










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.15 no.41 Murcia ene. 2016
REVISIONES
Instruments and impacting factors on standard precautions knowledge among health workers
Instrumentos e fatores impactantes sobre o conhecimento das medidas de precauções-padrão entre trabalhadores de saúde
Instrumentos y factores impactantes en conocimiento de medidas de precauciones estándar entre trabajadores de la salud
Duarte Valim, Marília*; de Morais, Richarlisson Borges** and Marziale, Maria Helena Palucci***
* Nurse. Doctor Professor. University Center Octávio Bastos Foundation (UNIFEOB). Email: duartevalim@usp.br
** Nurse. Professor. Health Technical School of the Federal University of Uberlândia.
*** Nurse. Titular Professor. Department of General and Specialized Nursing of the School of Nursing of Ribeirão Preto. University of São Paulo. Brazil.
ABSTRACT
The study identified instruments for measuring knowledge and information from health professionals on standard precautions (SP); to describe the knowledge and the information of workers; to check dimensions and contents evaluated; to inform the instruments psychometric characteristics and factors affecting standard precautions knowledge.
Integrative review, whose descriptors and key words were selected in the databases LILACS, Pubmed (MEDLINE), ISI Web of Knowledge, Scopus and CINAHL databases. The final sample was 18 cross-sectional studies, being heterogeneous concerning places and sectors of achievement, and countries located in the different classifications of the Human Development Index (HDI). No one of the instruments contemplated all topics recommended and content validation was the largest worry of authors. The knowledge is below the recommended and the majority of workers do not understand the goals of standard precautions (SP). It is suggested the validation of existing instruments for which reliable results can be found.
Key words: Validation studies; Knowledge, Attitudes and Practice in Health; Personal Health.
RESUMO
Buscou-se identificar instrumentos para mensurar o conhecimento e informações dos profissionais de saúde sobre as precauções-padrão (PP); descrever o conhecimento e informações dos trabalhadores; verificar dimensões e conteúdos avaliados; informar as características psicométricas dos instrumentos e fatores impactantes no conhecimento.
Revisão integrativa, cujos descritores e palavras-chave foram selecionados nas bases de dados: Lilacs, Pubmed (Medline), Isi Web of Knowledge, Scopus e CINAHL. A amostra final foi de 18 estudos transversais, sendo heterogêneos quanto aos locais e setores de realização, e países situados nas diversas classificações de Indíce de Desenvolvimento Humano (IDH). Nenhum instrumento contemplou todos os tópicos preconizados e a validação de conteúdo foi a maior preocupaçãos dos autores. O conhecimento está abaixo do recomendado e a maioria dos trabalhadores não compreendem os objetivos das PP. Sugere-se a validação dos instrumentos existentes para que resultados fidedignos possam ser encontrados.
Palavras chave: Estudos de Validação; Conhecimentos, Atitudes e Prática em Saúde; Pessoal de Saúde.
RESUMEN
El objetivo fue identificar instrumentos para medir el conocimiento y la información de los profesionales de la salud acerca de las precauciones estándar (PE); describir estos conocimientos; verificar las dimensiones y contenidos valorados; informar sus características psicométricas y los factores que influyen en el conocimiento.
Revisión integral, cuyas palabras-clave fueran buscadas en base de datos Lilacs, Pubmed (Medline), ISI Web of Knowledge, Scopus y CINAHL. La muestra final fue 18 estudios transversales, heterogéneos en cuanto a los sitios y sectores de ejecución, así como los países situados en las diversas clasificaciones del Índice de Desarrollo Humano. Ningún instrumento incluyó todos los tópicos recomendados y la validación de contenido fue la mayor preocupación de los autores. El conocimiento está por debajo de lo recomendado y la mayoría no comprende los objetivos de las PE. Se sugiere la validación de los instrumentos existentes para obtenerse resultados confiables.
Palabras clave: Estudios de Validación; Conocimientos, Actitudes y Práctica en Salud; Personal de Salud.
Introduction
The biological risk is a discussed issue in recent decades and deserves attention due to serious problems that cause not only for the individual exposed to risk, but family, community and institutions(1).
According to the Centers for Disease Control and Prevention(2), with the advent of HIV transmission, universal precautions (UP) were formulated with the main objective of protecting the health professionals of exposure to Biological Material Potentially Contaminated (BMPC); however the UP lacked both as regards the biosecurity measures in the transmission of pathogens track patient-patient and health professional-patient. Thus, in 1996, were imposed Standard Precautions (SP), which relate to the combination of the main characteristics of the UP and insulation of tangible substances and is based on the principle that any blood, body fluids, secretions and excretions (except sweat), skin and mucous membranes may contain infectious agents transmissible and have the dual objective of protecting the health professional and the patient (3,4).
It is known that 57 health workers presented serum-conversion to the HIV virus in the United States, after occupational exposure to BMPC(5) and that 140 new cases of infection were reported among workers since 1981, which reported no other risk factors associated with exposure to HIV and whose historical reports were of occupational exposure to blood and other fluids tangible or laboratory material contaminated by viruses, being the most recent case of seroconversion dated in 2009(6). However, difficulties of records on the real number of workers who have acquired this infection of occupational form, mainly in developing countries like Brazil(7,8). In this way, in developing countries, the monitoring systems and control of work accidents (OA) with MPBC need to be improved, as well as the notification of the OA should be encouraged(7-9).
Infections associated to health establishments are also worrying when focus is the safety of the patient. Known worldwide as "Health care associated infections" (HCAI), are considered as the most frequent adverse effect and studied from hospitalization and the main public health problem in developed countries due to the morbidity, mortality, prolonged hospitalization and negative effects to the patient and to the economic well-being of the nation(10,11).
