security and equity), with a Likert scale of seven response options (Strongly disagree to Strongly agree). It showed excellent reliability (α = .937) and adequate fit indexes: CMIN/DF = 2.023; CFI = .976; SRMS = .050; RMSEA = .059.
Work-related Quality of Life Scale (Van Laar et al., 2007). It evaluates the quality of work life in health personnel. It was translated, adapted and validated in the study population, obtaining a 15 item-version divided into four factors (job satisfaction, job opportunities, working hours and professional achievements), with a Likert scale of seven response options (Strongly disagree to Strongly agree), reporting excellent reliability (α = .960), with the following fit indexes: CMIN/DF = 2.767; CFI = .948; SRMR = .052; RMSEA = .079 p < .001.
Work Stress Instrument (Hernández-González et al., 2012). It assesses environmental and work situations perceived as stressful. It was adapted and validated in the study population obtaining a 28 item-version divided into six factors (emotional exhaustion, dissatisfaction with remuneration, dissatisfaction with professional practice, lack of motivation, excessive work demands and professional demerit), with a Likert scale of four responses (from Never to Frequently); showing excellent reliability (α = .965), with the following fit indexes: CMIN/DF = 4.032; CFI = .846; SRMR = .052; RMSEA = .102 p < .001.
Brief Work Enthusiasm Scale (UWES-9, by its acronym in Spanish; Hernandez-Vargas et al., 2016). It evaluates the positive, persistent and work-related mental state. It was adapted and validated in the study population, obtaining a 7 item-version, one single factor and a Likert scale of five responses (from Never to Always). The scale yielded an excellent reliability (α = .938), with fit indexes: CMIN/DF = 1.925; CFI = .995; SRMR = .052; RMSEA = .056, p ≥ .05.
Procedure
The battery of instruments, which included MQWLS, Quality of work life scale, Work-related Quality of Life Scale, Work Stress Instrument and Brief Work Enthusiasm Scale, was answered online through Google Forms®. The participants first answered the sociodemographic data and if they accepted the informed consent, they answered each of the questionnaires. Answering questionnaires online has been shown to be as valid and reliable as paper-and-pencil instruments (Calleja et al., 2020; Pérez & Lugo-González, 2022). The link to the form was distributed via Facebook® and WhatsApp® through advertisements to target population in two periods (from February 09 to March 06, 2021 and from May 19 to June 09, 2021) To answer the battery lasted approximately 25 minutes.
Ethical considerations
The protocol research of this study was approved by the Ethic Committee of the Facultad de Estudios Superiores Iztacala, Universidad Nacional Autónoma de México (approval folio no. 1399). Participation in the study was anonymous, confidential and voluntary, and all participants agreed to participate after reading the informed consent form.
Data analysis
In the first sample, descriptive statistics of the participants and the distribution properties of the items were obtained in order to delete those participants who did not show variability and those items that were biased. The reliability of the items was then tested by eliminating those that correlated very poorly with the total scale (< .35; DeVellis, 2017; Furr, 2018). An Exploratory Factor Analysis (EFA) was performed with the Maximum Likelihood method and Oblimin rotation, expecting that the variance explained was greater than 40% and every item load more than 0.40 in each factor (Ferrando & Lorenzo-Seva, 2014; Lloret-Segura et al., 2014). Likewise, the mean variance explained (to evaluate convergent internal validity) and multivariate normality were obtained with Mardia test, and metric invariance models were also tested. Finally, to obtain external evidence of convergent validity, Pearson correlations were performed with the Quality of Work Life Scale (Martínez, 2019) and Work-related Quality of Life Scale (Van Laar et al., 2007), as well as with Work Stress Instrument (Hernández-González et al., 2012) and UWES-9 (Hernandez-Vargas et al., 2016); expecting correlations greater than 0.30. In addition, analysis of variance (ANOVA) was performed to obtain evidence of discriminant validity with contrasted groups.
With the second sample of participants, a Confirmatory Factor Analysis (CFA) was carried out yielding the following fit indexes: the χ2 /degree of freedom ratio (CMIN/DF; value < 3 indicates an adequate fit); comparative indexes CFI and NFI, variance ratio GFI and AGFI (values > .90 and CFI > .95 are interpreted as an adequate fit); error indexes SRMR and RMSEA (values < .05 in the first case, and < .08 in the second, indicate an adequate fit) (Hu & Bentler, 1999). In addition, the proposed changes of modification indexes were made in order to improve the model fit. Analyses were performed in SPSS® and AMOS® v.23.
