










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkInternational adoption of children who spent their early years in orphanages or institutions has been widespread in Europe and North America in the last 30 years (Selman, 2012). Notwithstanding its challenges, international adoption has been broadly successful in providing a stimulating and nurturing family environment for children with early adversity, resulting in an impressive catch-up across most developmental domains (Palacios et al., 2019; van IJzendoorn & Juffer, 2006). Nevertheless, long-term developmental consequences of early adversity are expected. Emotional or internalizing problems, like depression or anxiety, have been one of the areas of attention, as attachment theory posits that the absence of a stable and committed caregiver early in life is a risk factor for the later development of depression and anxiety, among other risks (Bowlby, 1973; Zahn-Waxler et al., 2000).
However, both the meta-analysis by Juffer and van Ijzendoorn (2005) and the most recent one by Askeland et al. (2017) showed that intercountry adopted children do not show more internalizing problems than community children. This meta-analytical finding has been discussed and explored in more detail. Evidence from several research studies with internationally adopted children suggests a more complex picture by showing that a) later-adopted children (as indexed, in general, by age at adoption higher than 18 or 24 months) do show higher rates of internalizing problems than community controls (Gunnar et al., 2007; Hawk & McCall, 2010); b) whereas children from some areas of origin like Asia tend to show relatively good adjustment, children adopted from Eastern Europe/Russia generally show more difficulties, including internalizing problems (Gunnar et al., 2007), and c) internationally adopted children (or placed in foster care) who had been institutionalized show more internalizing problems than community controls (Humphreys et al., 2015), whereas internationally adopted children without institutional experience, do not (Wiik et al., 2011). Furthermore, the meta-analyses on this subject have also shown that differences in mental health between adopted and community youth were larger when using categorical rather than dimensional scores of emotional and behavioral symptoms, that is, when comparing the proportion of youth in the clinical range of problem behaviors (Askeland et al., 2017).
Moreover, some aspects regarding the developmental pathway to internalizing symptoms were not present in the meta-analyses. Cross-sectional evidence showing a late onset of emotional problems among internationally adopted individuals (Vegt et al., 2009) has been confirmed by longitudinal studies. In the English and Romanian Adoptees Study (ERA), there was no evidence at age six of elevated rates of emotional problems among children adopted from severely depriving institutions. However, in early adolescence, it was evident an increase in internalizing problems, both at a dimensional and a categorical level (Colvert et al., 2008). These emotional disturbances were further exacerbated in the transition to adulthood (Sonuga-Barke et al., 2017).
Researchers from the ERA study interpreted their findings as reflecting a developmental cascade from the social and educational difficulties associated with early adversity-related neurodevelopmental problems (Golm et al., 2020). This hypothesis is further supported by the well-established co-morbidity between ADHD and depression (Biederman et al., 1998), considering that ADHD-like symptoms are one of the most frequent and persistent consequences of early adversity in general and of institutionalization in particular (Sonuga-Barke et al., 2017). Furthermore, fetal alcohol spectrum disorder (FASD), which seems to be present at a high rate among adoptees from Eastern Europe (Popova et al., 2023) is related to internalizing problems (Chudley et al., 2005). Neuroanatomical deficits (as manifested, for example, by severe deficits in head circumference), ADHD, and FASD are indicators of severe neurodevelopmental problems as a consequence of prenatal or post-natal adverse experiences that are common among internationally adopted children from Eastern Europe (Miller et al., 2009).
Research has also documented that other post-adoption factors could be associated with the development of internalizing difficulties and adjustment difficulties. This could be the case with adoption communication: adopters’ active and empathic attitude towards adoption communication facilitates dialogue and exploration of adoption-related issues and expression of emotions (Brodzinsky, 2006; Thomas & Scharp, 2020). A high degree of openness in adoption communication helps adopted individuals to make sense of their adoption and adoption-related losses and encourages the child to initiate adoption conversations, helping to diminish preoccupation with adoption (Brodzinsky, 2006; Horstman et al., 2016). Although research evidence is not abundant, some studies have related communication openness with higher self-esteem and lower adjustment problems (Aramburu et al., 2020; Brodzinsky, 2006; Grotevant et al., 2011).