The estimated number of Health Care Associated Infections (HCAI) in the USA is of the order of 1.8 million a year(12,13) and mortality caused or associated with HCAI is estimated at 99,000 deaths annually, with variations related to the type of infection and subgroups of the population.
The problem is further aggravating factor in countries with lower levels of development. Study has identified that the rates of HCAI in neonatal units in developing countries were 3 to 20 times larger than in developed countries(14). Longitudinal study performed in Intensive Care Centers in the South and Southeast of Brazil indicate the HCAI were distributed as follows: 28% blood infections associated with the use of central venous catheter, 44.3% pneumonia associated with mechanical ventilation and 27.7% infection of the urinary tract associated with the use of catheter. The indexes of HCAI this Brazilian study were significantly higher than those found in North American studies(15).
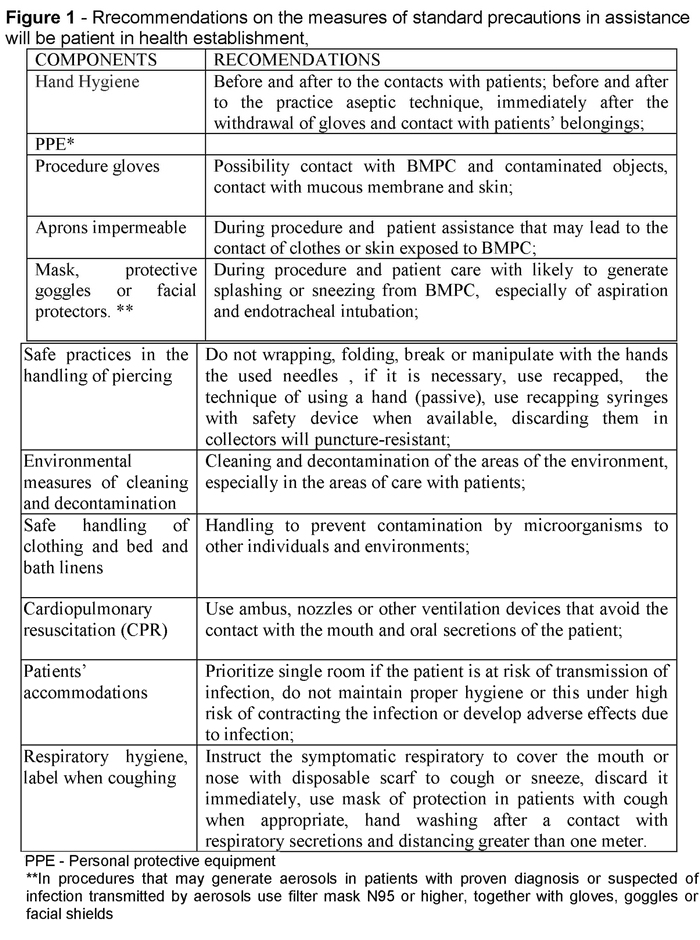
Investigations on the control of HCAI led the adoption of three new measures of SP: respiratory hygiene/label when coughing, safe practices for injection and use of protective masks for the insertion of catheters or lumbar puncture procedures, with the main objective of patient protection(4). The World Health Organization(16) still considers the disposal of solid waste of health institutions as an integral item of SP.
The SP currently recommended(4) are presented in figure 1.
The standard precautions (SP), known as well as universal precautions, when correctly applied, are the main strategy for protection of workers and to prevent the HCAI(3), but evidence of national and international literature give low adherence of professionals (serotype). The justification of the behavior of non-adherence encompasses many factors, among them, the related to the working environment -such as material, human resources and management commitment of the institution-and individual factors such as knowledge about the measures of SP and professional(17,21-23).
The personal factors that can influence the desired behavior of the professional include: self-efficacy; beliefs related to measures of SP and diseases; the knowledge on the SP and the attitudes in function of adherence to SP(24).In this way, studies have demonstrated that knowledge of workers is a factor impacting on the adherence to SP in establishments of health assistance(9,22,23).
The instruments of measures are used to identify the information that the professionals have assimilated relating to SP, because they show important results for the adoption of strategies for the prevention and control of exposure to BMPC. Studied individuals(25) show that the majority of the instruments applied with the purpose of verifying adherence of professionals to SP using selective elements and do not relate to all of the topics of the SP. Only a few studies provide explicit descriptions on the process of construction and validation of the instrument items, however most of the items that make up the instrument are not submitted, nor the psychometric characteristics of these, and the validity and reliability (26).
The knowledge, information, innovation and permanent education configure currently as the central themes of organizations(27). The information has been increasingly acknowledged as any other institutional feature, which needs to be managed to assist organizations improve their productivity, competitiveness and overall performance(28). Thus, the need for the creation of a conducive environment for the study and for the wide and healthy discussion concerning the use of information and knowledge in organizations is raised(27).
The impulse to the human being to seek information is the existence of a problem to be resolved, a goal to be reached and the observation of a lack in the knowledge related to a particular subject or condition(29). Knowledge can be understood as the significant links that people do in their heads between information and its applicability in action related to a given context, making explicit the direct connection between information and knowledge(30).
As regards the instruments to be presented, the authors refer that the same were constructed having as reference the international guidelines and references of the local organizations related to the description and use of SP measures. In this way, the topics of content of the instruments were classified as the topics of SP recommended by Seigel et al. (2007)(4) and the WHO)(4),presented in Figure 1.
