










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Classified as a specific phobia in the DSM-5 (American Psychiatric Association, 2014), fear of flying causes intense anxiety and avoidance behaviours that can lead to severe anxiety disorders when flights cannot be avoided. Prevalence figures are imprecise and vary widely, ranging from 10% to 40% of the population in developed countries (Van & Diekstra, 2000). About 2.5% of the population have a specific phobia of flying (Oakes & Bor, 2010), while about 25% of the adult population experience significant anxiety when flying, 10% avoid flying because of their anxiety, and 20% resort to alcohol or sedatives to cope with flying (Botella et al., 2015; Rus-Calafell et al., 2013).
Fear of flying has several facets: fear of being in a closed space, of heights, lack of control over the situation, but primarily fear of having an accident (Tortella-Feliu et al., 2000). Cognitive-behavioral therapy or exposure therapy, both live and in imagination, has proven effective in treating this phobia. However, one of the techniques that has recently become popular for treating phobias is exposure therapy through virtual reality (VR) due to its numerous benefits (Baños et al., 2005; Glantz et al., 1996; Gottlieb et al., 2021; Hakim & Hammad, 2022; Renner et al. 2024; Smith et al., 2020; Tortella-Feliu et al., 2000), where considerable evidence has accumulated regarding its effectiveness. Thanks to the inclusion of this immersive technology, psychology has expanded its scope for treating not only specific phobias but also other mental disorders, providing opportunities to create scenarios that would be difficult to recreate in real life. Evidence has shown that VR does not cause adverse effects; on the contrary, it effectively mitigates fears and anxiety toward a feared object or context (Carl et al., 2019).
In this respect, the pioneering work of Rothbaum et al. (1995) on acrophobia paved the way for other successful studies using VR as an exposure technique. Slater's team, for example, focused on the treatment of fear of public speaking, and so did also other authors (Slater et al., 1999; Takac et al., 2019). Other studies focus on panic disorder with agoraphobia (Freeman et al., 2022), social anxiety (Hache-Labelle et al., 2023), post-traumatic stress disorder (Difede & Hoffman, 2002; McLay et al., 2017; Rothbaum et al., 1995; 2001), body image distortion and eating disorders (Mölbert et al., 2018; Myers et al., 2004), childhood autism (De Luca et al., 2021) and even substance-related disorders such as nicotine or heroin addiction (Bordnick et al., 2012; Kuntze et al., 2001; Lee et al., 2003) and behavioural addictions such as gambling (Dickinson et al., 2020).
Results from the systematic review by Ribé-Viñes (2023) showed that participants' anxiety decreased after systematic exposure to VR flight-related environments. Therefore, exposure to the feared object through a three-dimensional environment allows the creation of settings that would not otherwise be available and involves a high degree of control (Maldonado, 2002). Individuals can expose themselves and interact with the phobic situation in real time without physically being in it; instead, they experience an immersion similar to the real world through VR goggles at a lower economic cost. According to Riva et al. (2016), it is a subjective experience that bridges the real world and virtual elements, inducing what is known as a sense of presence (feeling of being in the virtual world) within a therapeutic framework. Several studies have shown that VR generates a stronger sense of presence than imaginative exposure (Botella et al., 2015; Gottlieb et al., 2021; Hakim & Hammad, 2022; Hache-Labelle et al., 2023; Lemmens et al. 2022). In addition, VR allows individuals to be exposed to more extreme situations than a real-life setting would allow, all under the control of the therapist, making it very safe. The therapist can adjust the environmental variables, tailor the exposure hierarchy, know at all times what the patient is seeing, and identify the stimulus that provokes the fear response.
VR is more immersive than imagined exposure because it stimulates sensory modalities (visual, auditory, vestibular) that are very beneficial for people who have difficulty imagining. In addition, VR sessions can be repeated until effective desensitisation is achieved and fear and anxiety responses are reduced (Hakim & Hammad, 2022; Ribé-Viñes et al, 2023; Rothbaum et al., 2001; Smith et al, 2020; Tortella-Feliu et al, 2000). This technique is economical and safe, allowing for patient confidentiality, controlled access to private environments, and flexible and effective treatment (Wilson & Soranzo, 2015). It also supports desensitisation and reduces fear and anxiety responses, which is an additional benefit.