An additional post-adoption challenge for internationally adopted adolescents is the possible discrimination experiences they may suffer due to their adoption status and racial/ethnic minority group membership (Ferrari et al., 2017; Lee, 2010). Perceived discrimination experiences can take the form of microaggressions, including comments or experiences of rejection or exclusion due to ethnic or adoptive status (Baden, 2016), and they may have negative consequences on mental health -particularly on depression, anxiety, and negative affect-, especially among adolescents (Schmitt et al., 2014; Williams et al., 2003). Several studies have found a relationship between perceived discrimination and well-being among intercountry adopted individuals, including self-esteem (Ferrari et al., 2017), depression (Arnold et al., 2016), or psychological distress and sleep disturbances (Koskinen et al., 2015).
A relevant methodological aspect to consider when assessing internalizing problems in adopted adolescents is the role of the informant. Regarding the magnitude of agreement, a low to moderate agreement between parent and self-report of adolescent’s psychosocial adjustment is a solid finding in the literature (De los Reyes & Kazdin, 2005; Rescorla et al., 2013). Regarding the direction of discrepancies, a higher level of mental health problems is detected when using self-reports rather than parent reports in community adolescents across cultures, both for internalizing and externalizing problems (Rescorla et al., 2013).
In adoptive dyads, however, it has been proposed that the magnitude and direction of parent-adolescent informant discrepancies could be different, with parent reports on mental health showing greater scores than self-reports. Meta-analytical evidence has shown that the differences between adopted and nonadopted youth are larger when parent reports instead of self-reports are used (Askeland et al., 2017). It has been proposed that this result could reflect two potential biases specific to the adopted population: an over-concern and a lower threshold of adoptive parents regarding the mental health problems of their adopted children (Juffer & van IJzendoorn, 2005; Miller et al., 2000), or a diminished perception and report of their problems by adopted adolescents, because of their exposure to early life adversity (Roskam et al., 2017).
This pattern of parent-adolescent informant discrepancy has been found in some studies with clinically referred adolescents for emotional and behavioral problems (e.g., Ferdinand et al., 2006), although the literature is rather inconsistent (Rescorla et al., 2017). A relatively recent international study of cross-informant agreement in clinically referred populations found overall better parent-adolescent agreement in clinically referred than in community samples for some metrics, to the extent that there were no substantial differences between parent and self-reports in several samples of clinically referred adolescents (Rescorla et al., 2017).
To shed light on this issue, the cross-national study of Roskam et al. (2017) analyzed whether there was a specific pattern of informant discrepancies for mental health problems among adoptive adolescent-parent dyads in a sample of 294 participants from six (mainly European) countries. They found no adoptive status effect, with both adopted and community adolescents reporting more mental health -both internalizing and externalizing- problems than their parents. Neither the direction nor the magnitude of the cross-informant agreement differed between the adopted and community group (Roskam et al., 2017). Recent studies analyzing internalizing problems in adolescents adopted domestically in the US or in late internationally adopted adolescents in Italy have found a similar pattern of results (more problems in self- versus parent report; Muzi & Pace, 2023; Wright et al., 2022), calling into question the hypothesized adoptive status effect on the direction of cross-informant discrepancy in adopted populations.
However, the study by Roskam et al. (2017) included a mix of domestic and international adoptions from as many as 16 countries of origin. As mentioned before, previous findings have indicated the more complex emotional and behavioral profile of adopted youth from Eastern Europe as compared with other areas of origin (Gunnar et al., 2007), which could imply a pattern of cross-informant agreement more similar to clinically referred than to community adolescents.
All the above points considered, the present study has three aims: 1) to compare internalizing problems between adolescents adopted from Eastern Europe and low-risk community adolescents, using both a dimensional and a categorical approach, as recommended by Kessler (2002), and both parent and self-report; 2) To compare the magnitude of the cross-informant agreement between parent and self-reports in internalizing problems and the direction of potential discrepancies between the adopted and the community group, and 3) to examine factors predicting internalizing problems within the adopted group, including age at adoption, adversity-related neurodevelopmental problems, and post-adoption processes (adoption communication openness and perceived discrimination).
