Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkHighlight
This systematic review shows that deprescription of antipsychotic medicines in patients with dementia is feasible.
The results of the review, together with the principle of prudence, show that gradual deprescription is a better alternative than abrupt deprescription.
Further research is needed to examine the effectiveness of other deprescribing strategies in terms of different variables.
Introduction
Around the world, populations are ageing, and this demographic transition will affect almost all aspects of society; today, there are more than 1 billion people aged 60 years or older. One condition, in particular, could well challenge World Health Organization (WHO) and the United Nations (UN) ambitions: dementia1-3)..
Dementia is a major cause of dependence and disability among older people worldwide. It is estimated that around 57 million (2019) people suffer from some type of dementia globally and is expected to increase to 153 million in 20501,4. Alzheimer’s disease (AD) is the most common form of dementia and may contribute to 60-70 % of cases3,4 . The global cost of dementia is estimated to be US$ 818 billion, 16 % of which is associated with direct health care costs3 . Dementia is currently the seventh leading cause of death and one of the major causes of disability and women are disproportionately affected by dementia, both directly and indirectly. Women experience higher disability-adjusted life years and mortality due to dementia, but they also provide 70% of care hours for people living with dementia5.
Dementia is characterised by deterioration in memory and in at least one other higher cognitive function that is severe enough to cause significant limitations in social or occupational functioning and is not explained by delirium or another axis I disorder6 .These limitations present themselves as cognitive and non-cognitive or behavioral and psychological symptoms of dementia (BPSD). BPSD are defined as disturbances in perception, thought content, mood or behaviour that frequently occur in patients with dementia7, and account for greater functional disruptions along with higher family burden8)..
Given the high prevalence of neuropsychiatric symptoms (NPS), the commonly used treatment is based on psychotropic medications. Atypical antipsychotics have greater recommendations in clinical guidelines for the management of agitation, aggression, and psychosis9) .While these have been proven effective10,11, the use of antipsychotics is associated with increased risk of mortality, stroke and other adverse events such as falls, sedation and cognitive decline12. This increase in adverse events confirms that antipsychotics (in generic form) should not be used routinely to treat patients with dementia with aggression or psychosis, unless there is serious distress or risk of physical harm to those who live and work with them13,14. A meta-analysis published by Schneider et al. (2005) estimated a similarly increased risk in mortality (OR = 1.54, 95 % CI 1.06 to 2.23, p= 0.02) for atypical neuroleptics15.
The available evidence, including clinical consensus, indicates that given the potential adverse effects, the first line of treatment for behavioral symptoms in dementia should be a non-pharmacological intervention. In addition, withdrawal of the medication must be contemplated. Prolonged use is indicated in patients with a history of severe episodes of psychosis or concomitant schizophrenia15.
According to Reeve et al.17, deprescribing can be defined as the process of ceasing inappropriate medication, supervised by a healthcare professional, with the aim of managing polypharmacy and improving clinical outcomes. Strategies described to promote deprescribing practices include comprehensive medication reviews, educational interventions and auditing of prescribing practices. These interventions have shown a number of benefits such as reducing polypharmacy, potential drug-to-drug interactions (pDDI) and the costs related to the use of medications. Thus, the objective of this article is to conduct a systematic review to synthesize the evidence about the withdrawal of antipsychotics in people with dementia that should be tapered or abrupt.
Methods
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guideline18. For this purpose, we designed a literature search strategy with both controlled terms (Medical Subject Heading) and free-text terms and adapted them to each of the databases used: PubMed, Embase, Web of Science-Core Collection, Cochrane Library, Scopus, MEDLINE (Ovid), and PsycINFO (Appendix A).
Inclusion/exclusion criteria
We included intervention studies (randomized or quasi-experimental trials), published between year 2000 and 2023 in Spanish or English, evaluating the effectiveness of antipsychotic deprescribing strategies (dose reduction or complete withdrawal) in people with dementia. The outcome measures under consideration were mortality, relapses of behavioral symptoms, quality of life and cardiovascular events. We excluded articles that examined deprescription of both antipsychotics and benzodiazepines together.
