










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Cirugía Oral y Maxilofacial
versión On-line ISSN 2173-9161versión impresa ISSN 1130-0558
Rev Esp Cirug Oral y Maxilofac vol.29 no.3 Madrid may./jun. 2007
ARTÍCULO CLÍNICO
Sagittal maxillary growth in unilateral cleft lip and palate patients following functional surgery
Crecimiento sagital maxilar en fisurados unilaterales operados funcionalmente*
F. Donoso Hofer1, F. Pantoja Buljevic2, R. Pantoja Parada3
1 Servicio de Cirugía Máxilo Facial
2 Facultad de Medicina. Universidad de Chile.
3 Servicio de Cirugía Máxilo Facial.
Profesor Titular Cirugía Máxilo Facial Universidad de Chile.
Hospital Clínico San Borja Arriarán. Santiago, Chile.
*Trabajo de investigación realizado en el Servicio de Cirugía Máxilo facial Hospital Clínico San Borja Arriarán,
Santiago de Chile y en la Facultad de Odontología de la Universidad de Chile.
ABSTRACT
Objective. To compare the sagittal maxillary growth between unilateral cleft lip and palate
patients operated under functional criterion at the age of 6 months and normal
patients who were blood-related.
Design. Delaires Architectural and Structural craniofacial analysis in conventional lateral radiographs of all the
patients with an age range of 7-12 years, determining the sagittal maxillary
growth by the anterior maxillary pillar angle (C1/F1). These measurements were
analyzed using the T-test with a 99.5% significance.
Results. The real and expected value of the anterior maxillary pillar angle was determined in all
cases. By comparing the results statistically, no significant differences were
found in the mean values obtained.
Conclusion. Maxillary sagittal growth in unilateral cleft lip and palate patients operated at the age of 6 months
under functional criterion, does not differ from the growth of normal patients.
Key words: Sagittal maxillary growth; Cleft; Functional criterion.
RESUMEN
Objetivo. Comparar el crecimiento sagital maxilar en pacientes con fisura labio-máxilo-palatina
unilateral operados a los 6 meses con criterio funcional con pacientes normales
que tengan relación consanguínea directa con los anteriores.
Diseño del estudio. Análisis arquitectural y craneofacial de Delaire en
telerradiografías de perfil en ambos grupos de pacientes cuyas edades fluctúan
actualmente entre los 7 y los 12 años, determinando el crecimiento sagital del
maxilar a través de la medida del ángulo del pilar maxilar anterior (C1/F1),
sometiendo las medidas al test T de Student con una significación del 99,5%.
Resultados. Se determinó el valor real y esperado para el ángulo del pilar maxilar
anterior en todos los casos. Al comparar estadísticamente los resultados, no se
encontraron diferencias significativas en los valores promedios obtenidos.
Conclusiones. El crecimiento sagital maxilar de los pacientes con fisura labio-máxilo-palatina
unilateral operados a los 6 meses con criterio funcional no difiere del de
aquellos pacientes normales.
Palabras clave: Crecimiento sagital maxilar; Fisurados; Técnica funcional.
Introduction
The skeletal area that we call the maxilla develops in a sagittal sense, among other factors, because of sutural growth originating from mesial migration and anterior rotation movements. These movements in normal individuals are associated with the genetic characteristics expressed in the chondrocranium, in addition to the stimulation of the habitual orofacial functions.1,2
One of the most serious problems with unilateral cleft lip and palate patients is confirming that the sagittal growth of the maxilla is insufficient.3-6 This produces functional, aesthetic and psychological disturbance in patients that affects their quality of life, and certainly that of their families.
Ortiz-Monasterio demonstrated that cleft patients who had not undergone surgery, had normal sagittal growth of the middle third of the face.7 The problem then should be sought in the type and opportunity of the surgical interventions that these patients undergo, with the aim of rehabilitation.
Our interest in the subject is based on the fact that in Chile, cleft lip and palate patients represent a problem for the Public Health Body as there is a high global incidence rate, because one out of every 650 live births has this pathology. The rate varies in the population depending on the ethnic group and socio-economic strata.8
The object of this work is to verify if sagittal maxillary growth of unilateral cleft lip and palate patients can be kept within normal ranges, by adapting the sequence, chronology and surgical technique to make this as coherent as possible with normal growth and morphogenetic processes. For this, the concepts and techniques formulated by Delaire, and which in our opinion meet these conditions, were adopted.