Given that our sample was comprised of adolescents adopted from Eastern Europe beyond the infancy years, for Aim 1 we expected that the adopted adolescents would show more internalizing problems than the community group, both at a dimensional and a categorical level, but more saliently at a categorical level, and both using parent and self-reports. Regarding Aim 2, on the magnitude of informant agreement, we hypothesized a low to moderate agreement between informants in both groups. On the direction of discrepancies, we hypothesized higher internalizing problem scores with self-reports than with parent reports in both groups, based on the most recent and relevant findings on adopted populations (Muzi & Pace, 2023; Roskam et al., 2017; Wright et al., 2022). For Aim 3, we expected late adoption, adversity-related neurodevelopmental problems, and perceived discrimination to predict higher internalizing problems among adopted adolescents. We expected adoption communication openness to predict lower internalizing problems, for both parent and self-reported internalizing problems.
Method
Participants
The sample was comprised of 99 Spanish adolescents between 12 and 18 years old. Sixty-nine were intercountry adopted adolescents (M age = 15.82 years, SD = 1.35) and 30 were community adolescents living with their birth families (M age = 16.11 years, SD = 1.12) and without known exposure to severe early adversity. All adopted adolescents were born in Russia. Age at adoption ranged from nine to 61.50 months (M = 32.91, SD = 14.96) and most adopted adolescents (n = 59, 85.5%) had pre-adoption institutional experience for an average of 33.14 months (SD = 15.12). At assessment, they had been a mean of 13.06 years (SD = 1.25) with their adoptive families. Three adopted adolescents were excluded from the sample analyzed here due to missing information on relevant variables, resulting in a final group of 66 adoptees. Table 1 displays descriptive demographic information for the adoptive (n = 66) and the community (n = 30) groups, both for the children and for the caregivers responding to the parent-report measures. There was a gender imbalance in the adoptive group (more proportion of boys) that is typical in adoptions from Russia (AIPAME, 2013).
Table 1. Descriptive Demographic Information for the Internationally Adopted and the Community Group.
| Sample characteristics | Adopted | Community |
|---|---|---|
| n (%) | n (%) | |
| Adolescents’ demographics | ||
| Female gender | 15 (37.9) | 17 (56.7) |
| Male gender | 41 (62.1) | 13 (43.3) |
| Caregivers’a demographics | ||
| Female gender | 57 (86.36) | 30 (100) |
| Male gender | 9 (13.64) | 0 (0) |
| Higher education level | 44 (66.66) | 16 (53.3) |
| Family structure | ||
| Bi-parental | 49 (74.2) | 26 (86.7) |
| Single mother/father | 17 (25.8) | 4 (13.3) |
Note. aDemographics are provided for the caregiver who completed the questionnaire
Instruments
Internalizing Problems
The parent- and self-reported versions of the Strengths and Difficulties Questionnaire (Goodman, 1997) were used to assess internalizing problems. This questionnaire was originally designed with five subscales covering the most common emotional and behavioral problems in childhood and adolescence (from four to 18 years). It has been validated in Spain (Ortuño-Sierra et al., 2015). Factor analysis as well as convergent and discriminant validity across informants and clinical disorders have shown that it is possible to derive broader internalizing and externalizing scales (Goodman et al., 2010). The internalizing scale includes 10 items on a 3-point scale (from 0 = not true to 2 = certainly true) covering manifestations of anxiety, depression, social withdrawal, or loneliness (e.g., “Often unhappy, down-earthed or tearful”, “Rather solitary, tends to play alone”). Following the authors’ guidelines, scores of 9 or higher were considered in the clinical range for internalizing symptoms. Internal reliability was satisfactory both for the parent-reported (Cronbach’s α = .73) and for the self-reported internalizing scale (Cronbach’s α = .71).