Given that fear of flying significantly limits opportunities for travel, professional and social development, this study aims to reduce the anxiety, worry and fear associated with flying in a 23-year-old woman through the use of virtual reality and to restore her ability to travel by air.
Method
Case Identification
The subject is a 23-year-old single woman (J) with no children, currently in her final year of business studies. She is not receiving concurrent psychiatric treatment. She has never required psychological or pharmacological intervention and does not take any drugs. She lives with her parents and is the youngest of three children. Her family is aware that she has sought help for her problem and she feels supported by them. Her socio-economic and educational level is medium-high. She has no family history of mental disorders and her relationship with her family is warm.
Reason for Consultation
The patient visited a private centre in Seville to ask for help, stating that she had not been able to travel by plane for more than four years. She reports that this problem first ocurred after a solo trip from Seville to Barcelona in 2019, when she experienced a negative incident (tachycardia, dry mouth, general malaise, dizziness and fatigue) due to poor digestion, which she associated with the flight. Following this episode, she avoided all opportunities to fly with family or friends and has only flown once (in these four years), experiencing the same anxiety symptoms as during the first episode. At the time she sought psychological help, she was very worried and anxious, convinced that her fear of flying would prevent her from going on a graduation trip organised by her peers at university. This motivated her to address the issue. Her anxiety occurs mainly when she is in the plane - during take-off, landing and throughout the flight - and less in the days leading up to the flight or before boarding. Her fear is centred on the idea of an accident, something going wrong with the plane and an emergency occurring in flight.
Case History
In terms of case history and progression, the problem arose four years ago during a domestic flight. It was the first time she had travelled alone, having previously flown with a family member or friend. About thirty minutes into the flight, she began to feel nauseous and dizzy and her heart rate accelerated. She had a very dry mouth and could not drink water, which added to her general discomfort. Narrating the event out of context, she attributes her fear of flying to the aversive experience of the physiological sensations of indigestion, as she had eaten hastily just before boarding. At that moment, however, she could only think that something terrible was going to happen and that the plane was going to crash, leaving her with no control. In this sense, it can be said that the traumatic event (general discomfort) during the flight was the aetiological factor of J's phobia of flying. Since that episode, she has avoided flying and has only travelled by air once out of necessity, experiencing significant discomfort throughout the flight. Now that her class is planning a trip, she wants to overcome this problem. J states that none of her family members share her fear of flying, nor is there anyone with a mental disorder.
Assessment Tools
The psychological assessment took place at the first session and included a customised semi-structured interview to gather information on problem history, psychophysiological responses, family background, medical and psychosocial history and other relevant aspects. This interview was supplemented by a series of standardised instruments to obtain pre- and post-treatment measures:
State-Trait Anxiety Inventory (STAI) by Spielberger et al. (1983), adapted by Buela-Casal et al. (2011). This inventory has 40 items distinguishing between State Anxiety (20 items), considered as a transient emotional state with consciously perceived feelings of tension and apprehension along with autonomic nervous system hyperactivity, and Trait Anxiety (20 items), which indicates how the person feels in general. Cronbach's alpha is 0.90 for trait anxiety and 0.94 for state anxiety.
Penn State Worry Questionnaire (PSWQ) by Meyer et al. (1990), adapted by Sandín et al. (2009). This instrument measures the tendency to experience generalised worry using 16 items on a five-point Likert scale. It has two factors: a general worry dimension and absence of worry, measured by reverse-scored items (1, 3, 8, 10 and 11). Scores range from 16 to 80, with a score of 60 or more indicating a high level of worry. Cronbach's alpha is .90 in a non-clinical population.
Fear of Flying Scale (FFS) adapted by Sosa et al. (1995) from Haug et al. (1987). This scale has 21 items covering situations related to flying, with five Likert-type response options (0 to 4, depending on the degree of anxiety provoked). It assesses three factors: fear of flying (4 items, ranging from 0 to 16 and Cronbach's alpha of .97), fear during the flight (8 items, ranging from 0 to 32, alpha of .95) and fear of flying without personal involvement, i.e. situations related to flying without the person actually being a passenger (9 items, ranging from 0 to 36, alpha of .67). There are no cut-off points for these factors; higher scores indicate greater fear of flying. Only the first two factors were considered, as the third was not clinically relevant in this case.