Material and method
Of the group of cleft patients in the Hospital Clínico San Borja- Arriarán, in Santiago de Chile, ten were randomly selected with the diagnosis of unilateral cleft lip and palate. There were five males and five females and the mean age was 8.3 years (age range 7-10 years). These children were operated using the cheilorhinoplasty technique first described by Delaire:9-11 Velopalatine and lip simultaneously six months after birth. In this intervention emphasis was put on the correct reconstruction of the two muscular rings involved in the cleft: the nasolabial and the orbicular muscles. The primary closure of the maxilla was carried out between 18 and 24 months of life and neither vomerine mucosa nor palatal maxillary fibromucosa were used.11,12
None of the patients in the study group received presurgical orthopedics and they were all operated by the same surgeon (Prof. Dr. Roberto Pantoja).
The patients in the study group were compared with the patients in the control group, which was made up of 10 healthy children (4 female and 6 male), with a mean age of 9.7 (age range 7-12). These children were brothers or cousins of the individuals in the study with the aim of avoiding a genetic bias in the sample.
In order to evaluate the sagittal growth of the maxilla, profile teleradiographies were obtained of all the children. These were taken using the same equipment so that any radiographic errors were minimized. Both authors carried out the tracings independently on two different occasions according to the architectural and structural craniofacial analysis proposed by Delaire, with its update.13-15
The sagittal position of the maxilla in this analysis is defined by the value of the anterior pillar angle of the face, formed between this skeletal structure and the anterior base of the skull. This angle is thus formed by a horizontal line that joins the "M" point (union of the naso-frontal, maxillo-frontal and maxillo- nasal sutures) with the apex of the posterior clinoid process (C1 line or upper line of the skull base), and by the vertical line that is traced from the frontomaxillary joint ("FM") that passes through the nasopalatine canal and fulcrum of the canine, which corresponds to the anterior pillar of the face or canine pillar (F1 line or anterior pillar line) (Fig. 1).
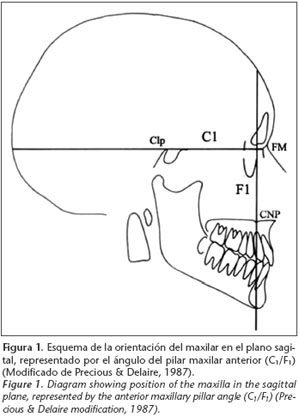
This angle therefore is the representation of the sagittal movements of the maxilla during its development, particularly its anterior rotation.
The value of the anterior pillar angle is considered normal in children when it has a value of 85º. However this value is used only as a reference as another four cranial parameters should be considered which modify it, in the sense that they influence its opening and closure.16
These parameters are: (A) the anterior angle of the skull base, (B) the sphenoid angle or the posterior skull base, (C) proportion between the height of the vault and the length of the skull base and (D) the relationship between the length of the craniofacial segment and the length of the rachidian-cranial segment of the skull base.
Depending on the results obtained for these parameters, a specific value for the anterior facial pillar angle for each individual patient will be determined, in concordance with their individual craniofacial characteristics, and which we will refer to as the Expected value.
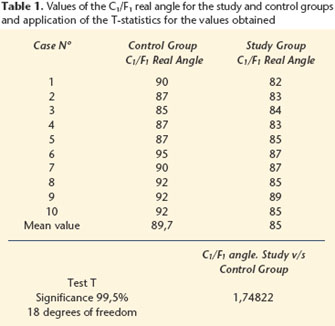
Once the corresponding measurements have been carried out for each patient and the values have been obtained by means of the cephalometric drawing, the mean value of the anterior facial pillar angles in the study group are compared statistically – the expected as well as real values. In addition, the mean values for the real angle of the anterior facial pillar of the study and control groups are compared by means of Students T-test statistics, with 18 and 9 degrees of freedom respectively, and with a significance of 99.5%.
Results
The values obtained for the angle of anterior facial pillar and from the T-test can be found in tables 1 and 2. In both cases the T-value obtained allows affirming that there are no statistically significant differences for the values of the angles obtained in the groups compared.

Discussion
The sagittal maxillary growth in a group of children with unilateral cleft lips and palates, who were operated on using functional criterion, does not differ significantly from the group of normal children with a similar age range and with a direct blood link with the previous group. (fig. 2)

Despite being a relatively small group of patients, the results indicate that a lack of sagittal midfacial development can be avoided or reduced to a large extent on adapting a sequence, chronology and surgical technique to the correct and appropriate restitution of orofacial functions, and by reconstructing the deep and superficial muscular rings.
In a similar study carried out by Adcock and Markus17 that compared unilateral cleft lip and palate patients who underwent functional and non-functional techniques, it was concluded that those patients operated using a functional technique reached growth and development levels that were similar to those in the control group, when compared with those patients operated with a non-functional technique.
Likewise Joos6 obtained similar results reconfirming that the surgical goal should be the reconstruction, at the appropriate time, of those skeletal units halted by cleft formation.