Adversity-Related Neurodevelopmental Problems
We constructed a summary index of common adversity-related neurodevelopmental problems among post-institutionalized children from three categorical indicators: ADHD diagnosis (n = 27, 40.9%), FASD diagnosis or confirmed prenatal alcohol exposure (n = 13, 19.7%; both reported by the adoptive parent) and deficit in neuroanatomy or head circumference (n = 22, 33.33%), as a broad indicator of brain growth. Following standard guidelines, a deficit in neuroanatomy or head circumference was considered by a standardized orbitofrontal head circumference score two standard deviations below the mean (z score < 2.0; Chudley et al., 2005). Orbitofrontal circumference was measured by the researchers during the data collection home visits and standardized scores were obtained from Spanish pediatric norms (Guerrero-Fernandez, 2020). Adolescents were assigned a score of 1 in each index if they presented the condition. Given that the three conditions tend to be co-morbid, and following previous research (Gunnar et al., 2007), we constructed a summary or cumulative index rather than including them as individual variables and artificially controlling statistically for one another.
Post-Adoption Processes
Adoption Communication Openness. The Adoption Communication Openness Scale (Brodzinsky, 2006) was used to measure this construct. This self-reported scale was answered by the adopted adolescents. It includes 14 items on a 5-point scale (1 = Strongly in disagreement to 5 = Strongly in agreement) covering different aspects related to the adolescent’s perception of their parents being open to discussing adoption-related issues and empathic and sensitive towards the adolescents’ feelings about adoption (e.g., “My mother/father is a good listener when it comes to my thoughts and feelings about being adopted.”). The 14 items load on one factor of adoption communication openness. We used the scores of the adolescents’ report on the identified main caregiver (see Procedure). The scale showed excellent internal consistency (Cronbach’s α = .89).
Perceived Discrimination. The Perceived Discrimination Scale (Lee et al., 2015) was used to measure this construct. It includes five items on a 4-point scale (from 1 = never to 4 = often) adapted to measure perceived experiences of discrimination related both to adoptive status and to ethnic minority membership (e.g., “I have been excluded or rejected by others because of my ethnicity/race”). Cronbach’s α was .72.
Procedure
The adoptive families were recruited through the collaboration of agencies and institutions responsible for international adoptions in Spain. They received a letter with information about the study and contact details. Families were part of the longitudinal LAIS. US study in Spain and had participated in previous data collections (see deleted for anonymous review for more details) (Cáceres et al., 2021). The community families were recruited through flyers in schools in varied socio-economic level areas from the same city where most of the adoptive families lived. Data collection was conducted from 2016 to 2018 (before the Covid-19 pandemic).
The families who participated received home visits in which the researchers explained the aims of the study and provided informed consent forms both to the main caregiver (identified as the caregiver whom the adolescent states to be closer with, most frequently the mother) and to the adolescent, and administered the measures and questionnaires. Adolescents answered the questionnaires by themselves without parental presence. The study was approved by the regional Ethics in Biomedical Research committee following international regulations on biomedical research with human subjects.
Data Analysis
For our first aim of comparing both parent-reported and self-reported internalizing problems between internationally adopted and community adolescents, we conducted independent samples t tests for the dimensional scores and chi-square tests for categorical scores, including Cramer V as effect size. For our second aim of analyzing cross-informant discrepancies in internalizing problems among both groups, when comparing parent- and self-reports in each group we used paired-sample t tests and when comparing discrepancy scores in each group, independent samples t tests. Following de los Reyes and Kazdin’s (2005) guidelines for the analysis of cross-informant discrepancies, we calculated cross-informant discrepancy scores by subtracting the standardized self-report scores from the standardized parent-report scores. We also run bivariate correlations between parent- and self-report scores to facilitate comparison with previous studies. Fisher r-to-z transformations were used to calculate a z-value for assessing the difference between two correlation coefficients from independent samples.
For our third aim of analyzing potential predictors of internalizing problems, analyses were run only with the adopted group. We first tested potential differences by age at adoption comparing mean internalizing problem scores between adolescents adopted earlier than 24 months and those adopted at 24 months or later using an independent sample t test. We then conducted multiple linear regression analyses for each informant’s internalizing problems score, including as predictors relevant covariates, adversity-related variables or post-adoption processes. The selection of predictors in the models followed both theoretical (e.g., we included gender as a covariate given the established gender differences in internalizing problems; Zahn-Waxler et al., 2000) and data-driven reasons. The assumptions of the multiple linear regression models were met following the inspection of appropriate parameters and graphs.