Results
Description of samples
Both samples were obtained by non-probabilistic purposive sampling; 293 HP participated in the first sample, of which 81.9% were women, with an average age of 40.41 years (SD = 9.36, range 20-63), 41% had a bachelor's degree and 49.5% were single; the most frequent profession was nursing (42%) and 29.4% worked in second level hospitals. The average length of service in months was 143.2 (SD = 111.3), the average monthly income was $18,268 pesos (SD = $16,951.9), and 54.6% of the participants already had COVID-19 vaccine. With respect to the second sample, 300 HP were recruited, of whom 81.3% were women, with an average age of 38.37 years (SD = 9.09, range 19-62), 43.3% had a bachelor's degree and 49.0% were single; the most frequent profession was nursing (56.3%) and 32.0% worked in first-level hospitals. The average length of service was 77.7 (SD = 91.04), the average monthly income was $16,289.29 pesos (SD = $8,800.44) and 19% had at least one COVID-19 vaccine (Table 1).

Exploratory factor analysis
The Kaiser-Meyer-Olkin index (KMO) was .952, and Bartlett's test of sphericity was significant (p < .001), indicating that the sample was adequate for subsequent analyses. Ten items were eliminated after inter-item correlation analysis and analysis of each item with the total scale. EFA was performed with the maximum likelihood method and Oblimin rotation with the remaining 50 items and the resulting model showed seven factors; however, 11 items did not meet the factor loading ≥ .40, so they were deleted. Finally, the resulting model consisted of 39 items distributed in six factors, which explained 67.6% of the variance.
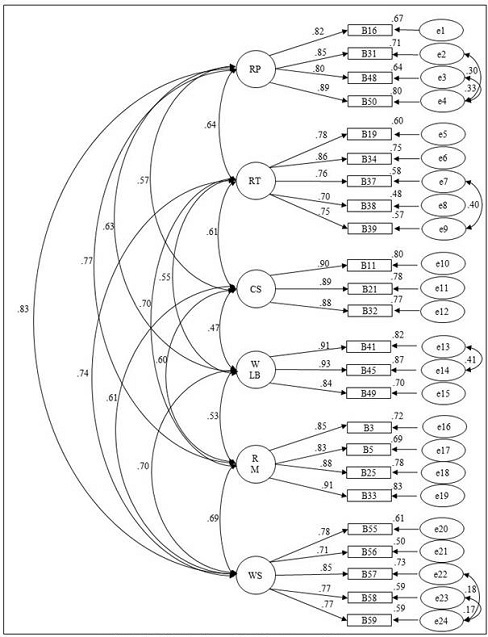
Confirmatory factor analysis
In CFA, items that had a large amount of error according to the residual covariances (n = 11), were deleted one by one: five were in factor 2 (item 1, 6, 12, 20 and 36), three in factor 4 (item 7, 29 and 30), two in factor 6 (item 22 and 54) and one in factor 1 (item 13). In addition, four items were eliminated for having high residual loadings (item 10, 27, 47 and 60).
The modification indexes suggested covariances between residuals; therefore, six covariances between errors were established that improved the model fit (Figure 1). The standardized factor coefficients obtained for the 24 items that made up the final version of the scale were satisfactory and the fit indexes were as follows χ2(231) = 564.729; CMIN/DF = 2.445; CFI = .945; NFI = .910; GFI = .865; AGFI = .824; SRMR = .0447; RMSEA = .070 (.062-.077) p < .001. Correlations between factors were moderated, ranging from .468 to .827, and factor loadings were statistically significant and range from moderate to high (standardized λ between .695 and .934, p < .001).
In addition to the CFA, invariance models were performed. In the evaluation of measurement invariance by sex, initially the configurational invariance model (M1) was tested and the obtained indexes (CFI = .927; RMSEA = .057; χ2/df = 1.978) indicated that the model fit was adequate. After that, the metric invariance model (M2) was tested, the indexes showed that the model fit well and when compared to M1, the ΔCFI was < .01, the ΔRMSEA < .015, and the Δχ2 was not significant (p > .05). When the scalar invariance model (M3) was tested, it showed a good fit and, compared to M2, the ΔCFI was < .01, the ΔRMSEA resulted < .015, and the Δχ2 was not significant (p > .05). Finally, the strict invariance model (M4) was tested and the indexes showed a good model fit. Compared to M3, the ΔCFI was < .01 and the ΔRMSEA resulted < .015 although the Δχ2 was significant (p < .05). With these data, it could be concluded that the structure of the MQWLS is similar for men and women.