The present study had as objectives to identify in national and international literature the instruments used to evaluate the knowledge and the information that the professionals of health establishments have on the SP, as well as describe what the knowledge of health workers about the theme; check which dimensions and content were evaluated in instruments; inform the psychometric characteristics of reliability and validity of instruments and the factors that exerted impact in knowledge.
Method
To achieve the goal established, it was realized an integrative review, which together with the systematic review, composes the methods of evidence-based Practice (EBP) and enables understanding of particular phenomenon through the knowledge already produced on the same(31).
As advocates Mendes(32), the following phases were followed to conduct the study: 1-establishment of research question; 2 - search strategy (establishments of inclusion and exclusion criteria, data base and selection of studies); 3 - categorization of studies (extraction, organization and data summarizing); 4 - Assessment of studies included in the review; 5 - Interpretation of the results and 6 - synthesis of knowledge.
The search was realized in LILACS, Pubmed (MEDLINE), ISI Web of Knowledge, Scopus and CINAHL databases, using the following descriptors and keywords: universal precautions; Standard Precautions, health personnel; knowledge; health knowledge, attitudes, practice and validity of tests.
The study inclusion criteria were: instruments of closed items to scale the knowledge of health establishments professionals to SP, with a quantitative approach, published in English, Spanish and Portuguese, in the period 1990 to March 2012 and with the abstracts available in the databases. The exclusion criterion was adopted to articles unavailable in full and the instruments that do not cover at least two aspects of SP measures.
The articles that fulfilled the inclusion criteria were identified, the data were extracted and information organized and classified in tables. The extracted information include the sample characteristics (location of study, professional category, age, gender, years of professional experience, working sector) and whenever possible, the level of knowledge of workers with respect to SP, as well as the items covered by the instruments and the psychometric characteristics of these (reliability, internal consistency and validity).
Once available, the factors impacting on knowledge to SP are reported. It is worth emphasizing that was performed a manual search of relevant references of selected articles in the sample.
Results
The crosses in the respective databases totaled 1,080 articles, being 345 in Medline, 11 in Lilacs, 450 in Cinhal, 171 in the Scopus and 103 in Isi Web of Knowledge. After the exclusion of duplicates, remaining 709 articles to be analyzed. Many articles were excluded based on reading the summaries, for not going to the meeting of the inclusion criteria. Some articles showed relevant summaries, but were excluded after reading. Large number of articles referring to the knowledge of the professionals on the HIV virus and other was of a qualitative approach, and therefore were excluded from the sample. Moreover, the majority do not used instruments with closed items, which made the final sample with18 articles included.
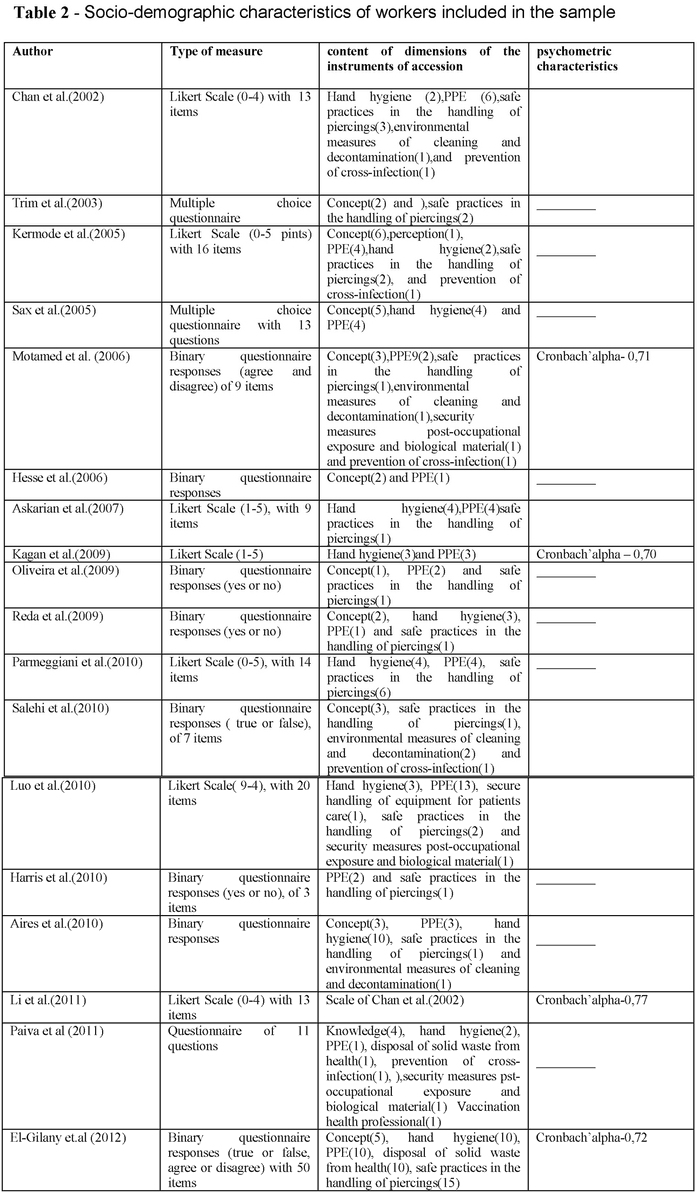
All the studies that compose the sample are transversal and no studies were found for the validation of instruments. No one of the instrument addressed all topics of accession SP referred to by the CDC (Seiegel, 2007) (4), being that the topics most commonly addressed: safe practices in the handling of piercing, use of PPE, hand hygiene and concept on the SP, followed of environmental measures of cleaning and disinfection and disposal of solid waste in health.
