










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.28 no.1 Zaragoza ene./mar. 2014
https://dx.doi.org/10.4321/S0213-61632014000100002
Self-reported screening questionnaire for the assessment of Joint Hypermobility Syndrome (SQ-CH), a collagen condition, in Spanish population
Antonio Bulbena, MD, PhD*,**,***; Núria Mallorquí-Bagué, MSc*,****; Guillem Pailhez, MD, Ph.D*,**,***; Silvia Rosado, RN**; Ignacio González, MD*****; Josep Blanch-Rubió, MD, PhD****** and Jordi Carbonell, MD, PhD******
*Doctorate program in Clinical Psychiatry and Psychology. Department of Psychiatry and Forensic Medicine. School of Medicine. Universitat Autonoma de Barcelona (UAB), Spain
**Anxiety Unit. Institute of Neuropsychiatry and Addictions (INAD). Hospital del Mar. Universitat Autònoma de Barcelona. Barcelona, Spain
***IMIM (Hospital del Mar Medical Research Institute), Barcelona, Spain
****Psychiatry, Psychology and Psychosomatics Department. Institut Universitari Quirón Dexeus. Barcelona, Spain
*****Primary Health Centre: Apenins-Montigala. Badalona, Spain
******Rheumatology service. Hospital del Mar. Universitat Autònoma de Barcelona. Barcelona, Spain.
ABSTRACT
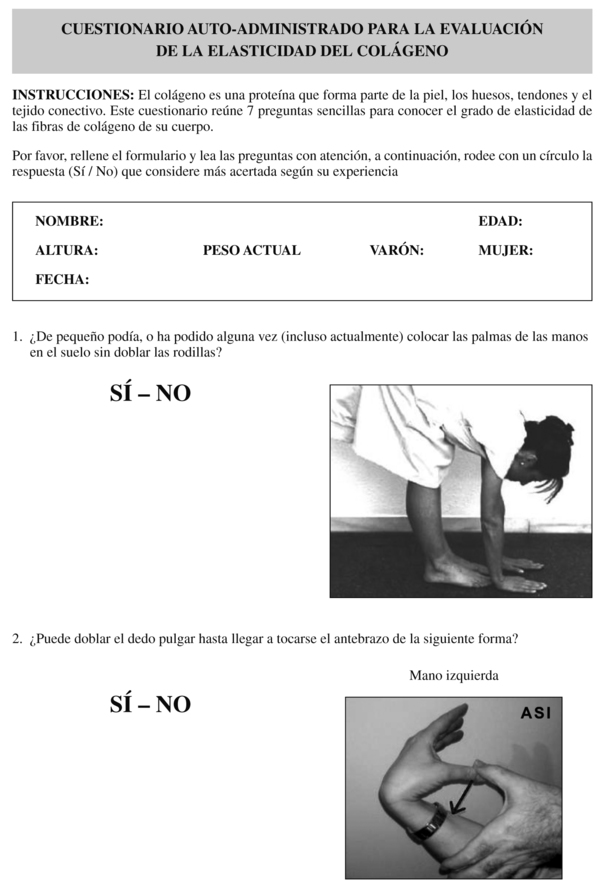
Background and Objectives: To develop a self-assessment screening questionnaire (SQ-CH), with image illustrated criteria to easily identify collagen anomalies and to assist Hypermobility's evaluation in a Spanish sample.
Methods: One hundred ninety one participants were recruited form an anxiety outpatient unit of a general university hospital and from a primary care setting, underwent a complete and rigorous evaluation of hypermobility. First, all participants completed the self-reported measures for the screening of Hypermobility Syndrome, the 7 self-reported items in y/n format aiming to validate (SQ-CH) and the 5 item self-reporting questionnaire of Hakim and Grahame (2003). Secondly, each of the participants was individual assessed by a trained clinician on the Beighton and Hospital del Mar evaluation for the diagnosis of Joint Hypermobility Syndrome.
Results: Significant correlations were found between the SQ-CH and the Beighton and Hospital del Mar scales as well as with the 5-item self-reporting questionnaire. Results on temporal stability, specificity and sensitivity of the SQ-CH were satisfactory, and the best cut-off point was set at 3 positive items (i.e. answered affirmatively).