Cohen d was used as an effect size measure in all the means comparisons, and bootstrapped bias-corrected accelerated 95% confidence intervals based on 2000 samples were reported in all analyses. Both the parent-reported and the self-reported internalizing problems variables were positively skewed. We log-10 transformed both variables and re-run all analyses. Given that statistical conclusions did not change, the results were reported using not log-transformed variables for better interpretation of the statistical data and results (Changyong et al., 2014).
Results
Internalizing Problems in Internationally Adopted and Community Adolescents
We first conducted preliminary analyses comparing the adoptive and community groups in the main sociodemographic variables, including caregiver educational level, adolescent age at assessment, and gender. The groups did not differ on these variables. Table 2 displays descriptive data and the results of the t test for means comparison for parent- and self-reported internalizing problems in both groups. The internationally adopted adolescents showed higher internalizing problems than the community adolescents as reported by the main caregiver, with a large effect size (Cohen, 1988), but not higher self-reported internalizing problems. Figure 1 shows the parent- and self-reported internalizing problems means in both groups.
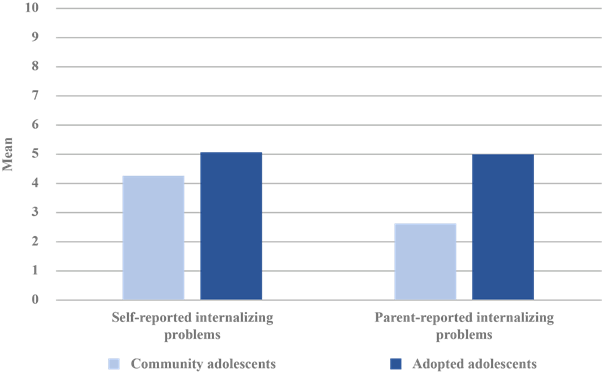
Figure 1. Self-Reported and Parent-Reported Internalizing Problems Means in Internationally Adopted and Community Adolescents.
Likewise, there were no statistically significant differences between the two groups in the proportion of adolescents with scores in the abnormal or clinical range of self-reported internalizing problems in each group (see Table 2; χ² [1] = 0.57, p = .449, Cramer V = .08), but there was a higher proportion of adolescents within the clinical range of parent-reported internalizing problems in the adopted group: whereas in the adopted group there were 14 adolescents, there were none in the community group (χ² [1] = 7.45, p = .006, Cramer V = .28; medium effect size, Cohen, 1988).
Table 2. Descriptive Data and Mean Comparison for Parent-Reported and Self-Reported Internalizing Problems for Internationally Adopted and Community Adolescents.
| Adopted (n = 66) | Community (n = 30) | ||||||
|---|---|---|---|---|---|---|---|
| M (SD) | n (%) clinical | M (SD) | n (%) clinical | t (94) | Mean diff. 95 % BCa CI | Cohend | |
| Parent-reported internalizing problems | 4.98 (3.64) | 14 (21.2) | 2.63 (2.08) | 0 (0.0) | −4.01*** | [−3.54, −1.15] | 0.79 |
| Self-reported internalizing problems | 5.07 (3.47) | 13 (19.7) | 4.27 (3.03) | 4 (13.3) | −1.09 | [−2.14, 0.51] | 0.25 |
| Discrepancy scores | 0.14 (1.11) | − | −0.31 (1.11) | − | −1.85+ | [−0.91, 0.03] | 0.40 |
Note.BCa = Bias corrected accelerated, CI = confidence interval. BCa 95% CI based on 2000 samples. Bolded values indicate that the CI do not include zero.
***p < .001,
+p < .10.
Cross-Informant Discrepancies for Internalizing Problems in Internationally Adoptive and Community Parent-Adolescent Dyads
In the group of adopted adolescents, there were no statistically significant differences between parent- and self-reported internalizing problems (t[65] = 0.18, p = .859, mean difference 95% Bca CI [−0.82, 0.99], d = 0.02). For the community adolescents, parent-reported internalizing problems were significantly lower than self-reported internalizing problems (t[29] = 2.39, p = .021, mean difference 95% Bca CI [0.30, 2.93], d = 0.43). When comparing discrepancy scores, the discrepancy between informants was greater in the community group, with a small effect size (d = 0.40, p = 0.67; see Table 2). The bivariate correlation between parent- and self-reported scores in the adoption group was r = .45 (p < .001), whereas, in the community group, it was r = -.04 (p = .840). The two correlation coefficients were different (z = 1.93, p = .027).