The measurement system and score adopted by the majority of the instruments were binary answers (yes/no, agree/disagree) and Likert scale (0-4 and 0-5 points), being that one article has used the multiple choice questionnaire. With the purpose of knowing the information of the professionals of health establishments on the SP, the authors have explored the validity of the content of instruments, by means of using available literature on the subject and by means of expert committees about the theme for the trial of the appearance instruments and relevance of the items. Some instruments have held the reliability by means of test-retest reliability and internal consistency was assessed by Cronbach's alpha.
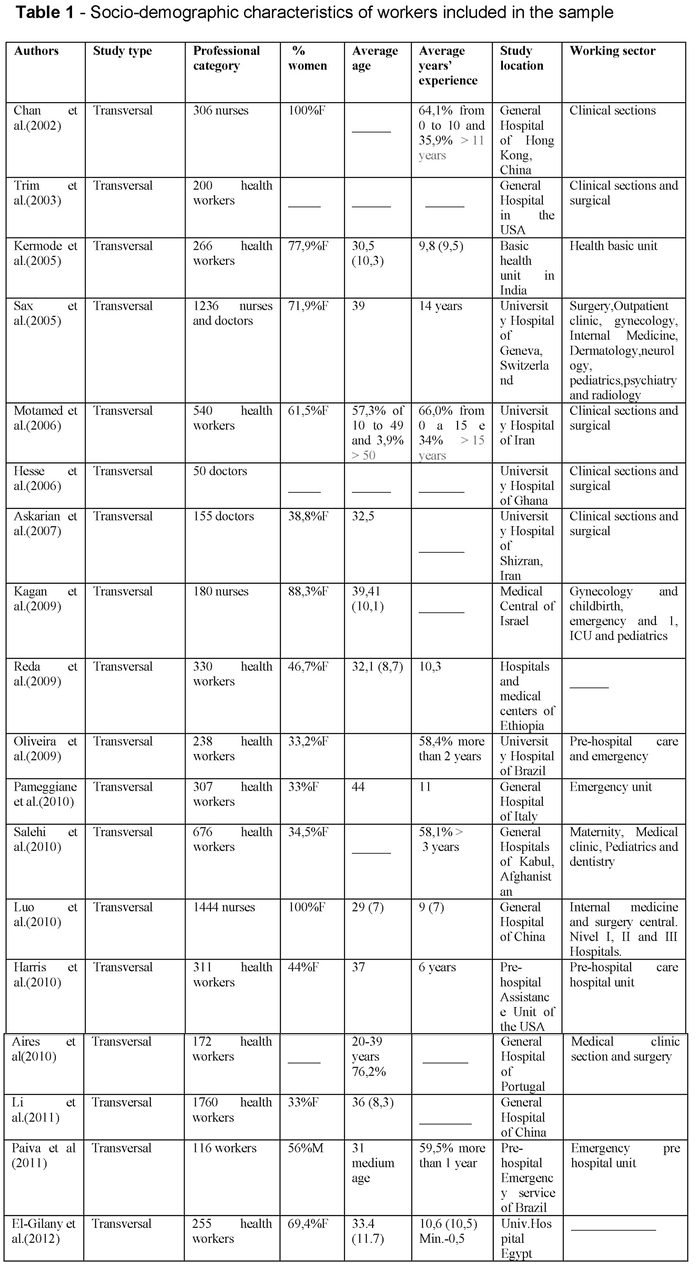
The Socio-demographic workers' characteristics included in the sample are shown in Table 1.
Discussion
1. Socio-demographic workers' characteristics: The sample is heterogeneous in relation to the places and sectors of study. Large part was held in clinical sectors, emergency and clinical-surgical of large hospitals. These sectors are characterized by high workload, higher risk of exposure to blood and greater realization of invasive procedures(4,33).
The sample countries have Human Development Index (HDI) distinct (34). The HDI refers to a composite value by the average of the measures reached in three promotes support: long and healthy life, knowledge and decent standard of living. The variables analyzed in order to obtain the HDI of a nation are: life expectancy at birth, average years frequented of studies, estimate of years of study and gross national income per captures(34). Very high HDI: United States of America, Switzerland, Italy and Israel; High HDI: Iran and Brazil; Medium HDI: Egypt, China, India and Ghana and HDI low: Afghanistan, Ghana and Ethiopia.
2. Content present in the instrument : none of the instruments contemplated all topics established by the CDC (Seigel et al. 2007)(3,4), as the measures of patient's accommodation, measures for the procedure of CPR and the hygiene measures respiratory/label when coughing.
It was evidenced that the authors build and use instruments with the inclusion of variables of greater interest to their reality. The inclusion of selective items related to knowledge of standard precautions (SP) is often more viable for the reality that if you want to investigate what the inclusion of all items recommended by the CDC (Seigel et al. 2007)(4), due to wide and extensive nature of SP. Waltz et al. (2010)(35)infer that the local context that if you want to investigate in a referred situation has important implications in the development of the topics of the instrument measures, as well as what will be done on the basis of the results obtained. However, it should be underscored the importance of the revision of the instruments over the years if the authors intend to apply it again in the same population or distinct populations, since the guidelines undergo changes over time, with the inclusion of new and important topics(3,4).
An example refers to the topic on the hygiene measures respiratory/label when coughing, included in 2007(4). This topic is essential in order to prevent the transmission of diseases of the respiratory tract, such as Severe Acute Respiratory Syndrome (SARS), and should be a topic considered in the tools of knowledge to SP, since the outbreak of SARS has had repercussions global socio-economic consequences (36).
Some instruments used topics not described in guidelines as specific recommendations of SP, the example of measures of the post-exposure to biological material and immunization (9, 37).