Data extraction and synthesis of results After removing duplicates, we screened by title and abstract all references identified in the different databases consulted to verify they potentially met the inclusion criteria. The full text of the selected articles was then reviewed and evaluated (AOC and AOL or EMR) by two independent reviewers. Any disagreement between reviewers throughout the screening and selection process was resolved by consensus by another reviewer (AOL or EMR). The Rayyan QCRI™ program was used for this purpose.
A data extraction form was designed and piloted to gather information on the methodology of the study, characteristics of the target population, interventions developed, main outcomes, follow-up time and study design. This work was performed independently by the three authors to reduce the risk of potential biases or errors.
Risk of bias
For assessment of risk of bias in the clinical trials, we used the check list prepared by Higgins et al.19 for the Cochrane Collaboration, covering six domains. A parallel independent assessment was carried out by the two authors and discrepancies were resolved by the third investigator. In the case of quasi-experimental studies, an ad hoc modification of the tool was made for the items linked to random generation and sequence generation, since these criteria are not applicable in the included studies. The evaluation has focused on assessing aspects related to selection bias and its minimization strategies through the selection and number of participants included, the control of confounding variables and the types of analysis performed.
The authors carried out a qualitative synthesis of results from the included studies and classified the articles according to type of intervention. Given the considerable heterogeneity observed among studies, in terms of type of intervention and outcome measures, a quantitative synthesis was not considered appropriate.
Results
The search returned a total of 2248 references, of which 1158 duplicate references were removed, leaving a total of 1090 references (Figure 1). After the first reading of titles and abstract, a total of 127 articles were selected for full-text review. Finally, eight articles were included in this revision. Four reviews were used only to identify relevant articles from their reference lists and for background information or discussion20-23.
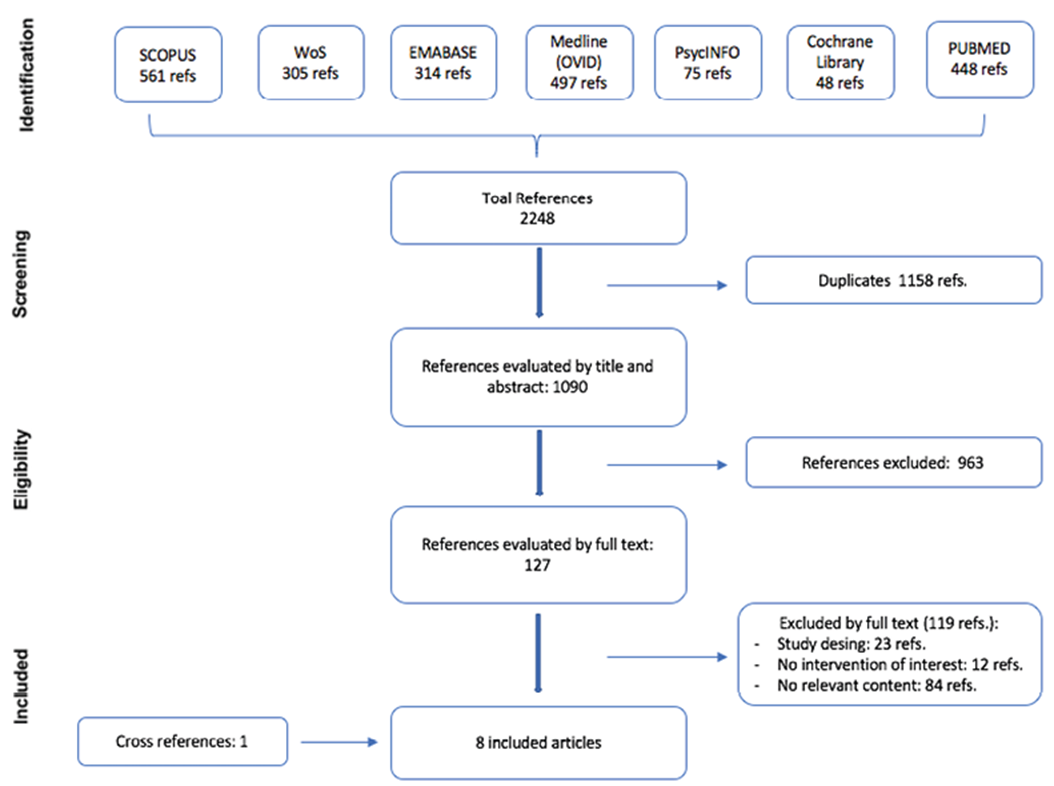
With regard to the characteristics of the included studies (a total of 789 patients included), it is worth noting that six of them were clinical trials24-29) and two were a quasi-experimental design30,31 . With regard to the study site, two were conducted in the United Kingdom, the others were conducted in the United States (n= 2), Norway (n= 1), Australia (n= 1), Spain (n= 1) and Canada (n= 1) (Table 1). 25% of the studies had sample sizes involving less than 40 participants, most of them (62.5%) living in nursing or residential care homes for the older people, 12.5% were users of geriatric day hospitals, and 25% had non-institutional nursing care. As for the intervention, three studies used an abrupt withdrawal schedule25-27, four used a gradual dose reduction as stipulated in a protocol(24,28, 29,31) and one compared abrupt withdrawal with gradual reduction30) (Table 1).