Expectancy Scale for Fear of Flying (ESFF) adapted from Gursky & Reiss (1987) and psychometrically validated by Sosa et al. (1995). It has 19 items and two subscales: Hazard Expectancy (9 items) assesses the frequency (0 to 3) of various catastrophic thoughts regarding the possibility of physical harm during flight or potential problems with the aircraft. Scores range from 0 to 27, with a Cronbach's alpha of .86. The Anxiety Expectancy subscale, with 10 items scored from 0 to 4, assesses expectations of experiencing various physiological anxiety symptoms during the flight. Scores range from 0 to 40, and Cronbach's alpha for this subscale is .91.
Wolpe's Subjective Units of Anxiety (SUDs) (1969), which measures subjective anxiety during virtual exposure sessions on a scale of 0 to 100 (0: no anxiety; 100: very high anxiety).
Differential diagnosis
J has been diagnosed with a situational phobia (F40.248) related to flying according to DSM-5 criteria (American Psychiatric Association, 2014). Although the patient describes herself as a nervous person who is easily upset, no other mental disorder has been identified as there are no impairing problems in other areas of her life (work, social or family).
Objectives of the intervention
The main aims of the intervention are: a) to reduce J's anxiety about flying, b) to reduce and diminish the anticipation of danger and catastrophic automatic thoughts during flights and to reduce worry, and c) to enable her to fly both alone and with others without experiencing anxiety symptoms.
Design
A single-case design (N = 1) with an AB structure over a total of eight sessions was used. It begins with phase A, in which the baseline is established through initial data collection. For this purpose, questionnaires are administered to assess the constructs of interest (fear of flying, anxiety, worry, danger expectancy). On the basis of the information obtained, phase B follows, in which an intervention is carried out with the person concerned. At the end of the intervention, the instruments are administered again to measure changes in the parameters assessed. After being informed of the purpose of the study and having been told what the treatment would entail, J signed the informed consent form in accordance with the Declaration of Helsinki (World Medical Association, 2013).
Intervention Plan and Treatment Objectives
The case approach is delivered over eight weekly one-hour sessions, following the treatment model recommended by Dilgul et al. (2020). The tasks focus on the following aspects
Pre-treatment assessment and psychoeducation related to fear of flying, avoidance and its consequences, and aircraft safety (1 session). The aim is to provide the patient with an objective understanding of her problem so that she can develop a more balanced perception of the benefits of air travel.
Gradual exposure via VR using the Psious platform (2017). This application uses a virtual reality headset kit and high quality headphones. It offers different scenarios to simulate experiences similar to flying: at home, on the way to the airport, at the boarding gate and on the plane. In this case, the boarding gate and in-flight environments were mainly used, with different "events" controlled by the therapist: time of day (night, day), weather conditions (rain), number of passengers on the plane (few or many people), take-off, landing, turbulence, announcements, etc., allowing exposure to the feared object in a controlled environment that the therapist can stop at any moment. These exposures were carried out over six sessions, lasting between 30 and 40 minutes depending on the scenario, and the intensity was gradually increased according to the patient's tolerance in order to achieve habituation. This procedure allowed for the monitoring of the patient, communication with her, full control of the environment and quantification of the level of anxiety using Subjective Units of Distress (SUDs; Wolpe, 1969), which range from 0 to 100 (0 being no anxiety, 100 being very high anxiety).
In each session, prior to the VR exposure, the patient was verbally prepared with an emphasis on psychoeducational aspects related to air travel, emphasising the importance and comfort of flying to distant places and the benefits of this opportunity.
Post-treatment assessment and feedback on achievement of therapeutic goals and relapse prevention (1 session). Following the final treatment session, a post-treatment psychological assessment was conducted using the same measures as in the first session. In addition, the results obtained were communicated, together with detailed guidelines for relapse prevention.
