










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Adolescents and young people are especially vulnerable to alcohol and tobacco consumption, affecting neurodevelopment during these stages.1,2 In addition to health consequences, it has been shown that alcohol and tobacco consumption also have a high economic and social impact on the populations.3-5 In Spain, 70.5% and 30.7% of adolescents aged between 14 and 18-years old reported alcohol and tobacco use within the last year, respectively.6
In the last decade there has been increasing interest in how the urban, social, and cultural environments influence people's behaviors related to health, such as substance use. 7Evidence suggests that greater accessibility to alcohol and tobacco products and higher exposure to their promotion may increase alcohol and tobacco consumption among adults and adolescents.8-10 The exposure to alcohol and tobacco accessibility and promotion is not evenly distributed in the space and several inequalities have been described according to neighborhood sociodemographic deprivation, with greater exposure in the most deprived areas.11,12
Previous studies have characterized alcohol and tobacco environments around secondary schools in the city of Madrid. A recent study highlighted that 75% of tobacco outlets are located closer than 300 meters to a school.13 Another study found that in Madrid there is an average density of 26 alcohol outlets within buffers of 400 meters around schools, with a mean distance of 82 meters to the closest outlet.14 These results show a high exposure to alcohol and tobacco around schools, and future studies should explore how this exposure may influence alcohol and tobacco consumption among adolescents.
This study aims to describe the accessibility to and promotion of alcohol and tobacco around secondary schools in Madrid and its distribution in relation with area-level socioeconomic deprivation; analyze the relationship between this exposure and individual alcohol and tobacco consumption among secondary school students between 14 and 18 years old in the city of Madrid; and explore other facilitators and barriers that may encourage or prevent alcohol and tobacco consumption among adolescents.
Method
Study design
This is a cross-sectional mixed-methods study carried out in Madrid, Spain, in three phases (Fig. 1). In phase 1, we conducted a systematic social observation in 500-meters street network buffers around secondary schools to collect contextual data on alcohol and tobacco accessibility and promotion. In phase 2, we surveyed a sample of secondary school students between 14 and 18-years about sociodemographic data and alcohol and tobacco consumption, and determinants of its consumption. In phase 3, we performed semi-structured interviews and one discussion group with students in these centers who have ever consumed alcohol or tobacco to complement the information gathered by the questionnaire in phase 2. Transversally, we will geocode all data obtained from these three phases to explore spatial patterns of the presence of alcohol and tobacco elements in the environment and consumption among adolescents by using Geographic Information Systems (GIS).

Phase 1: systematic social observation around selected secondary schools
All schools that taught secondary education in the city of Madrid (n = 565) were classified into nine strata defined as the combination of the tertiles of neighborhood socioeconomic status (SES) and tertiles of alcohol and tobacco outlet density (i.e., SES High-High Density; SES High-Medium Density; etc.). To account for deprivation, we used a validated predefined index, which includes indicators based on unemployment, precarious employment, occupational class, educational level, and property value.15 We obtained alcohol and tobacco outlet locations from two public databases.16,17 We defined outlet density as the number of outlets within a street network buffer of 500 meters around schools, using ArcGIS 10.6 (Esri, Redlands, CA, USA). We defined a “strata-balanced” strategy to contact and invite schools for participation to ensure a minimum of six centers within each strata. This may guarantee a minimum geographic variability of cases within each strata by including centers from different neighborhoods throughout the city (and avoid geographic-location bias). Centers within each strata were ranked by their alcohol and tobacco outlet density value. In strata representing high neighborhood outlet density, the contact of centers with the highest densities were prioritized. In contrast, the contact of centers with the lowest densities were prioritized in low neighborhood outlet density strata. Centers in medium neighborhood outlet density strata were randomly ranked for contact prioritization. The response ratio was 12.42%.
