










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.3 Madrid mar. 2016
LETTERS TO THE EDITOR
Disconnected pancreatic duct syndrome: complete pancreas transection secondary to acute pancreatitis
Síndrome del ducto pancreático desconectado: transección completa del páncreas secundaria a pancreatitis aguda
Key words: Pancreas. Pancreatitis. Disconnected pancreatic duct syndrome.
Palabras clave: Páncreas. Pancreatitis. Síndrome del ducto pancreático desconectado.
Dear Editor,
Disconnected pancreatic duct syndrome (DPDS) is defined by a complete discontinuity of the pancreatic duct, such that a viable side of the pancreas remains isolated from the gastrointestinal tract. The most frequent causes are acute pancreatitis and pancreatic trauma, with a 10-30% incidence in acute pancreatitis (1,2). However, there is a lack of reliable epidemiologic data. This pancreatic disruption is infrequent in clinical practice and its diagnostic and therapeutic management are controversial. We present an extreme case of disconnected pancreatic duct syndrome with complete duct disruption and pancreatic transection following acute pancreatitis, as well as the diagnostic and therapeutic processes carried out.
Case report
A 56-year-old female with a medical history of dyslipidemia and hypothyroidism was admitted to a regional hospital for severe acute idiopathic pancreatitis. During hospitalization she developed a large pseudocyst in the pancreatic neck region. The patient underwent 3 unsuccessful attempts to cannulate the pancreatic duct by endoscopic retrograde cholangiopancreatography (ERCP) as it was not possible to identify the pancreatic duct distal to the pseudocyst. Percutaneous drainage was then indicated, which resolved the pseudocyst but led to an external pancreatic fistula. The patient was discharged after conservative management of the fistula for three months, and referred to our hospital for reconsideration of the therapeutic management.
By that time, the patient was asymptomatic and the pancreatic fistula remained closed. However, she presented an exocrine pancreatic insufficiency treated with pancreatic enzyme replacement therapy. The patient underwent conservative management and close follow-up with physical examination and radiologic imaging with CT-scan or MRI alternatively with endoscopic ultrasound every 6 months.
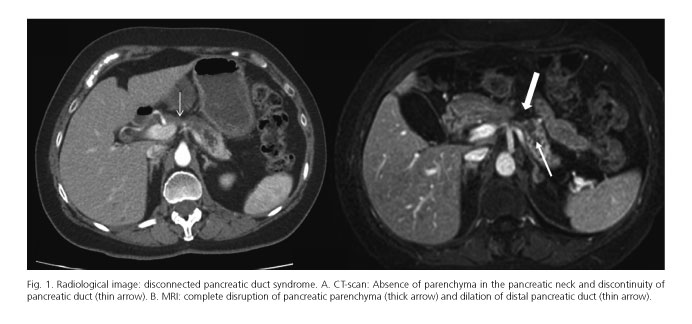
After two years of uneventful follow-up the patient developed progressive abdominal pain. Radiologic imaging demonstrated a marked dilation of distal pancreatic duct (Fig. 1 A and B). This finding was confirmed by endoscopic ultrasound suggesting an intraductal papillary mucinous neoplasm (IPMN).
Due to the above findings, the patient underwent surgery. Intraoperatively, a complete transection throughout the pancreas parenchyma with duct disruption at the neck was found, with a space between both pancreatic edges of about 2 cm, where porto-mesenteric axis was located. Distal pancreatectomy involving isolated pancreatic side and splenectomy was carried out.
The patient evolved without complications after surgery and was discharged on the 7th post-operative day. Histopathologic examination revealed chronic pancreatitis without any characteristic suggestive of IPMN.
Discussion
Disconnected pancreatic duct syndrome (DPDS) is characterized by a discontinuity of the pancreatic duct and consequent lack of continuity between a viable side of the pancreas and the gastrointestinal tract. This isolated side of the pancreas continues its exocrine function, which may lead to intra or peripancreatic collections and even cause an external pancreatic fistula (1-3).