Age at Adoption, Neurodevelopmental Problems and Post-Adoption Processes as Predictors of Internalizing Problems Among Internationally Adopted Adolescents
The following analyses were conducted only with the adoption sample. Table 3 displays descriptive data for internalizing problems and the percentage of adolescents with internalizing problems in the clinical range among those adolescents adopted earlier and later than 24 months. Late-adopted adolescents showed more parent-reported internalizing problems, with a small-to-medium effect size, although the bootstrapped 95% CI included zero. Similarly, among late-adopted adolescents, there was a higher proportion of adolescents in the clinical range of parent-reported internalizing problems than among early-adopted adolescents (χ² [1] = 4.51, p = .034), but this was not the case when comparing clinical scores of self-reported internalizing problems (χ² [1] = 0.02, p = .967).
Table 3. Internalizing Problems in Adolescents Adopted Before and After 24 Months.
| Age at adoption < 24 months (n = 20) | Age at adoption > 24 months (n = 46) | ||||||
|---|---|---|---|---|---|---|---|
| M (SD) | n (%) clinical | M (SD) | n (%) clinical | t (94) | Mean diff. 95 % BCa CI | Cohend | |
| Parent-reported internalizing problems | 4.05 (2.86) | 1 (5.0) | 5.39 (3.89) | 13 (28.3) | −1.39 | [−3.03, 0.27] | 0.39 |
| Self-reported internalizing problems | 4.72 (3.58) | 4 (20.0) | 5.22 (3.45) | 9 (19.5) | −0.53 | [−2.19, 1.34] | 0.14 |
Note.BCa = Bias corrected accelerated, CI = confidence interval. BCa 95% CI based on 2000 samples.
Table 4 shows the bivariate correlation matrix between covariables, age at adoption, internalizing problems, post-adoption processes, and neurodevelopmental problems within the internationally adopted group. The mean for adoption communication openness was rather high (M = 4.01, SD = 0.77, range 1-5), whereas for perceived discrimination it was low (M = 1.74, SD = 0.59, range 1-4). Twenty-six adopted adolescents (39.4%) did not present any neurodevelopmental problems, whereas 22 (33.3%) presented one, 14 (21.2%) two, and four (6.1%), the three of them. Neither age, age at adoption (as a dimensional variable), nor gender showed statistically significant associations with internalizing problems. Boys and girls did not show statistically significant differences in either variable of internalizing problems by Students’ t test mean comparison neither.
Table 4. Correlation Matrix Between Internalizing Problems, Covariates, Post-Adoption Processes, and Neurodevelopmental Problems Among Internationally Adopted Adolescents.
| Variable | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|---|
| 1. Age | - | |||||||
| 2. Age at adoption | .54*** | - | ||||||
| 3. Gender (1 = female) | −.12 | −.14 | - | |||||
| 4. Parent-reported internalizing problems | .15 | .12 | .17 | - | ||||
| 5. Self-reported internalizing problems | −.09 | .11 | .15 | .45*** | - | |||
| 6. ACO | .12 | −.23+ | −.06 | −.22+ | −.53*** | - | ||
| 7. Discrimination | .10 | .36** | .01 | .07 | .40** | −.16 | - | |
| 8. Neurodevelopmental problems (0-3) | −12 | .00 | .15 | .39** | .21+ | −27* | −.10 | - |
Note.ACO = Adoption Communication Opennes.
***p < .001,
**p < .01,
*p < .05,
+p < .10.
The summary of the multiple linear regression models predicting parent- and self-reported internalizing problems is displayed in Table 5. Both models were statistically significant. The model predicting parent-reported internalizing problems predicted 17% of the variance, considering the adjusted R2 . Neurodevelopmental problems and age at adoption later than 24 months predicted higher parent-reported internalizing problems.