Conclusions: The developed screening questionnaire for hypermobility (SQ-CH) is, to our knowledge, the first self-assessment questionnaire to evaluate the symptoms of the joint hypermobility syndrome in a Spanish population. It has shown good validity and good reliability and is therefore ready for its use as a screening tool to assess this collagen condition in all sort of potential suffers, particularly, patients suffering from anxiety.
Keywords: Joint hypermobility; Diagnosis; Anxiety disorders; Psychometrics; Questionnaires.
Introduction
Joint Hypermobility Syndrome (JHS) is an inherited connective tissue disorder characterized by a generalized collagen abnormality with an increase of active or passive joint mobility. The estimated prevalence of Joint Hypermobility ranges between 10-20% in western countries and it is more frequent in women (3:1). However, in spite of being a source of pain and distress, JHS often goes unnoticed and its prevalence still remains unknown1,2.
Clinical features of JHS are always associated to the connective tissue and can either be articular or extra-articular. Specifically, patients with JHS are prone to present chronic pain (e.g. arthralgia, soft-tissue rheumatism, chronic with spinal pain, rheumatoid arthritis and headaches)3; asthma4; anxiety disorders (particularly panic, agoraphobia and social phobia)5,6; an increased incidence of cardiac (Mitral Valve Prolapse, high elasticity of the aortic wall), digestive problems (reflux, irritable bowel syndrome, diverticulosis)7 and, the so-called functional illnesses such as fibromyalgia, temporomandibular joint disorder and chronic fatigue3.
Nowadays, JHS requires a clinical diagnosis which involves a physical examination applying standardised criteria8. In clinical practice, the most frequently used criteria are the Beighton's (1988)9, the Brighton's10 and the Hospital del Mar's criteria11. The Beighton scoring system is a fast and easily conducted examination. It consists of five items that describe nine movements for exploring the mobility grade on some of the patient joints; being the highest score (nine), the highest pro-bability to have JHS. The Brighton revised criteria add some extra-articular features for the JHS assessment and point out different scores according to age. The Hospital del Mar criteria were obtained after a multivariate analysis of margins from the original Carter & Wilkinson's, the Beighton's and the Rotés' criteria. This new scale showed consistent indicators of reliability, internal consistency and predictive validity, and provided evidence for using different scores for each gender. It consists of ten items (measuring articular and extra-articular features), and similarly to the Beighton's method one point is given for each criterion up to a maximum score of 10; a high score may be an indicative of JHS.
The cut-off point for the diagnosis of JHS in any of these scales is based on clinical criteria since there is no gold standard established so far. In previous studies cut-off points chosen were based on the author's view, target sample or procedure difficulties. These cut-off points matched the most widely accepted as appropriated: 4/5 for the Beighton's method (from 0 points to 4 not JHS / from 5 points to 9 JHS) and 3/4 for men and 4/5 for women in the Hospital del Mar criteria. In 2003, Hakim & Grahame12 published the first self-administered screening questionnaire to detect hypermobility, with satisfactory reliability and validity. Analysis showed that a positive answer to any two questions in the five-part questionnaire gave the highest combined sensitivity and specificity (80-90%) for detecting hypermobility.
The aim of this study is to develop a self-administered screening questionnaire to detect Joint Hypermobility Syndrome (SQ-CH), simple and reproducible, with pictures attached to each item in order to facilitate the JHS detection in a Spanish population.
Method
Participants
A hundred and fifty eight patients between 18 and 60 years old were consecutively recruited from an anxiety outpatient unit belonging to a general university hospital. Ano-ther set of thirty three subjects were recruited in a primary care setting for reliability means. Patients suffering from any disease that could have hindered JHS evaluation were excluded of the study.
Instruments
All outpatients underwent a socio-demographic interview. Hypermobility syndrome was screened through a self-assessment criteria set which included the 7 criteria Screening Questionnaire to detect Hypermobility (SQ-CH) aiming to be validated, which includes the basis of the 5 item self-reporting questionnaire of Hakim and Grahame (2003). Diagnosis of JHS was conducted through the JHS physical examination which was based on the Beighton's9 and Hospital del Mar's11 criteria. All physical examinations were conducted for a specialised clinician.