This clinical entity was named by Kozarek et al. in 1991 (4). Its main cause is severe acute pancreatitis and, most commonly, when it is treated by percutaneous drainage or by necrosectomy. This syndrome occurs predominantly in the pancreatic neck region due to its perfusion, being an area susceptible to ischemia and, therefore, pancreatic necrosis.
The criteria for diagnosing DPDS include necrosis of at least 2 cm in the neck or body of the pancreas, the existence of viable distal pancreatic tissue from necrosis region and the extravasation of contrast material injected into the main pancreatic duct at pancreatography obtained by ERCP (5).
The main problems related to DPDS are that its diagnosis is often missed or delayed in the initial management of these patients and, hence, unnecessary or inappropriate therapeutic procedures are performed. Although there is a lack of clinical and epidemiological data and therapeutic algorithms are not clearly defined, the accumulated experience of high-volume hospitals has enabled the following conclusions (2,3,5-7): the diagnosis must be suspected after severe acute necrotising pancreatitis, primarily when collections or necrosis involve central areas of the pancreas; the diagnosis is based on CT, MRI and ERCP findings; if DPDS is suspected by radiologic imaging, percutaneous drainage must be avoided due to the risk of external pancreatic fistula development which would be difficult to resolve. Endoscopic techniques are better options if drainage or necrosectomy are needed. If the patient remains asymptomatic, a wait-and-see approach can be taken but DPDS often develops complications during follow-up. In such cases surgery should be indicated. Distal pancreatectomy (with or without splenectomy) or Roux-en-Y anastomosis are surgical options depending on anatomic conditions (size of pancreatic remnant and diameter of Wirsung duct) and physiopathology factors (diabetes and exocrine insufficiency).
Juan M. Gámez-del-Castillo1, Marina Garcés-Albir1, María Carmen Fernández-Moreno1,
Francisco J. Morera-Ocón1, Rosana Villagrasa2 and Luis Sabater-Ortí1
Departments of 1Surgery and 2Gastroenterology. Hospital Clínico.
Universidad de Valencia. Valencia, Spain
References
1. Ramia JM, Fabregat J, Pérez-Miranda M, et al. Síndrome del ducto pancreático desconectado. Cir Esp 2014;92:4-10. DOI: 10.1016/j.ciresp.2013.02.024. [ Links ]
2. Fisher TD, Gutman DS, Hughes SJ, et al. Disconnected pancreatic duct syndrome: Disease classification and management strategies. J Am Coll Surg 2014;219:704-12. DOI: 10.1016/j.jamcollsurg.2014.03.055. [ Links ]
3. Pelaez-Luna M, Vege SS, Petersen BT, et al. Disconnected pancreatic duct syndrome in severe acute pancreatitis: Clinical and imaging characteristics and outcomes in a cohort of 31 cases. Gastrointest Endosc 2008;68:91-7. DOI: 10.1016/j.gie.2007.11.041. [ Links ]
4. Kozarek RA, Ball TJ, Patterson DJ, et al. Endoscopic transpapillary therapy for disrupted pancreatic duct and peripancreatic fluid collections. Gastroenterology 1991;100:1362-70. [ Links ]
5. Sandrasegaran K, Tann M, Jennings SG, et al. Disconnection of the pancreatic duct: An important but overlooked complication of severe acute pancreatitis. Radiographics 2007;27:1389-400. DOI: 10.1148/rg.275065163. [ Links ]
6. Murage KP, Ball CG, Zyromski NJ, et al. Clinical framework to guide operative decision making in disconnected left pancreatic remnant (DLPR) following acute or chronic pancreatitis. Surgery 2010;148:847-56. DOI: 10.1016/j.surg.2010.07.039. [ Links ]
7. Pearson EG, Scaife CL, Mulvihill SJ, et al. Roux-en-Y drainage of a pancreatic fistula for disconnected pancreatic duct syndrome after acute necrotizing pancreatitis. HPB 2012;14:26-31. DOI: 10.1111/j.1477-2574.2011.00397.x. [ Links ]