We used systematic social observation to gather data on alcohol and tobacco points of sale, promotion elements/banners and signs of consumption within a predefined street network buffer of 500 meters around schools that accepted to participate in the study. Data were collected between August and October 2021, excluding school holiday weeks. An updated version of the OHCITIES questionnaire18,19 was used to record the alcohol items. We modified an existing questionnaire used elsewhere to collect tobacco exposure.20-22
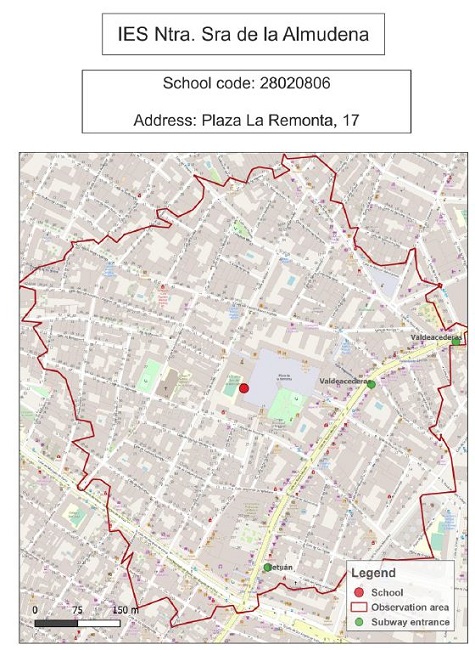
We provided theoretical-practical training to fieldworkers for data collection of alcohol and tobacco environments. We prepared maps of the buffer observation area around each secondary school (Fig. 2).
Phase 2: individual data collection
We conducted a survey among students between 14-18 years, enrolled in secondary schools in the city of Madrid between February and April 2022. An initial sample size of 1,089 students was calculated, 363 participants for each socioeconomic level stratum (assuming power of 80% and losses of 20%). This would allow us to detect changes in alcohol and tobacco prevalence of 7% between different socioeconomic strata based on the results obtained in a previous study.23 Forty nine of the 55 centers involved in this study agreed to participate in the collection of individual consumption data, obtaining a total sample of 2287 students (with a loss of six centers in this phase, of which four were from strata representing high SES and high or medium alcohol and tobacco outlet density areas).
The questionnaire included information related to sociodemographic data, alcohol and tobacco consumption patterns and determinants of their consumption. Alcohol and tobacco related questions were based on the Survey on Drug Use in Secondary Education in Spain (ESTUDES).24 The questionnaires were provided and filled in paper format, except for seven centers that claimed for an online format. In these cases, we used a free online survey tool (https://www.surveymonkey.com).
Phase 3: Qualitative data collection
A theorical, intentional, non-probabilistic purposive sampling was carried out.25 Inclusion criteria were being a student between 14 and 18 years of age and having ever consumed alcohol or tobacco. We recruited informants through the dissemination of a flyer in schools. We performed twenty semi-structured interviews (six from schools located in high and medium SES neighborhood, respectively, and eight from low SES neighborhood schools) and a discussion group (organized with five students from a medium SES neighborhood school) between April and September 2021. The topics covered in the interviews and discussion group tried to complement the information collected by the questionnaire in relation to alcohol and tobacco consumption patterns and factors influencing its consumption. Moreover, a section to explore health promotion strategies to prevent alcohol and tobacco consumption was included.
Statistical and geographic analyses
We will obtain prevalence ratios of consumption and consumption patterns. We will carry out qualitative and thematic descriptive analysis using ATLAS-ti software26 and we will use sequential explanatory method27 to relate quantitative and qualitative results. Transversally, we will use Geographic Information Systems to geocode exposure and consumption data. Geographic Information Systems will allow us to create measurements to characterize alcohol and tobacco environment (i.e., outlet proximity and density, density and visibility of promotion elements and signs of consumption) and analyze spatial inequalities in the alcohol and tobacco accessibility, promotion and consumption among different geographies in the city of Madrid. We will use Poisson regression models with multilevel robust variance, with the individual at level 1, the educational center at level 2 and the neighborhood at level 3 to assess associations between ecological data and individual characteristics.
Ethical considerations
This study was conducted according to the principles promulgated by the Declaration of Helsinki and the Ethics Committee of the University of Alcalá (CEI/HU/2020/48, CEIP2021/5/128) granted ethical approval. We informed participants and their legal representatives about the study and we requested a written informed consent from both parties, including also the permission to be contacted in the future. Confidentiality and anonymity of all data is guaranteed.
Discussion
The quantitative measurement of environmental exposure may be subject to discrepancies in the definition of operational variables trying to address the complexities of reality, as well as depending on the quality of the data. Likewise, information collected through questionnaires may be subject to reporting biases. To try to avoid these limitations, we will carry out a quality control of the data and we will contrast the quantitative information from the individual questionnaires with the semi-structured interviews and discussion group. The main strength of this project is the use of a mixed methodology that combines qualitative with quantitative and geographic approaches. This will allow us to conduct an in-depth analysis of the relationships between the accessibility and promotion of alcohol and tobacco around schools and alcohol and tobacco consumption and its determinants in secondary school students. In addition, it will allow us to learn about other facilitators of the onset of alcohol and tobacco consumption in this population.