Adequate sagittal maxillary development in this group of patients is related to the early establishment of correct incisor occlusion, as previously discussed.18
As it was decided that close relationships would be given special relevance, the control group had a wider age range and, taking into consideration that in the mixed dentition period, the growth curve accelerates on nearing the puberty growth period (as from 9 years and 9 months in females and 11 years and 6 months in males)19 it is not strange for the control group to have growth values that are more advanced than those of the study group.
The cephalometric analysis used would appear to be adequate, as it has the advantage of not being based on statistical averages but rather on craniofacial distribution established by physiological alignments, which are influenced by the unique features of each skeleton, making it personalized and reliable.14
![]() Correspondence:
Correspondence:
Francisca Donoso Hofer
Departamento de Cirugía Máxilo Facial, Universidad de Chile.
Av. Santa María 571. Recoleta-Santiago, Chile
Email: frandonoso@yahoo.com
Recibido: 02.02.05
Aceptado: 06.10.06
References
1. Markus AF, Delaire J, Smith WP. Facial Balance in cleft lip and palate: Normal development and cleft palate. Br J Oral Maxillofac Surg 1992;30:287-95. [ Links ]
2. Precious D, Delaire J. Balanced facial growth: A schematic interpretation. Oral Surg Oral Med Oral Pathol 1987;63:637-44. [ Links ]
3. Bardach J. The influence of cleft lip repair on facial growth. Cleft Palate J 1990;1:76-8. [ Links ]
4. Bardach J, Eisbach K. The influence of primary unilateral cleft lip repair on facial growth: Part I Lip pressure. Cleft Palate 1977;1: 88-97. [ Links ]
5. Joos U. Evaluation of the result of surgery on cleft lip and palate and skeletal growth determinants of the cranial base. J Cranio Maxillofac Surg 1989;17:23-5. [ Links ]
6. Joos U. Skeletal growth after muscular reconstruction for cleft lip, alveolus and palate. Br J Oral Maxillofac Surg 1995; 33:139-144. [ Links ]
7. Ortiz-Monasterio F, Serrano A, Barrera G, Rodriguez-Hoffman H, Vinageras EA. Study of untreated adult cleft palate patients. Plast Reconstr Surg 1966;38:36-41. [ Links ]
8. Dabed C, Cauvi D. Survey of dentist: experience with cleft palate children in Chile. Cleft Palate-Craniofac J 1998;35:430-33. [ Links ]
9. Markus AF, Delaire J. Functional primary closure of the lip. Br J Oral Maxillofac Surg 1993;31:281-91. [ Links ]
10. Delaire J. Un example de chirurgie physiologique: la réhabilitation "primaire" du prémaxillaire dans fentes labio-maxillaires. Rev Orthop Dentofac 1991;25:453-75. [ Links ]
11. Delaire J, Mercier J, Gordeeff A. Bedhet. Les trois fibro-muqueses palatines. Rev Stomatol Chir Maxillofac 1989;90:379-90. [ Links ]
12. Delaire J, Precious D. Avoidance of the use of vomerine mucosa in primary surgical management of velopalatine clefts. Oral Surg Oral Med Oral Pathol 1985; 60:589-97. [ Links ]
13. Precious DS, Delaire J. Clinical observations of cleft lip and palate. Oral Surg Oral Med Oral Pathol 1993;75:141-51. [ Links ]
14. Delaire J, Schendel SA, Tulasne JF. An architectural and structural craniofacial analysis: A new lateral cephalometric analysis. Oral Surg Oral Med Oral Pathol 1981;52:226-38. [ Links ]
15. Delaire J. Lanalyse architecturale et structurale cranio-faciale (de profil). Principes théoriques. Quelques exemples demploi en chirurgie maxillo-faciale. Rev Stomatol 1978;1-33. [ Links ]
16. Salagnac JM. Dento Skeletal study in Delaires architectural and structural analysis. A complement adapted to orthodontic practice. Rev Stomatol Chir Maxillofac 1987;88:48-55. [ Links ]
17. Adcock S, Markus AF. Mid-Facial growth following functional surgery. Br J Oral Maxillofac Surg 1997;35:1-5. [ Links ]
18. Pantoja R, Silva S, Rodríguez N. Estudio comparativo de la oclusión dentaria entre dos poblaciones de fisurados labio máxilo palatino unilateral operados con técnica y cronología diferentes. Rev Dent Chile 2001;92:23-4. [ Links ]
19. Avendaño A, Valenzuela C. Seguimiento longitudinal de crecimiento y desarrollo, de 6 a 20 años. Área Norte de Santiago. Revista Pediátrica Stgo 1988;31:4-58. [ Links ]