Table 1 Characteristics and outcomes of studies included.
| Author | Methods | Participants | Description of the Intervention and follow up | Participants description | Outcomes |
|---|---|---|---|---|---|
| Intervention: abrupt withdrawal schedule | |||||
| Ballard, 200425 | Double-blind randomized clinical trial | Senior residents with BPSD from United Kingdom residences. | Abrupt discontinuation of treatment (12-week follow-up). CG was treated with placebo and IG, received active treatment with antipsychotic. | 100 patients (IG= 46 and CG= 54) were studied, who were randomized to 2 groups. The CG the mean age was 83.6 ± 9.3 years for the IG and 83.1 ± 7.1 years for the CG. | The IG had a mean score NPI = 16.0 and the CG NPI = 14.0. When the APS was interrupted abruptly, the IG (mean NPI score <14 (p= 0.46)) shows statistically non-significant changes in agitation (p= 0.89), mood (p= 0.85) and psychosis (p= 0.41). In patients with low doses of APS and NPI <14, the change in agitation reaches statistical significance (p= 0.018). |
| Ruths, 200826 | Randomized clinical trial with 4-week follow-up | Older people with dementia in residences (≥3 months) being treated with antipsychotic for BPSD. | Abrupt discontinuation of antipsychotics for 4 weeks. Following: (≥3 months). CG maintained with antipsychotic treatment for four-week intervention. IG was antipsychotic discontinuation. | 55 patients (IG= 27 and CG= 28) were included, mean age 84.1 ± 7.1 years, and 43 women. | In IG, 22 participants were maintained without requiring antipsychotic treatment. The BPSD (evaluated with NPI) remained stable or even improved in 42 patients (IG = 18 and CG = 24; p=0.18). Patients with greater behavioral impairment required higher doses of antipsychotics at baseline compared to those with better NPI scores (p=0.42). |
| Ballard, 200927 | Randomized clinical trial | Institutionalized older people with a diagnosis of dementia and BPSD (≥3 months) in residences in the UK. | Abrupt discontinuation of antipsychotics.104 weeks follow-up. CG was maintained with placebo and IG treated with their antipsychotic treatment for 12 months. | 165 patients were randomized (CG= 83 and IG= 82), Baseline SIB and NPI scores for IG were 73.8 ± 20.7 and 15.8 ± 11.3 and for CG 71.1 ± 22.7 and 17.4 ± 14.6 for CG. 128 (78 %) started the study, 64 of them in each group. | 12-month mortality: The cumulative probability of survival during the 12 months was 89.7 % (95 % CI: 71.3 %-96.5 %) and 97.1% (95 %CI: 80.9-99.6 %), for CG and IG respectively. Among those who received at least one dose, survival (ITTm) was 70.3% (95 %CI 57.5-79.9 %) and 76.6% (95 %CI 64.2 % -85.2 %), while it was 74.7% (95 %CI 63.9-82.7 %) and 79.3 % (95 %CI 68.8-86.6 %) according to randomization (ITT). 54-month mortality: CG showed higher mortality than IG (p=0.03, HR 0.58 [95 %CI: 0.35-0.95]; ITT according to randomization p=0.02, HR 0.58 [95 %CI 0.36-0.92]), the difference in mortality was more pronounced after the first year. |