Table 5. Summary of Multiple Linear Regression Models Predicting Parent- and Self-Reported Internalizing Problems by Covariates and Relevant Post-Adoption and Adversity-Related Factors.
| Parent-reported internalizing problems | Variables | Self-reported internalizing problems | |||||
|---|---|---|---|---|---|---|---|
| Variables | β | 95 % Bca CI | β | 95 % Bca CI | |||
| Lower | Upper | Lower | Upper | ||||
| Gender (female = 1) | .14 | -.08 | .36 | Gender (female = 1) | .09 | −.10 | .28 |
| Neurodevelopmental problems | .36** | .17 | .55 | Neurodevelopmental problems | .12 | −.04 | .28 |
| Age at adoption > 24 months | .21* | .02 | .42 | ACO | −.43*** | −.63 | −.25 |
| ACO | −.09 | −.31 | .07 | Discrimination | .34** | .14 | .51 |
| Adjusted R2 | .17 | .37 | |||||
| F | 4.28** | 10.43*** | |||||
Note.ACO = Adoption Communication Opennes, BCa = Bias corrected accelerated, CI = confidence interval. BCa 95% CI based on 2000 samples. Bolded values indicate that the CI do not include zero.
***p < .001,
**p < .01,
*p < .05.
The model predicting self-reported internalizing problems explained a higher amount of variance (adjusted R2 = .37). Higher adoption communication openness predicted lower self-reported internalizing problems, whereas more perceived discrimination experiences predicted higher internalizing problems. Neither gender nor neurodevelopmental problems were significant predictors for self-reported internalizing problems.
Discussion
This study aimed at analyzing internalizing problems in adolescents adopted from Eastern Europe to Spanish families, comparing them with a community group and using both a dimensional and categorical approach, as well as parent and self-reports for assessing internalizing problems. We explored the possible differences as well in informant discrepancies between the adopted and community group, and different adversity-related and post-adoption factors that could predict variability in internalizing problems among adopted adolescents.
As predicted, the adopted adolescents showed more internalizing problems than community adolescents community adolescents living with their birth families. However, this pattern of results was only apparent when comparing parent-reports of internalizing problems, whereas there were no differences between groups when using self-reports. This finding is partially consistent with the result of the meta-analysis on the mental health of internationally adopted youth of Askeland et al. (2017) showing higher differences with community controls when measuring mental health using parent rather than self-reports. The differences in internalizing problems between the adopted and the community group did not seem to be larger when using a categorical rather than a dimensional assessment of internalizing problems, contrary to previous results (Askeland et al., 2017).
Regarding the magnitude of agreement, whereas in the community group the agreement between parent and self-reports was very low or almost nonexistent, in the adoptive group the cross-informant agreement was higher and in the upper range of what has been previously found in community samples (r = .45; Rescorla et al., 2013). Regarding the direction of discrepancies, the hypothesis of higher internalizing scores when using self-reports was confirmed only for the community group, but not for the adoption group, where the cross-informant discrepancy was minimal and there were no differences between parent and self-reports on internalizing problems. This finding was unexpected, since previous studies with adopted populations did find higher self-reported internalizing problems when compared with parent-report (Roskam et al., 2017; Muzi & Pace, 2023; Wiik et al., 2011; Wright et al., 2022) and no differences in the magnitude and direction of informant discrepancies between adopted and community groups (Roskam et al., 2017).
A possible explanation may be the higher level of adversity and a higher parental awareness of the more complex profile of adolescents adopted from Eastern Europe like those in our sample, as compared with adolescents adopted domestically or internationally from other areas of origin in previous studies (Roskam et al., 2017; Wiik et al., 2011: Wright et al., 2022). It is open to discussion whether the lower level of informant discrepancy is related to a lower threshold of adoptive parents for mental health concerns (Miller et al., 2000), or to other mechanisms at play.
The potential predictors of internalizing symptoms also behave differently depending on the informant for internalizing problems. The variability explained by the regression model was relatively low for parent-reported internalizing problems. Two indices related to early adversity the duration of psychosocial deprivation and the potential neurodevelopmental consequences of adversity, predicted (modestly) higher internalizing problems. An adoption after 24 months predicted higher internalizing problems, mirroring previous findings with a large sample of internationally adopted children and adolescents from four to 18 years using the same age at adoption cut-off (Gunnar et al., 2007).