3. The instruments' psychometric characteristics: the purpose of the great majority of authors was the validation of the content of the instruments, having as reference the literature available on the measures of SP. As Pasquali (38) said, the theoretical definition is developed through the following a careful review of the literature, in which the essential elements on the meaning of the concept are delimited and logically organized.
The construct validation was not performed in any study that it is presented in the sample, being that this aims to establish sustenance to the capacity of the instrument has the function of measuring the construct with the purpose for which it is being used, so that the content validation, in isolation, does not ensure the validation of an instrument (35).
The internal consistency of the instrument by Cronbach Alpha and reliability through the test-retest reliability was verified in some studies (9,20,22,37,39-42).The internal consistency of an instrument refers to verifying the correlation (homogeneity) between the items of an instrument in the form of scale (sub-scale), as well as, if they are measuring the same construct.
The internal consistency is an important and appropriate for instruments that intend to measure a single construct through the use of multiple items and should vary around 0,70 to 0,95. However, it should be emphasized that the Alpha of Cronabach should not be performed in isolation when is the objective to validate an instrument, since this measure does not take into account possible variations that occurred in a period of time and is influenced by the number of items of the instrument (35).
The reliability by the test-retest is an important psychometric index to be considered because it is able to detect the measurement stability over a period of time estimated time and refers to the degree to which repeated measurements in stable persons provide similar responses, varying from 0 to 1(43). However, few were the instruments that presented the validation process of the same or its psychometric properties, fact that exerts direct impact in the veracity of the results and the generalization of data.
4. Information on the measures of standard precautions (SP): as shown in table 2, the correct information for workers on the SP is lower than the recommended procedure.
In some studies, the workers revealed to have correct information and knowledge regarding the disposal of needlestick(20,37,39), but in some studies the appropriate knowledge about this topic was not observed(22,44,45). Study realized in Iran(22) showed that the majority of doctors believe that the needles must be folded before disposal, which exposes them to risks of needlestick, being this type of exposure more frequently among health workers(7,8) and with greater risk of contamination to the HIV virus, HCV and HBC(5).
The information of workers regarding the use of PPE showed variable knowledge between the countries included in the sample. Some studies have revealed a greater knowledge(20,22,37,39,46-51) while other studies showed lower knowledge(45-46). Study realized in Switzerland(46) revealed that many workers (47%) do not have adequate information about the importance of the use of masks of protection when performing the physical examination in respiratory symptoms. Still with relation to the PPE, the study carried out in Brazil revealed that only 53% of drivers who work in emergency care units consider important the accession to the gloves procedure(45), which exposes them to unnecessary risks and greater exposure to BMPC(8).
The knowledge about the hand hygiene showed to be superior compared to the other items in the majority of studies(20,40,46,48,49). However, some findings showed that less than 75% of the doctors in Iran knew the importance of hand hygiene, before and after the use of procedure gloves and Paiva(45) showed that only 52% of drivers who work at the emergency unit in Brazil knew the importance of hand hygiene.
Study conducted in Portugal(50) revealed that 21% of professionals are unaware of alternative forms to washing their hands. Seigel et al. (2007) (4) said that hand hygiene has often been cited as the most important practical in the reduction of infectious agents in health establishments and incorporates an essential element of SP. The term "hand hygiene" includes both the washing of hands with soap simple or containing antiseptics and water as the use of products, the basis of alcohol which do not require the use of water. In the absence of visible dirt in the hands, these products are preferable to the use of soap simple or antimicrobials and water by its high microbiological activity, by the reduction of skin dryness and by convenience. The improvement of hand hygiene practices has been associated with a substantial reduction in the incidence of HCAI(4), whose results reveal the need for training and awareness of workers about the theme.
With respect to the basic concept of standard precautions (SP), that should be applied to all patients, regardless of the clinical diagnosis or suspect, was verified lack of knowledge , since the most informed was that the SP must be only applied in patients with positive HIV virus or viral hepatitis, or with clinical diagnosis or suspected of infection potentially transmissible. This lack of knowledge was present in countries with different HDI, from the highest and lowest places, such as Switzerland, India, the United Arab Emirates, Pakistan and Afghanistan(20,40,42,46,52).
This fact can bring serious consequences to workers and health institutions, seen that infections such as HIV may have long period between the contamination of the individual by the virus and the presence of characteristic symptoms of infection and the diagnostic confirmation, whose period on average is 10 years(53). Viral hepatitis also represent a serious risk and special attention should be directed to the risk of contamination by HCV, because there are currently no existing prophylaxis(54).
Many workers were not informed with the term "standard precautions"(9,20). Study realized in India(20) revealed that 88% related to SP as "nursing barriers". Accordingly, findings in the literature show that the professionals identified such measures as "use of PPE" and "human care"(55).
The findings show that the concept of double protection of SP, workers and the patients, is still not understood by many professionals, since there is a lack of the knowledge in relation to the concept of transmitting infections of professionals to patients(49,52), the example of HCAI(3,4). This deficiency of information is present in all classifications of countries by means of IDH.
Regarding the type of exposure to BMPC, was observed that many workers consider only the risk of an accident caused by a needlestick injury(46,51,56,57), since it did not consider the contamination by sneezing and fluids of BMPC in mucous membranes. It cannot be underestimated this type of exposure, since there are reports of seroconversion after this type of accident at work(58). Study realized in the USA(56) showed that only 21% knew the risk of contamination to the hepatitis B virus after percutaneous exposure; 30% for hepatitis C and 27% to the HIV virus. The great majority of workers underestimated the risk. Some workers consider the HIV virus infecting more that the HBV(45). It is known that in relation to HIV, the risk of occupational transmission is around 0.3 to 0.5% in percutaneous exposure, while for the hepatitis B virus risk may vary from 6 to 30%(5).