| Devanand, 201128 | Randomized clinical trial in two phases. | Alzheimer’s outpatients with agitation, aggression, or psychosis | Two phases (with follow-up of 44 weeks): Phase A: after a washout period of one week washing of antipsychotics, a flexible dose of haloperidol was prescribed (according to response and EA). Phase B: those who responded favorably were randomized to carry out the intervention: discontinuation or continue with haloperidol. CG, there was a 2-week double-blind sequential placebo substitution tapering period: patients on 4 mg daily at end-Phase A switched to 2 mg daily for 1 week, 1 mg daily for the next week and then switched completely to placebo; patients on 2 or 3 mg daily switched to 1 mg daily for 2 weeks and then switched to placebo, and patients who received 0.5 mg or 1 mg were switched directly to placebo without a tapering period. | 78 patients with a mean age of 75±8.0 years were studied, 57 % of which were women. | Phase A: target symptoms (agitation and psychosis) and BPRS score decreased (p <0.001), but extrapyramidal symptoms increased (p <0.01). At the end, 22 people responded to the treatment, of which 20 completed the follow-up Phase B: the proportion of patients was higher (40 % vs 80 %; p=0.07) and less time to relapse in the discontinuation group compared to the haloperidol group (p=0.04). Neither baseline nor residual severity of target symptoms predicted relapse in phase B. |
| Devanand, 201229 | Randomized clinical trial in two phases | Patients from veteran medical centers, memory clinics and geriatric clinics in the USA with Alzheimer’s who present agitation, aggressiveness or psychosis | Two phases (48-week follow-up): Phase A (16 weeks): after one week of washout, a flexible dose of risperidone was prescribed (according to response and adverse events). Phase B (32 weeks): those who responded were randomized to: (Group 1) continue risperidone. (Group 2) risperidone 16 weeks and placebo 16 weeks) and (Group 3) placebo. Phase A: equal treatment. Phase B: CG received placebo for 32 weeks. | 180 patients initiated the study with a mean age of 79.6 ± 7.6 and 59 % women. 80 % had psychosis and 81 % agitation-aggressiveness. | Phase A: The severity of psychosis and agitation symptoms was reduced (p <0.001), although extrapyramidal symptoms increased (p=0.009). General physical symptoms decreased, and physical self-maintenance worsened (p <0.001). The relapse or recurrence rate of BPSD was higher among those on placebo than with risperidone (60 % [24 of 40 patients in G3] v / s 33% [23 of 70 patients in G1 and G2], p=0.004 Phase B: of the 112 patients who responded, 110 were randomized. The group that received placebo (Group 3), compared to those that continued with risperidone (mean dose 0.97 ± 0.74 mg) (Group 1 and 2) showed a higher risk of relapse (HR 1.94; 95 % CI 1.09-3.45; p=0.02). During the next 16 weeks, the group that stopped risperidone and switched to placebo (Group 2) showed a higher risk of relapse HR 4.88; 95 % CI: 1.08-21.98 (p=0.02), than the group that continued with risperidone (Group 1). No significant differences were found in adverse events between the 3 groups. |
| Intervention: gradual dose reduction | |||||