The development of the self-assessment questionnaire SQ-CH consisted of two steps: a detailed Spanish translation of the Hakim and Grahame's five criteria, including a more detailed wording12 and the addition of two new criteria. Added criteria were extrarticular items known to be present in the complete syndrome. All seven items are in dichotomy format (yes/no) and included an attached image for comprehension purposes; one point is given for each criteria answered affirmatively (minimum 0, maximum 7 points) (annex 1).


Procedure
Two trained and validated clinicians (S.R and I.G) carried out JHS assessments applying the mentioned criteria. Both examiners had previously been validated on the basis for agreement between them and clinical rheumatologists' standard (kappa inter-examiners reliability ranged from 0. 8 to 1). These examiners were unaware of the SQ-CH score results. To assess test re-test reliability, the SQ-CH was administered and re-administered after one week to 33 participants. Before taking part in the study, patients received an oral and written explanation of the data recollecting protocol; written consent for publication was obtained from all the patients. Hospital del Mar ethical committee approval was sought and granted.
Statistical analysis
Socio-demographic descriptive data and JHS characteristics were studied. Clinimetric properties evaluated in the SQ-CH were: (a) temporal stability (b) internal consistency, (c) concurrent validity of SQ-CH questionnaire compared to Beighton and Hospital del Mar criteria respectively, and to the self-reporting questionnaire of Hakim and Grahame, (d) cut-off points and the sensitivity and specificity analysis, (e)sensitivity, specificity and odds ratio for each item studied according to the cut-of point suggested (f) analysis of positive and negative predictive value, and percentage of wrong classified according to the estimated prevalence. Non-parametric techniques were chosen because the normal distribution of the joint hypermobility measures could not be guaranteed. Statistical analysis was conducted by the SPSS (19.0) software for Windows.
Results
The mean age of the sample was 35.52 years (SD = 10. 18) and 71. 27% were women. Most of the recruited participants of the sample (89.9%) met DSM-IV-TR inclusion criteria for Panic and/or Phobic cluster disorders.
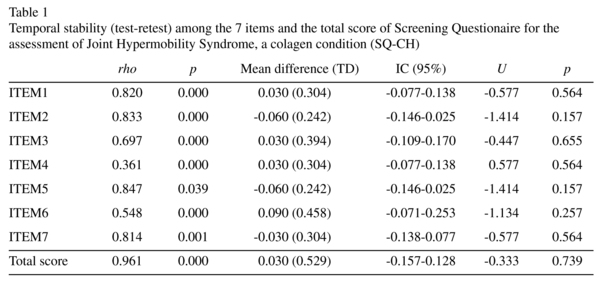
Temporal stability of the SQ-CH assessment showed a tau-kendall index of 0.911 and an intraclass correlation coefficient (ICC) of 0.961 (IC 95% = 0.922-0.980). Positive and statistically significant correlations were obtained among the 7 items that compose the questionnaire and the total score of SQ-CH. Mean equality assessment on test-retest was granted (Table 1). The interval consistency of the questionnaire (Cronbach alpha coefficient) was of 0.713.
Due to the high correlation index (r = 0.9; p<0.001) and the results similarity between JHS measures, those obtained by Beighton's evaluation system are not included. According to the Hospital del Mar criteria, the prevalence of JHS in the sample is 37.3%. SQ-CH is positively correlates with both the Hospital del Mar criteria (rho = 0. 745; p<0.001) and the self-reporting questionnaire of Hakim and Grahame (rho = 0.857; p<0.001).