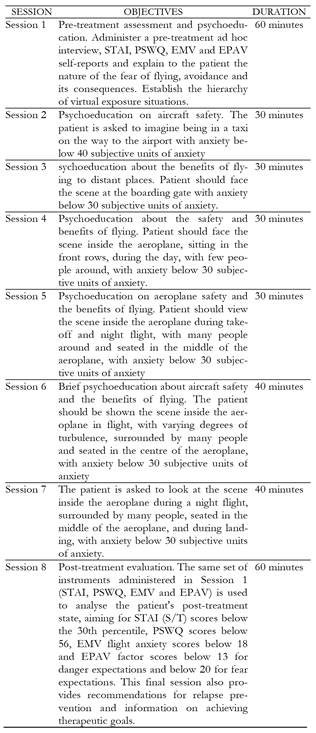
Table 1 summarises the description, set objectives and timeframe of the eight sessions conducted.
Data Analysis
As this is a single-case study, the clinical significance criterion proposed by Jacobson and Truax (1991) was used to assess treatment efficacy. This allows an analysis of the patient's progress and determines whether the changes observed are due to treatment rather than chance. These authors consider a change in the patient's functional performance as an efficacy parameter. This method is based on two primary constructs: a) the cut-off point (CP), which indicates whether the patient's functioning after therapy is closer to the average of the functional group than to that of the dysfunctional group, and b) the calculation of a reliable change index (RCI) to determine whether the observed change has sufficient statistical power to be considered real (p < 0.05). An RCI greater than 1.96 (when improvement implies an increase in post-test scores) or less than -1.96 (when clinical improvement implies a decrease in scores) is sufficient to consider the change real, as it is extremely unlikely to be due to chance (p < .05). The calculation algorithm is expressed as follows RCI = ((Xpost - Xpre) / Sdiff), where Xpre is the pre-treatment score, Xpost is the post-treatment score, and Sdiff is the standard error of the difference between the two measures, where (Sdiff = SD x √(1 - Rxx) x √2); SD is the standard deviation in the clinical sample, and Rxx is the reliability of the measure. Thus, a clinically significant change is found when post-pre ≥ 1.96×Sdiff or post-pre ≤ -1.96×Sdiff. Based on the CP and RCI, the method suggests several possible classifications according to the level of change (Jacobson & Truax, 1991; Jacobson et al., 1999): recovered (those who achieved both the CP and the required RCI), improved (those who did not achieve the CP but the RCI), unchanged (those who did not meet either criterion), and worsened (those who achieved a reliable RCI but in the opposite direction of improvement).
Results
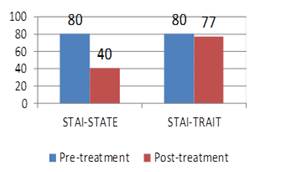
As shown in Figure 1, the virtual exposure intervention to aircraft scenarios significantly reduced patients' state anxiety, characterised by situational anxiety responses, whereas trait anxiety, a stable trait, showed no relevant changes.
In order to confirm that the changes in anxiety levels were not due to instrument error, but rather represented real and reliable effects, the RCI was applied, yielding the results shown in Table 2. A score of -8.71 for state anxiety indicates a substantial improvement, in contrast to -0.54 for trait anxiety, which is not statistically significant (Table 2).

A decrease in worry, fear of flying and expectation of danger was observed after treatment, as shown in Figure 2.
The RCI for worry and fear of flying (measured by PSWQ and EMV) indicates that the post-treatment changes are highly significant and exceed the expected variability, indicating real improvement. Similarly, danger and anxiety expectations (assessed by EPAV), including catastrophic thoughts and physical anxiety symptoms, also decreased significantly, confirming the efficacy of the intervention, as shown in Table 3.
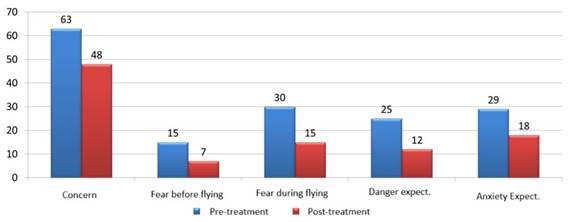
Figure 2: Pre- and Post-Treatment Results in Worry (PSWQ), Fear of Flying (EMV), and Expected Danger and Anxiety of Fear of Flying (EPAV)

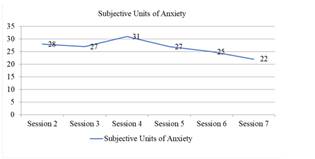
The intervention also impacted subjective units of anxiety (SUDs), which progressively decreased with each virtual exposure session on the plane (Figure 3). Although anxiety did not fall below 30 SAUs in the fourth session (the first inside the airplane with a flight simulation), subsequent sessions reached minimum levels of 22 on a 0 to 100 scale, indicating clear progress in managing anxiety in simulated flight situations.