Regarding to the handling of piercing devices, the study of Salehi et al.(42) refers that 82% of workers believe that is allowed to carry out the recapping active. Findings in the literature showed that practices related to improper disposal of sharp material was responsible for a large proportion of accidents with exposure to BMPC in a city in the interior of São Paulo, Brazil, being that the manipulation of the pickup box, discard in common trash bag and the active recapping totaled 35.2 % of these accidents(7,8).
It can be noticed in the great majority of studies included is the stigma with regard to the care to be provided to HIV carriers. It was stated that procedure gloves must always be wore when the assistance to HIV seropositive patients(39,48). Added to this lack of knowledge, many professionals consider that these patients should be kept in isolation room(37,42). The lack of knowledge about the transmission of the disease and evolution cause even more preconception respect to the holder(59).
Still on this theme, some workers have said that as the routine of the establishments, all surgical patients should be tested for HIV(20,42,47), evidencing the need for training and education.
5. Variables of impact on adherence to SP: the titration was the variable that was associated with more frequency to knowledge, positively, as shows the study of MotamedOliveira(37), Harris(44) and El-Gilany(51).
The presence of training was associated positively in two studies(41,46), as well as the desire to receive training on the measures of SP by workers(22,48).
The age range of 20 to 30 years showed with more knowledge in the study of Motamed(37) and the professionals with 50 years or more are related negatively to knowledge(37,41), as well as those who work more time in the institution(40).
The knowledge about the need for hand hygiene was positively associated with the knowledge of the SP in the study of Parmeggiane(49) and the knowledge on the SP was related positively to the adherence in some studies, being that in only a research was so strong(22) and a moderate association(37).
It is worth emphasizing, however, that although the objective of the majority of the authors was to validate the topics of knowledge on the SP, the presence of variables that impact on knowledge reported by different studies analyzed also reveal evidence of convergent and divergent validation.
Some limitations must be reported. The knowledge on the SP as well as the impact of variables impact evidenced were analyzed on the basis of the articles selected to compose the sample, which may mean that this sample is not completely representative of reality, since studies that relate such variables may have been excluded taking as reference the inclusion criteria of pre-established.
Conclusion
It is suggested the validation of the instruments used to obtain reliable results, since few studies have reported the validation process of the instruments used on knowledge related to standard precautions. With relation to validation of instruments is important to emphasize that important psychometric characteristics - as the construct validity convergent divergent - are not/present in instruments included.
The findings showed incorrect information and inadequate workers about the measures standard precautions. The basic principle of standard precautions is not understood worldwide by workers included in the studied sample. In this way, the permanent education related to the theme of standard precautions is essential for the concepts that are understood and seized and managers, workers, users and higher education institutions should work together for an accession to these important measures of protection. It is essential that the agencies of global health awareness about the reality in order to plan and propose actions with views to the knowledge and accession to standard precautions. It is emphasized the need for future research in order to evaluate the level of knowledge and the variables predictive for the knowledge of the SP through the application of instruments previously validated in more representative samples and less selective of workers.
Received: March 18, 2015
Accepted: 12 June 2015
References
1. Soerensen AA. Acidentes ocupacionais com ênfase ao risco biológico em profissionais do atendimento pré-hospitalar (tese). Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo; 2008. [ Links ]
2. Centers for Disease Control and Prevention. Recommendations for preventing transmission of infection with human T-lymphotropic virus type III/lymphadenopathy-associated virus in the workplace. MMWR 1985;34(45):681-686;691-695. Avaiable from: http://www.cdc.gov/mmwr/preview/mmwrhtml/00033093.htm. [ Links ]
3. Garner JS. Guideline for isolation precautions in hospitals. The Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1996;17(1):53-80. [ Links ]
4. Siegel JD, Rhinehart E, Jackson M, Chiarello L. Guideline for isolation precautions:preventing transmission of infectious agents in healthcare settings. Atlanta; 2007 (cited 2012 Jan. 1). Avaiable from: http://www.cdc.gov/ncidod/dhqp/pdf/guidelines/isolation2007.pdf. [ Links ]
5. Centers for Disease Control and Prevention. Surveillance of healthcare workers with AIDS, as of December 2002. Atlanta; 2003. (cited: 2012 Apr. 8). Avaiable from: www.cdc.gov/ncidod/dhqp/bp_hiv_hp_withh.html. [ Links ]