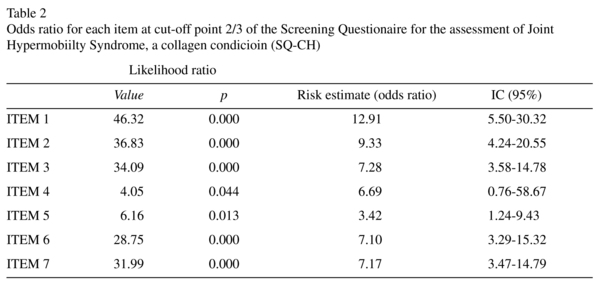
The cut-off point proposed for this sample population is 2/3 (from 0-2 lack of JHS and from 3-7 JHS) with a sensitivity of 0.78 and a specificity of 0.24. The area under the ROC curve of the 7 self-assessed criteria (SQ-CH) is 0.861.Sensitivity and specificity percentages for the 2/3 cut-off point in relation to the Hospital del Mar criteria are 78.0% and 75.8% respectively, obtaining a percentage of 65.75% correctly classified as positive and 85.2% correctly classified as negative. Likelihood ratios are positive and significant for each item according to the cut-off point in relation to the total score in SQ-CH (Table 2).
Finally, the estimated prevalence of JHS when measured by SQ-CH is of 44.3%. With a positive predictive value of 92.79%, negative predictive value of 46.22% and a propor-tion of wrongly classified of 22.48%.
Discussion
The proposed self-assessment questionnaire for JHS screening in a Spanish sample (SQ-H) has shown adequate clinimetric properties. Global correlation between SQ-CH and the widely used criteria of Beighton9 and Hospital del Mar11 are high as expected. Correlation between SQ-CH and the self-reporting questionnaire of Hakim and Grahame12 also showed high correlation. Therefore, data in temporal stability, specificity and sensitivity are appropriate for a screening questionnaire.
The SQ-CH has been created as a screening tool to facilitate the JHS diagnosis, which requires a high sensitivity and temporal stability. Results shown in the test-retest indicate temporal stability in both the inter-item reliability and the total score of the questionnaire reliability. The internal consistency is close but under 0.8. However, the fact that JHS has a huge diversity of clinical manifestations and items have to measure different constructs might explain a lower internal consistency.
Based on the validity results, the cut-off point is established at 2/3 (patients would pro-bably have JHS at a score of 3 or more). Considering this cut-off point, 44. 3% of the studied sample has JHS, with a 78% of sensitivity compared to the criteria of Hospital del Mar. Previous studies have shown a 10-20% prevalence of hypermobility affection in general population and a 60%-70% of JHS in patients suffering from panic/phobia cluster1,2,5,6. Recently a longitudinal study concluded that JHS is a risk factor for developing anxiety disorders, showing that patients with JHS present a higher incidence (RR: 22.6) of anxiety disorders than non JHS patients13. Furthermore, a study conducted with brain magnetic resonance imaging (MRI) techniques observed structural differences in emotional-processing brain regions and specifically concluded that bilateral amygdala volume distinguished those participants with from those without hypermobility14. On the bases of these findings, the target sample of the study was deliberately chosen from an anxiety unit in order to detect more hypermobility subjects; therefore the percentage obtained was higher than in the general population but lower than the one proposed in studies that used an anxious clinical sample5,6. The observed difference with other anxious clinical samples might be due to the fact that 10% of our sample includes anxiety diagno-sed spectrum disorders (obsessive-compulsive disorders, non-specified anxiety disorder and generalised anxiety disorder) but not panic/ phobic cluster which is described to be the most associated to joint hypermobility syndrome.
According to the estimated prevalence, the high positive predictive values and the low proportion of cases wrongly classified, reaffirm the questionnaire's functionality. Finally, validity measures guarantee a correct diagnosis evaluation in hypermobility and high correlation compared to criteria with clinical exploration, already mentioned above.
Further contributions of this Spanish questionnaire are the additional attached images which enable the interpretation of the images, moreover we have avoided the term joint because the questionnaire includes extra-articular features and instead, the word collagen should be more appropriate to name the clinical condition.
In regard to the limitations, a wide age range might have been a confounding variable, even though we excluded ages ranging below 18 and above 60 in order to avoid a possible bias in the JHS exploration and evaluation. On the other hand, the cut-off point settled entails an adequate but not high percentage of specificity. Nevertheless, it is adequate in statistical terms and, in clinical means, its usefulness lies in the screening capability. Hence, in order to evaluate and properly diagnose JHS, the original criteria with clinical exploration will also be needed. Furthermore, the number of sample participants should preferably be larger referring to ROC statistical analyse terms. Finally, due to the study's design and the impossibility to repeat the evaluations in all participants, test-retest reliability measures have not been applied to the complete sample but to a group of 33 participants. However, the obtained results guarantee the stability of the questionnaire.