| Brodaty, 201831 | Longitudinal study Prospective cohort) | Older adults living in 23 nursing homes and receiving antipsychotic treatment (> 3 months) | Two components (follow-up of 52 weeks): 1) Training for health workers. 2) Deprescription protocol based on dose reduction to 50% every 2 weeks and complete withdrawal after 2 weeks in minimum dose. | A total of 139 residents met the inclusion criteria, with 93 residents completing the follow-up. The mean age of 84.3 ± 7.3 years, 65.6 % were women and 66.9 % completed the follow-up. | The most common cognitive symptom was agitation/ aggressiveness (89%); risperidone was the most widely used antipsychotic (n=62.4 %). Withdrawal from antipsychotics was achieved in 86.2 %, 79.1%, 81.7 % of patients at 3, 6 and 12 months, respectively. There was no significant change in the NPI-NH score. |
| Bravo, 201930 | Quasi-experimental trial without a control group | Older people with dementia and treated with ≥1 antipsychotics from a care center in Spain | Reduction and / or suspension of antipsychotic treatment, according to symptoms with a follow-up of 52 weeks. Dose reduction to 50 % every 2 weeks and completely withdrawn after two weeks in minimal dose. | The study began with 38 residents, of whom 3 withdrew due to deterioration. The mean age was 82.31 ± 5.81 and 60 % were women. | The patients had severe Barthel dependence = 33.29 ± 28.62 and a previous NPI-NH score of 12.91 ± 12.80. At 6 months of evaluation, there was no statistically significant difference in the NPI-NH score = 13.76 ± 16.68 (p=0.124). At the end of the follow-up period, 2 residents required a return to the prescription of antipsychotics. |
| Van Reekum, 200224 | Randomized double-blind clinical trial | Patients with dementia under treatment with antipsychotics (> 6 months) from 2 nursing homes and a geriatric ward in Canada. | Antipsychotic dose reduction of 50 % in the first week and half of the remaining dose in the second week (26-week follow-up). CG, received placebo during pretrial phase and dose reduction phase. | A total of 34 residents (IG= 16 and CG= 17) were studied, the mean age of the IG was 84.4 ± 4.6 and 82.9 ± 6.9 years for CG. | Daily doses (chlorpromazine equivalents) were 24.9 mg for IG and 34.3 mg for CG. 23.5 % of the IG subjects were withdrawn from the study early due to behavioral worsening, compared with 18.8 % of the CG (RR=1.33; 95 %CI 0.25-7.17). When evaluating the intervention, the CG showed a tendency to worsen behavioral problems (p=0.06), self-harm (p=0.08), especially in the persistence initiation subscale (p=0.05). In IG, the antipsychotic dose was higher among those who worsened than in those who were stable (p=0.06). |
APS: antipsychotics IG: intervention group; CG: control group; SIB: Severe Impairment battery; BPSD: Behavioural and Psychological Symptoms of Dementia; NPI: Neuropsychiatric Inventory; NPI- NH: Neuropsychiatric Inventory - Nursing Home Version; RR: Relative Risk; 95% CI: 95% confidence Interval; ITT: Intention to treat: ITTm: Intention to treat-modified; HR: Hazard ratio; BPRS: Brief Psychiatric Rating Scale.
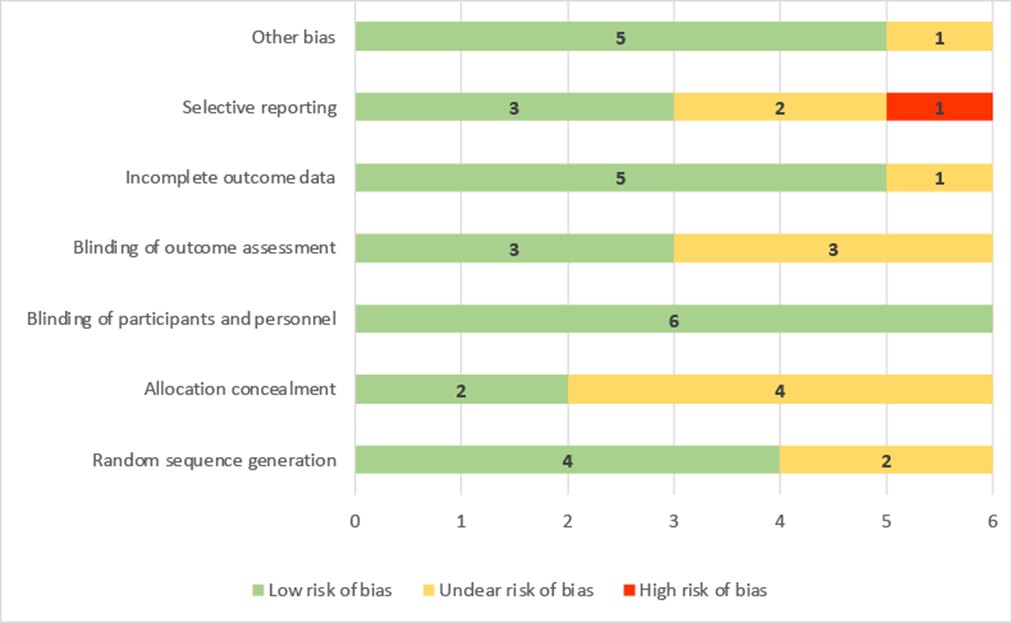
Risk of Bias
The results of the risk of bias assessment are shown in figures appendix A1, A2 and A3. The risk of bias in the included clinical randomized trials is low in general. It should be stressed that the blinding of participants and personnel was clearly described in all the trials. The domain regarding selective reporting scored to be at high risk of bias in one trial24. Regarding quasi-experimental studies, Bravo30 scored at high risk of bias in three of the domains.