6. Centers for Disease Control and Prevention. Department of Health and Human Services - USA. Surveillance of Occupationally Acquired HIV/AIDS in Healthcare Personnel, as of December 2010. Atlanta; 2010. (cited: 2012 Jul. 26). Avaiable from: http://www.cdc.gov/HAI/organisms/hiv/SurveillanceOccupationally-Acquired-HIV-AIDS.html. [ Links ]
7. Valim MD, Marziale MHP. Avaliação da exposição ocupacional a material biológico em serviços de saúde. Texto Contexto Enferm. (online). 2011;20(Esp):138-46. Available from: http://www.scielo.br/scielo.php?script=sci arttext&pid=S010407072011000500018&lng=enhttp://dx.doi.org/10.1590/S010407072011000500018. [ Links ]
8. Valim MD, Marziale MHP. Notificações de acidentes do trabalho com exposição a material biológico: estudo transversal. Online Braz J Nursing. (online). 2012;11(1):51-64. Avaiable from: http://www.objnursing.uff.br/index.php/nursing/article/view/3537/html_1. [ Links ]
9. Luo Y, He GP, Zhou JW, Luo Y. Factors impacting compliance with standard precautions in nursing, China. Int J Infect Dis. 2010;14:1006-14. [ Links ]
10. Jarvis WR. Selected aspects of the socioeconomic impact of nosocomial infectious: morbidity, mortality, cost and prevention. Infect Control Hosp Epidemiol. 1996;17(8):552-57. [ Links ]
11. Burke JP. Infection control e a problem for patient safety. N Engl J Med. 2003;348:651-56. [ Links ]
12. Weinstein RA. Nosocomial infection update. Emerg Infect Dis. 1998;4: 416-20. [ Links ]
13. Klevens RM, Edwards CL, Richards CL, Horan TC, Gayners RP, Pollock DA, et al. Estimating health care-associated infections and death in U.S hospitals, 2002. Public Health Rep. 2007;4(6):160-66. [ Links ]
14. Zaidi AKM, Huskins WC, Thaver D, Bhutta ZA, Abbas Z, Goldmann DA. Hospital-acquired neonatal infections in developing countries. Lancet. 2005;365(26):1175-88. [ Links ]
15. Salomao R, Rosenthal VD, Grimberg G, Nouer S, Blecher S, Buchner-Ferreira S, et al. Device-associated infection rates in intensive care units of Brazilian hospitals: finding of the International Nosocomial Infection Consortium. Rev Panam de Salud Publica. 2008;24:195-202. [ Links ]
16. World Health Organization. Practical Guidelines for Infection Control in Health Care Facilities. WPRO Regional Publication. Manila; 2007. (cited: 2010 Jan. 10). Available from: http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf. [ Links ]
17. Brevidelli MM, Cianciarullo TI. Fatores psicossociais e organizacionais na adesão às precauções-padrão. Rev Saúde Pública. 2009;43(6): 907-16. [ Links ]
18. Gershon RRM, Karkashian CD, Vlahov D, Kummer L, Kasting C, Green-McKenzie J, et al. Compliance with universal precautions in correctional health care facilities. J Occup Environ Med. 1999; 41:181-89. [ Links ]
19. Janjua NZ, Rezaq M, Chandir S, Rozi S, Mahmood B. Poor knowledge-predictor of nonadherence to universal precautions for blood borne pathogens at first level care facilities in Pakistan. BMC Infect Dis. 2007; 7:1-11. [ Links ]
20. Kermode M, Jolley D, Langkhan B, Thomas MS, Holmes W, Gifford SM. Compliance with universal/standard precautions among health care workers in rural north India. Am J Infect Control. 2005; 33:27-33. [ Links ]
21. Gershon RRM, Vlahov D, Felknor AS, Vesley D, Johnson PC, Delcios GL, et al. Compliance with universal precautions among health care workers at three regional hospitals. Am J Infect Control. 1995;23(4):225-36. [ Links ]
22. Askarian M, Mclaws ML, Meylan M. Knowledge, attitude, and practices related to standard precautions of surgeons and physicians in university-affiliated hospitals of Shiraz, Iran. Int J Infect Dis. 2007;11(1):213-19. [ Links ]
23. Efstathiou G, Papastravou E, Raftopoulos V, Merkouris A. Factors influencing nurses' compliance with Standard Precautions in order to avoid occupational exposure to microorganisms: A focus group study. BMC Nursing. 2011; 10: 1-12. [ Links ]
24. Mahat G, Eller LS. HIV/AIDS and universal precautions: knowledge and attitudes of Nepalese nursing students. J Adv Nurs. 2009;65(9):1907-15. [ Links ]
25. Gammon J, Morgan-Samuel H, Gould D. A review of the evidence for suboptimal compliance of healthcare practitioners to standard/universal infection control precautions. J Clin Nurs. 2007;17(2):157-62. [ Links ]
26. Lam SC. Universal to standard precautions in disease prevention: preliminary development of compliance scale for clinical nursing. Int J Nurs Stud. 2011;48(12):1533-39. [ Links ]
27. Neto RCD de A. Gestão de informação e do conhecimento nas organizações: análise de casos relatados em organizações públicas e privadas (dissertação). Belo Horizonte: Escola de Ciência da Informação, Universidade Federal de Minas Gerais; 2002. [ Links ]
28. Bergeron, P. Information Resources Management. Anual Review of Information Science and Terminology.1996; 31(1):263-300. [ Links ]
29. Coadic YF. A ciência da informação. Brasília: Briquet de Lemos; 1994.2.ed.124p. [ Links ]
30. Dixon NM. Common Knowledge: how companies thrive by sharing what theyknow. Boston: Harvard Business Press; 2000. 1.ed. 188 p. [ Links ]
31. Broome ME. Integrative literature reviews for the development of concepts. In: Rodgers BL, Knafl KA, editors. Concept development in nursing: foundations, techniques and applications. Philadelphia: W.B Saunders Company; 2000. p.231-50. [ Links ]