A summary index of adversity-related neurodevelopmental problems, including ADHD diagnosis, FASD diagnosis or confirmed prenatal alcohol exposure, and severe deficit in head circumference as an index of brain development, also predicted higher parent-reported internalizing problems among the adopted adolescents. The links between neurodevelopmental problems and internalizing symptoms may be direct, as in the disturbances in affect regulation associated with FASD, or mediated through the widespread social and educational impairment associated with these adversity-related neurodevelopmental difficulties (Biederman et al., 1998; Chudley et al., 2005), as shown by Golm et al. (2020).
Self-reported internalizing problems, on the other hand, were particularly predicted by post-adoption processes, specifically by adoption communication openness and perceived ethnic and adoptive discrimination. This is consistent with the limited research findings about the positive effects of open communication about adoption for adopted individuals’ adjustment and self-esteem (Brodzinsky, 2006; Grotevant et al., 2011). Perceived discrimination also predicted higher self-reported internalizing symptoms, in line with previous findings showing the negative effect of discrimination on depression and mental health in general among the general population (Schmitt et al., 2014) and among intercountry adopted youth specifically (Arnold et al., 2016; Ferrari et al., 2017; Koskinen et al., 2015). Thus, in the adoption sample, there is an interesting contrast between parents and adolescents regarding the factors predicting internalizing problems: while in the parents those factors are more objective (age at adoption, neurodevelopmental problems), they are more subjective in the case of the adolescents (personal assessment of communication openness, perceived discrimination). This suggests that the lived experience of adoption (Brodzinsky et al., 2022) is both a source of influence and the product of other influences.
A limitation of the study was the cross-sectional design, which impede ascertaining the directionality of the effects. The temporal precedence of the adversity-related variables, which showed relations to parent-reported internalizing problems, supports a predictor-to-outcome effect. However, for post-adoption processes and self-reported internalizing problems, bidirectional relations could be expected, given the shared informant used for measuring these constructs (self-report questionnaire) and the links between negative affect and self-reports (Watson & Pennebaker, 1989). Future studies with a longitudinal approach could clarify the role of post-adoption processes such as adoption communication or discrimination on internalizing problems. Another limitation was the sample size, which, particularly for the community adolescent’s group, was small. Our measure of internalizing problems was relatively short, although its discrimination, convergent, and construct validity have been proved with detailed psychiatric interviews (Goodman et al., 2010).
Notwithstanding these limitations, we believe our study contributes to a better understanding of internalizing or emotional problems among post-institutionalized, internationally adopted adolescents. The somewhat higher presence of adolescents with internalizing symptoms with clinical significance among internationally adopted adolescents from Eastern Europe reinforces the idea that emotional problems merit further attention in this population in adolescence, especially among individuals who were adopted at a later age, those with neurodevelopmental problems, or, more broadly, among those from areas involving more preadoption adversity like Eastern Europe.
The study also provides evidence on the relevance of the informant when assessing mental health among internationally adopted children and interpreting research findings, since our results point that the differences in parent-reported internalizing problems may be partly due to differences in the pattern of informant discrepancies between adoptive and community parent-dyads, at least in adolescents adopted from Eastern Europe. Our study also reinforces the idea that adopted adolescents’ mental health outcomes are not only related to the pre-adoptive early adversity but also to post-adoption processes like adoption communication openness or the discrimination experiences they may experience due to their ethnic or adoptive status (Grotevant et al., 2011), highlighting the relevance of the lived experience of adoption.
Taken together, our results help to extend and nuance previous findings on the presence of emotional problems during adolescence of internationally adopted youth who had suffered early adverse experiences in the form of institutionalization and other hazards and on the potential role for adopted individuals’ adjustment of post-adoption processes. This may prove to be useful both for understanding the long-term consequences of early adversity and for prevention and intervention efforts addressing emotional problems among internationally adopted people as they develop through adolescence and early adulthood.