In summary, the developed screening questionnaire for Joint Hypermobility Syndrome (SQ-CH) is, to our knowledge, the first self-assessment questionnaire to detect JHS in Spanish and follows the original line opened in English by Hakim and Grahame with their questionnaire. It is useful and appropriate as a screening tool, previous to the clinical diagnosis (hetero-administered). Therefore, it presents an important contribution in the JHS diagnosis and, might provide an easy way to assess this collagen condition in all sort of potential sufferers of JHS and particularly, patients suffering from anxiety disorders.
Key message
The Screening Questionnaire for Collagen condition and Hypermobility's assessment (SQ-CH) has shown good validity and reliability in a Spanish sample and therefore is useful and appropriate.
References
1. Beighton PH, Grahame R, Bird HA, eds. Hypermobility of joints. Berlin: Springer, 4th edition; 2012. [ Links ]
2. Ross J, Grahame R. Easily mised? Joint hypermobility syndrome. BMJ 2011; 342: 7167. [ Links ]
3. Keer R, Grahame R. Hypermobility syndrome. New York: Butterworth Heinemann; 2003. [ Links ]
4. Morgan AW, Pearson SB, Davies S, Gooi HC, Bird HA. Asthma and airways collapse in two heritable disorders of connective tissue. Ann Rheum Dis 2007; 66: 1369-1373. [ Links ]
5. Bianchi Sanches S, De Lima Osório F, Udina M, Martin-Santos R, Crippa JA. Anxiety and joint hypermobility association: a systematic review. RBP 2012; 34 Suppl: 53-68. [ Links ]
6. Martin-Santos R, Bulbena A, Porta M, Gago J, Molina L, Duro JC. Association between the joint hypermobility syndrome and panic disorder. Am J Psychiatry 1998; 155: 1578-1583. [ Links ]
7. Mishra MB, Ryan P, Atkinson P, Taylor H, Bell J, Calver D, et al. Extra-articular features of benign joint hypermobility syndrome. Br J Rheumatol 1996; 35: 861-866. [ Links ]
8. Remvig L, Juul-Kristensen B. Need for international consensus on examining for joint laxity: comment on the article by Clinich et al. Arthritis & Rheumatism 2011; 63 (12): 4039-4040. [ Links ]
9. Beighton P, Grahame R, Bird H. Hypermobility of joints. London: Springer; 1999. [ Links ]
10. Grahame R, Bird HA, Child A, Dolan L, Edwards-Fowler A, Ferrell WR, et al. The revised (Brighton 1998) criteria for the diagnosis of benign joint hypermobility syndrome. J Rheumatol 2000; 27: 1777-1779. [ Links ]
11. Bulbena A, Duró JC, Porta M, Faus S, Vallescar R, Martín-Santos R. Clinical assessment of Hypermobility of joints: Assembling criteria. J Rheumatol 1992; 19: 115-122. [ Links ]
12. Hakim AJ, Grahame R. A simple questionnaire to detect hypermobility: an adjunct to the assessment of patients with diffuse musculoskeletal pain. Intern J Clinical Practice 2003; 57: 163-166. [ Links ]
13. Bulbena A, Gago J, Pailhez G, Sperry L, Fullana MA, Vilarroya O. Joint Hypermobility Syndrome is a Risk Factor Trait for Anxiety Disorders: a 15-year follow-up cohort study. Gen Hosp Psychiatry 2011; 33(4): 363-370. [ Links ]
14. Eccles JA, Beacher FDC, Gray MA, Jones CL, Minati L, Harrison NA, et al. Brain structure and joint hypermobility: relevance to the expression of psychiatric symptoms. BJ Psych 2012; 200: 508-509. [ Links ]
![]() Correspondence:
Correspondence:
Antonio Bulbena
Hospital del Mar
Passeig Marítim, 25
08003 Barcelona, Spain
Tel.: (+34) 93 248 3495
Fax: (+34) 93 248 3445
E-mail: abulbena@gmail.com
Received: 14 June 2013
Revised: 18 November 2013
Accepted: 2 December 2013