Discussion
This highly standardised and controlled study presented the case of J, who sought private counselling for a specific phobia of flying. The aim was to reduce the situational anxiety, fear, worry and danger expectations associated with flying, using a cognitive-behavioural approach, mainly involving virtual reality exposure therapy, using materials from Psious. The treatment protocol consisted of eight sessions, two of which were pre-treatment (first) and post-treatment (last) assessments. Sessions were designed to last approximately 60 minutes each, although flexibility was allowed to accommodate the patient's needs.
Several clinically meaningful virtual scenarios were used, both before boarding and during the flight, allowing J to interact and immerse herself in the feared situation with maximum realism in a controlled environment. This immersion was effectively achieved in all sessions, particularly in the fourth session, the first virtual scenario inside the aircraft, where moderate levels of anxiety prevented achievement of the initial goal. However, as the treatment progressed, the levels of anxiety, fear and danger expectancies associated with flying gradually decreased. Based on the results of the post-treatment assessment, J showed positive progress in terms of her fear of flying and related symptoms. All post-treatment assessment instruments showed significant reductions in scores, suggesting that the virtual reality exposure was effective and achieved the therapeutic goals. These results are consistent with previous studies (Baños et al., 2001; Botella et al., 2007; Kahan et al., 2000; Klein, 1998; North et al., 1997; Rothbaum et al., 1995; Wiederhold et al., 1998) describing the efficacy of virtual reality in individual case studies.
Most studies focus on subjective symptom burden, neglecting psychophysiological parameters; however, in this paper, subjective units of anxiety (SUDs) have been included. It can be seen that subjective anxiety unit values were relatively dispersed around the mean, with limited variability between scores. In the first virtual exposure session inside the aircraft (session 4), the expected reduction was not achieved, possibly due to the novelty of the virtual situation and the significant emotional involvement induced by the sense of presence inside the aircraft, the situation that elicited the greatest fear, leading to anxiety and discomfort. However, in subsequent exposures, SAUs significantly decreased and the patient's verbal responses during the sessions were also positive. These findings are consistent with those of Beckham et al. (1990), who observed that emotional processing, together with heightened physiological responses during exposure and subsequent decrease, was associated with improved therapeutic outcomes.
The efficacy of the treatment was further evidenced by J's report that, two months after completing the treatment sessions, she was able to complete her end-of-course trip with her classmates without experiencing any anxiety or worry about a potential emergency during the flight. Consequently, it can be said that the therapeutic goals have been maintained at least in the medium term and that a clinically significant change has occurred according to Jacobson and Truax (1991), as J. has resumed normal functioning, comparable to her classmates, qualifying her as part of the functional population. In the terms of Kraemer et al. (2003), it can be affirmed that the intervention effectively resolved the problem that prompted her consultation and improved her quality of life (Kazdin, 1999).
Although this is a single-case study, which limits the generalisability of the results, and self-report measures were used to collect responses, these limitations do not diminish the conclusion that virtual reality resources are a highly recommended treatment alternative for specific phobias, with efficacy comparable to traditional methods, as also suggested by previous studies (Browning et al., 2023; Cardos et al., 2017; Ribé-Viñes et al., 2023).
In addition, the methodology used in this study, based on reliable change scores, guarantees that the post-intervention change is not only statistically significant, but also clinically relevant. Consequently, the results can be considered positive both quantitatively, based on objective post-treatment data, and qualitatively, based on the patient's expressed satisfaction. On completion, she confirmed that she had achieved a very positive outcome for her future, enabling her to face flying without experiencing any symptoms of anxiety, fear or worry.
The use of VR in this case of fear of flying represents a significant therapeutic success and proves to be a useful, easily applicable and highly reliable gradual exposure procedure in the treatment of specific phobias.