32. Mendes KS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Contexto Enferm. 2008;17(4):758-64. [ Links ]
33. Brevidelli MM, Cianciarullo TI. Compliance with standard-precautions among medical and nursing staff at a university hospital. Online Braz J Nursing. (online). 2006;5(1):1-9. Avaiable from: http://www.uff.br/objnursing/index.php/nursing/article/view/291. [ Links ]
34. United Nations Development. Human development report 2011: human development statistical annex. New York; 2011. (cited 2012 Feb. 25). Avaiable from: http://hdr.undp.org/en/media/HDR_2011_EN_Tables.pdf. [ Links ]
35. Waltz C, Strickland OL, Lenz ER. Measurement in nursing research. New York: Springer; 2010. 4o ed. 504p. [ Links ]
36. Sung JJ, Wu A, Joynt GM, Yuen KY, Lee N, Chan PK, et al. Severe acute respiratory syndrome: report of treatment and outcome after a major outbreak. Thorax. 2004;59:414-20. [ Links ]
37. Motamed N, Babamahmood A, Khalilian M, Peykanheirati M, Mozari M. Knowledge and practices of health care workers and medical students towards universal precaution in hospitals in Mazandaran province. East Mediterr Health J. 2006;12(5):653-60. [ Links ]
38. Pasquali L. Testes referentes a construto: teoria e modelo de construção. In: Pasquali L., et al. Instrumentação Psicológica: fundamentos e práticas. Porto Alegre: Artmed; 2010, 560 p. [ Links ]
39. Chan R, Alexander M, Chan E, Chan V, Ho B, Lai C. Nurses' knowledge of and compliance with universal precautions in an acute care hospital. Int J Nurs Stud. 2002;39(2):157-63. [ Links ]
40. Kagan I, Ovadia KL, Kaneti T. Perceveid knowledge of blood-borne pathogens and avoidance of contact with infected patients. J Nurs Scholarship. 2009;41(1):13-19. [ Links ]
41. Li L, Chunqing L, Zunyou W, Jihui G, Manhong JIA, Zhihua Y. HIV-related avoidance and universal precaution in medical settings: opportunities to intervene. Health Serv Res. 2011;46(2):617-631. [ Links ]
42. Salehi AS, Garner P. Occupatinal injury history and universal precautions awareness: a survey in Kabul hospital staff. BMC Infect Dis. 2010;10(19):1-4. [ Links ]
43. Terwee CB, Bot SDM, de Boer MR, van der Windt DA, Konl DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34-42. [ Links ]
44. Harris SA, Nicolai NA. Occupational exposures in emergency medical service providers and knowledge of and compliance with universal precautions. Am J Infect Control. 2010;38(2):86-94. [ Links ]
45. Paiva MHRS, Oliveira AC. Conhecimento e atitudes de trabalhadores de um serviço público de emergência sobre adoção de precauções padrão. Rev Bras Enferm. 2011;64(4):704-710. [ Links ]
46. Sax H, Perneger T, Hogonnet S, Herrault P, Chraiti MN, Pittet D. Knowledge of standard and isolation precaution in a large teaching hospital. Infec Control Hosp Epidemiol. 2005;26 (3):298-304. [ Links ]
47. Hesse AAJ, Adu-Aryee NA, Entsua-Mensah K, Wu L. Knowledge, attitude and practice universal basic precautions by medical personnel in a teaching hospital. Ghana Med J. 2006;40(2):61-64. [ Links ]
48. Reda AA, Vandeweerd JM, Syre TR, Egata G. HIV/AIDS and exposure of healhcare workers to body fluids in Ethiopia: attitudes toward universal precautions. J Hosp Infect. 2009;71(2):163-69. [ Links ]
49. Parmeggiani C, Abbate R, Marinelli P, Angelillo IF. Healthcare workers and health care-associated infections: knowledge, attitudes, and behavior in emergency departments in Italy. BMC Infect Dis. 2010;10(35): 1-9. [ Links ]
50. Aires S, Carvalho C, Aires E, Calado E, Aragão I, Oliveira J, et al. Avaliação dos conhecimentos e atitudes sobre precauções padrão: Controlo de Infecção dos Profissionais de Saúde de um Hospital Central e Universitário Português. Acta Med Port 2010;23(2):191-202. [ Links ]
51. El-Gilany AH, Badawy K, Sarraf B. Knowledge of health care providers os standard precautions and infection controla t students'hospital, Mansoura University, Egypt. TAF prev Med Bull. 2012;11(1):1-6. [ Links ]
52. Sreedharan J, Muttappillymyalil J, Venkatramana M. Knowledge about standard precaution among university hospital nurses in the United Arab Emirates. East Mediterr Health J. 2011;17(4):331 -34. [ Links ]
53. González LO, Valdez LLS, Corcho DB, González AG, Ávila JLP, Lantero MI. Debut clínico del SIDA en Cuba. Rev Cubana Med Trop. 2007;59(2):127-33. [ Links ]
54. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Exposição a materiais biológicos. Brasília; 2006. [ Links ]
55. Melo DS, Souza ACS, Tiplle AFV, Neves ZCP, Pereira MZ. Nurses' understanding of standard precautions at a public hospital in Goiania-GO, Brazil. Rev Lat Am Enfermagem. 2006;14(5):720-27. [ Links ]
56. Trim JC, Adams D, Elliot TSJ. Healthcare workers' knowledge of inoculation injuries and glove use. Br J Nurs. 2003;12(4): 215-21. [ Links ]
57. Oliveira AC, Cardoso CS, Mascarenhas D. Intensive care unit preofessionals' knowledge and behaviour related to the adoption of contact precautions. Rev Lat Am Enfermagem. 2009;17(5): 625-31. [ Links ]
58. Centers for Disease Control and Prevention. Workbook for Designing, Implementing and Evaluating a Sharp Injury Prevention Program. Atlanta; 2008. (cited: 2010 Jun. 5). Available from: www.cdc.gov/sharpssafety/. [ Links ]
59. Velandia MA. Manual de consejeria pré y posprueba en VIH y sida. In: Programa de sida. Ministerio de Salud. Bogotá: Fundación APOYÉMONOS; 2002, 122p. [ Links ]