In the evaluation of measurement invariance by occupation, initially the configural invariance model (M1) was tested and the indexes obtained (CFI = .924; RMSEA = .059; χ2/df = 2.026) indicated that the model fit was adequate. Afterwards, the metric invariance model (M2) was tested, the indexes showed that the model fit well and when compared with M1, the ΔCFI was < .01, the ΔRMSEA resulted < .015, and the Δχ2 was not significant (p > .05). When testing the scalar invariance model (M3), it showed a good fit and, compared to M2, the ΔCFI was < .01, the ΔRMSEA resulted < .015, and the Δχ2 was not significant (p > .05). Finally, the strict invariance model (M4) was tested and the indexes showed a good model fit compared to M3, the ΔCFI was < .01 and the ΔRMSEA resulted < .015, although the Δχ2 was significant (p < .05). Then, these results demonstrate the presence of configural, metric, scalar and strict invariance, so the factor structure of the MQWLS is equivalent for physicians and other professions.
Reliability
The internal consistency index for the total scale was α =.949, while McDonald's Omega coefficient was ω = .982. The indexes per subscale dimension with Cronbach's alpha coefficient ranged from .880 to .939, and for the Omega's from .880 to .926. Composite and ordinal reliability were also obtained; the values were similar (Table 2).

Convergent validity
To obtain evidence of convergent validity, correlations were made with the Work Enthusiasm Scale (r = .439, p < .01) and the Work Stress Scale (r = -.322, p < .01; see Table 3).
Construct validity
To establish evidence of construct validity, correlations were performed with the Work-related Quality of Life Scale (r = .714, p < .01) and the Quality of Work Life Scale (r =.584, p < .01); results are shown in Table 3.
Table 3. Convergent and construct validity (correlation of the MQWLS with the other scales of the study).

DE= emotional exhaustion, DR= dissatisfaction with remuneration, DPP= dissatisfaction with professional practice, LM= lack of motivation, EWD= excessive work demands, DP= professional demerit; JS= job satisfaction, JO= job opportunities, WH= working hours, PA= professional achievements, PD= personal development, A= autonomy, JS= job security, E= equity,
*p < .01.
Discriminant validity
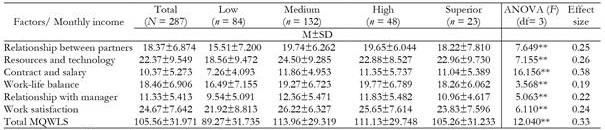
To obtain evidence of discriminant validity with contrasted groups, analyses were performed with some sociodemographic variables that the literature has suggested might be different in terms of QWL. Monthly income was the only variable showing statistical differences (p < .05) in the six factors of the scale, results are shown in Table 4.
Interpretation of the scale
The final MQWLS consisted of 24 items, distributed in 6 dimensions: 1. Relationships between partners (RC, 4 items), 2. Resources and technology (RT, 5 items), 3. Contract and salary (CS, 3 items), 4.Work-life balance (BV, 3 items), 5. Relationship with manager (RJ, 4 items) and 6. Work satisfaction (SL, 5 items); with seven response options on a Likert-type scale (from "Strongly disagree" to "Strongly agree"). The minimum score is 24, while the maximum is 168; the higher score obtained on the scale the better the QWL. The instructions for its application and the order of the items are presented in supplementary material
Discussion
In the last two years, HP have been one of the main risk groups for the development of mental disorders, substance use and deterioration in their quality of life as a result of their exhausting workday, which was exacerbated during the COVID-19 pandemic (da Silva Neto et al., 2021; Raudenská et al., 2020; Robles et al., 2021; Suryavanshi et al., 2020). Such a situation prompted the creation of a psychometric scale that would assess QWL in this population and have acceptable validity and reliability evidence.
The design of the MQWLS had a systematic and methodological rigor in both phases of the study, because it was based on a clear and integrative conceptual definition of the construct (Castro et al., 2018), allowing the operational definition of the different dimensions and, consequently, the generation of the items. The state of the art conducted during the first phase and considering the psychometric quality criteria proposed by Windle et al. (2011), allowed the identification of ten scales that assess WQL, however, they present limitations in their psychometric properties (e.g. do not consider both dimensions of the construct, do not report more than three validity evidences, reliability indexes are lower than .80, did not perform CFA or were designed only in one profession, among others); a situation that justify the need to create a scale with sufficient psychometric properties that adequately measure the construct (Calleja, 2022).