Abrupt withdrawal Schedule
Regarding the effectiveness of the interventions (Table 1), only Ballard (2009)27 assessed survival, using Cox regression. Findings revealed that patients who followed an abrupt withdrawal from antipsychotic medication showed a statistically significant lower risk of mortality at 24 months (HR=0.58; 95 % CI: 0.36-0.92) than patients who continued with treatment.
Two cross-over clinical trials examined relapse rates following abrupt withdrawal from haloperidol28 and risperidone,29 with follow-ups of 24 and 48 weeks respectively, including 4428 and 11029 patients, who remained stable (responders) the last month. Devanand28 observed a higher rate of relapse of BPSD (p= 0.07) and a shorter time to a relapse (p= 0.04) in the group that received placebo compared to the group that continued to receive antipsychotic medication. Later, in 2012, Devanand29 showed that after 16 weeks of follow-up, the relapse rate of BPSD was higher in patients who received placebo than in those who continued with risperidone (HR= 1.94, 95 % CI: 1.09-3.45). This result was maintained for 32 weeks (HR= 4.88, 95 % CI: 1.08-21.98).
Ballard25 evaluated the abrupt discontinuation of antipsychotic medication, performing cluster analyses according to the Neuropsychiatric Inventory (NPI) score. He found that patients with NPI score <14 (mild) who were discontinued from antipsychotics showed no significant difference in the baseline NPI (p=0.46) (intragroup difference). In contrast, patients with NPI >14 (moderate to severe) showed a significant difference in the management and relapse of BPSD variables compared with the control group (p= 0.018) (intergroup difference). Ruths’ review showed that, regarding the abrupt withdrawal of antipsychotics (risperidone, haloperidol, or olanzapine), there are no differences in relation to improvement or harm in BPSD (p= 0.18)26. It is important to underline that patients who received previously high doses showed greater levels of behavioral deterioration after withdrawal (p= 0.042).
Gradual dose reduction
Three studies evaluated the effectiveness of the gradual withdrawal of antipsychotics, by tapering to half of the daily dose in the first week and removing the dose over the following two weeks. Bravo (2019)30 included 35 patients, and at 6 months achieved total withdrawal in 80% of patients and dose reduction in the rest of patients; whereas Brodaty31 achieved withdrawal from antipsychotics in 79.1 % and 81.7 % (95 % CI: 72.4 %-89 %) of patients at 6 and 12 months, respectively. Both studies showed no statistically significant differences in BPSD (p> 0.005), compared to baseline values. It should be noted that Brodaty31 found statistically lower rates of relapse of BPSD among patients who were withdrawn from antipsychotics compared to patients who continued with treatment (p= 0.005). Finally, the Van Reekum study24 involving 34 patients, found that those who were withdrawn from medication had a non-significant increased likelihood of exacerbation of behavioral symptoms (RR 1.33; 95 % CI: 0.25-7.14). Bravo30 used a strategy of reduction and/or discontinuation of antipsychotic medication, and at 6 months of follow-up no significant differences were found in the Neuropsychiatric Inventory-Nursing Home version (NPI-NH) score.
Discussion
This review shows that deprescribing antipsychotics is feasible among people with dementia, but further research is needed to reconfirm these findings32,33 . The review also shows that deprescribing is associated with benefits in terms of survival, and with potential improved outcomes in the management and relapse of BPSD18. These results are similar to those described in the review by Van Leeuwen (2018)33 which worked on a similar objective to the present review, but presents different inclusion criteria.
When reviewing the selected articles and comparing the clinical results, no major difference is observed in the management of BPSD through abrupt or gradual withdrawal schemes. In contrast, abrupt withdrawals showed significantly higher rates of relapse and/or adverse events28,29. In this regard, a systematic review that included four clinical trials comparing abrupt versus gradual antipsychotic discontinuation in patients with schizophrenia34 found no significant differences in clinical outcomes (extrapyramidal signs, adverse events, etc.). In summary, there are no differences between reducing or continuing antipsychotic doses in terms of quality of life and functionality. However, with dose reduction there was a higher risk for relapses and dropouts, and potentially for rehospitalisations35.