The evaluation of the items carried out by experts in the first phase showed evidence of content validity, subsequently, when performing EFA the theoretically proposed structure was corroborated, however, with the intention of having items with loadings ≥ 0.40, the scale was reduced to six factors (Ferrando & Lorenzo-Seva, 2014; Furr, 2018; Lloret-Segura et al., 2014). In the second phase, the results obtained in the CFA corroborated the validity of this structure constituted by six factors, which according to the indexes obtained and when contrasted with the indexes proposed by Hu and Bentler (1999), a valid model was obtained to evaluate QWL in HP. The factor loadings for the items ranged from moderate to high (.695─.934), indicated theoretical relevance for the construct measured (Furr, 2018). Regarding the internal consistency indexes (alpha and omega), the findings obtained for the total scale and by dimension suggest that the MQWLS is highly reliable (DeVellis, 2017; Windle et al., 2011).
Regarding the evidence of convergent validity, the MQWLS-24 correlated statistically and positively with the Work Enthusiasm Scale (Hernandez-Vargas et al., 2016), while negatively with the Work Stress Scale (Hernández-González et al., 2012). The above is consistent with literature, providing evidence on the correlation between QWL and these two constructs (Hipólito et al., 2017; Killian, 2005; Pérez-Zapata & Zurita, 2014), suggesting, on one side, the higher work enthusiasm the higher QWL, and on the other, the higher stress at work the lower QWL. Regarding construct validity, positive and significant correlations were found between the MQWLS-24 and the Work-related Quality of Life Scale (Van Laar et al., 2007) and the Quality of Work Life Scale (Martínez, 2019). Finally, evidence of discriminant validity was carried out with sociodemographic variables, with monthly income being the only significant one in the six dimensions of the scale. This finding allows us to identify monthly income as a variable that has an effect on QWL in HP, although there is great heterogeneity among the monthly income of the participants in the study, suggesting the higher monthly income, the higher QWL. As future considerations, it is proposed to carry out studies that consider this variable when measuring QWL and/or to develop a psychometric scale that evaluates satisfaction with economic remuneration, so the correlation between both constructs and social implications that this variable has on QWL can be analyzed in greater depth.
The psychometric indexes obtained in the MQWLS-24 are not only satisfactory and reliable, but also cover the psychometric limitations of existing scales to measure QWL in Mexico and the rest of the world (Blanch et al., 2010; Calderón et al., 2008; Ferrans & Powers, 1985; Gonzalez et al., 2010; Hernández-Vicente et al., 2017; Herrera & Cassals, 2005; Martín et al., 2004; Martínez, 2019; Rivera-Ávila et al., 2017; Toledo et al., 2010; Van Laar et al., 2007; Vega & Martínez, 2009), since it has a clear conceptual definition of the construct and its dimensions have multiple evidences of validity and reliability. Moreover, since it is a relatively short instrument, it is easy to answer and interpret. Future studies could consider the MQWLS-24 as the reference parameter for assessing QWL in HP in Mexico or validate and adapt it to other economically active groups.
Despite the strengths of the study, some limitations that were also present in the scale development should be considered. The scale was created during the COVID-19 pandemic, so participants' levels of QWL could differ from the work situation prior to this health emergency, given the conditions of work overload that could exacerbate the symptoms of emotional distress and generate a floor effect in the measurement of the construct. Therefore, a longitudinal study could be carried out to evaluate whether QWL variates as a function of the course of the pandemic and the work demands experienced by HP. Likewise, it would be optimal to carry out the application of the battery under a probabilistic sampling at national level, because although the scope was wider because of the electronic format, we did not obtained data from all the states. Finally, the sample was mostly made up of nurses and physicians, so it will be desirable to count with personnel of other areas.
Conclusion
MQWLS-24, the instrument developed in this study, is a promising psychological tool with a valid and reliable theoretical model to assess QWL in Mexican health professionals. QWL is a composite construct that, if affected, can have a negative impact on the performance of employees' daily work and their interaction with third parties. Health professionals are workers who interact daily with a large number of patients, family members and other professionals, so ensuring adequate or optimal QWL should be one of the priorities in labor policies in the public and private sector. In this regard, the MQWLS- can be used to rapidly identify in which of the six domains of QWL the health professional is affected, in order to implement psychological interventions and/or design labor policies to improve their work environment.
Declarations
Ethics approval.
The study was reviewed and approved by the Ethic Committee of the Facultad de Estudios Superiores Iztacala, Universidad Nacional Autónoma de México (approval folio no. 1399).