Thus, it is concluded that it is preferable to withdraw gradually, because of the principle of prudence36. On the other hand, the systematic review conducted by Sheehan (2017)36, including 21 studies, failed to draw firm conclusions on the best way to approach deprescription in patients with intellectual disability, since it was found that patients did not tolerate discontinuation and required that the antipsychotic medication be re-prescribed.37
These findings are consistent with the review conducted by Page (2016)20, which included a total of 132 articles (34,143 participants) that evaluated deprescribing one or more medications in older people. In non-randomized studies, deprescribing was shown to significantly reduce mortality (OR 0.32; 95 % CI: 0.17-0.60). However, deprescribing did not significantly modify mortality in the randomized studies (OR 0.82; 95 % CI: 0.61-1.11).
Two factors found in the literature are associated with higher probabilities of successful deprescribing. One is a lower dose of antipsychotics30,34 , since in patients requiring low doses (even without reaching therapeutic threshold), the need for the use of antipsychotic medication may not be justified. It is important to pay special attention to the narrow dose-time relationship; according to evidence some doses of antipsychotics greater than 62-74 mg chlorpromazine equivalents are associated with a lower probability of achieving sustained deprescription over time21 .The other factor is related with the fact that patients with lower levels of functional impairment (NPI lower than 14) show better outcomes in the management of the BPSD (though with no statistical significance in relation to total NPI) and lower rates of relapse.23 This could indicate that measurements of BPSD (using the NPI rating scale) could be interfered by other symptoms or contexts38,39 and this issue has important clinical relevance. This result has also been observed in patients with a diagnosis of schizophrenia35.
It should be noted that evidence and clinical practice guidelines recommend antipsychotic treatment with risperidone, which is the neuroleptic that offers the biggest benefits in the management of BPSD40,41 . On the other hand, typical antipsychotics, olanzapine injection (atypical antipsychotic) or haloperidol (as a second line), are recommended in emergency situations where there is severe psychomotor agitation39,41) . In addition, typical antipsychotics show a higher incidence of known adverse events than their more modern congeners (atypical)40 .
The potential benefits of the use of antipsychotics may be diminished when the treatment is longer than required16,23. In this sense, there is a greater likelihood of adverse events linked to the use of antipsychotic medication (extrapyramidal signs, metabolic disorders, cardiovascular risk, death) after four months of treatment, and an increased risk of mortality after 12 months of treatment. Based on the above and taking into account the results yielded by this review, it seems reasonable that tapering off antipsychotic medication should be assessed after 12 weeks of treatment or once BPSD are under control16,39. This assessment should take into account the risk of occurrence of adverse events and the loss of effectiveness of treatment.7 Follow-up of the patient is required after medication withdrawal. In this regard, it is important to take a holistic and integrated approach to assessment, considering not only patients’ BPSD but also their family or supportive situation, etc.39-41. The evidence suggests that deprescription is necessary, and when it is guided by ad-hoc professionals, it shows better results42. Ballard (2002)43 showed that liaison psychiatry turns out to be a powerful strategy when it comes to reducing the inappropriate use of antipsychotics in people with dementia.
This review has several limitations that should be considered when interpreting the results. First, the low number of subjects included in the different studies, followed by the fact that most studies involved institutionalized patients, 5 trials involving nursing homes out of 8 included. These aspects may limit the external validity of the results, since pharmacotherapeutic monitoring and control may differ at community levels. The heterogeneity in terms of proximity and accessibility to health services of some residences should be taken into account. Other factors and contexts that could lead to different results should also be take into consideration. These issues make the extrapolation of the results to the community setting somewhat limited.
Finally, the authors consider that an optimal deprescription of antipsychotics, in accordance with the de-implementation of low-value clinical activities44-46 must include training that allows clinical teams to evaluate and compare performance between professionals and health centers, based on a body of evidence, under a multisectoral approach, and taking into account the principle of patient autonomy47,48) . It is also worth noting that a systematic review found that physicians frequently overestimated benefit and underestimated harm when evaluating treatments47. Further research is needed in this area, with studies involving a larger number of participants, other contexts and different sociodemographic characteristics.