










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Leptomeningeal carcinomatosis (LC) results from the spread of cancer cells to the leptomeninges. LC is diagnosed in 4-15% of cancer patients [1]. The malignancies most frequently associated with LC are: hematologic (lymphoma and leukemia), breast, lung, head and neck cancer, melanoma, and gastric cancer. In most cases (70%), LC is diagnosed in the advanced phase of the disease. However, in 5-10% of patients, LC is the initial manifestation of cancer (including cases where the primary neoplasm cannot be found). Up to 20% may present as a recurrence of the disease. Despite efforts to an early diagnosis, the prognosis of patients with LC continues to be unfortunate.
CASE REPORT
A 46-year-old male ex-smoker with a history of latent tuberculosis treated at 18 years old came in 2020 to the Emergency Department of the University Hospital Complex of Albacete three times for myalgia, chills, and lumbar pain for about three weeks. In the last 48 hours, he suffered headaches and vomiting. A chest X-ray showed an infiltrate in the right hemithorax. He was admitted to the Pneumology department with suspicion of right pneumonia. Seventy-two hours after admission, he presented a convulsive crisis. 24 hours after this episode, he began with blurred vision in the right eye and loss of visual acuity, rapidly evolving to bilateral amaurosis. The ocular fundus was normal. Cerebrospinal fluid (CSF) showed pleocytosis with a predominance of mononuclear cells, hyperproteinorrhachia, and glucose consumption (table 1). CSF cultures were negative, and cytology was negative for malignant cells on two occasions.
Table 1. Characteristics of cerebrospinal fluid.
| Macroscopic | Trasparent |
|---|---|
| Total cells | 321 /µL |
| Mononuclear cells | 70% |
| Polymorphonuclear cells | 30% |
| Lactate dehydrogenase | 257 U/L |
| Proteins | 0,70 g/dL |
| Glucose | 44 mg/dL |
| Multiple PCR* | Negative |
| Serologies | Toxoplasma, Cytomegalovirus, lues, Lyme disease: Negative |
| Adenosine deaminase | 15,7 U/L |
| Tuberculosis detection | Polymerase chain reaction, detection of acid-fast bacilli, Cultures: Negative |
| Cytology | Lymphocytic pleocytosis. Negative for malignancy. |
| Flow cytometry | T CD3 lymphocytes 13.73%, T CD4 6.46%,JNK 1.18, B CD19 lymphocytes 89.17, suppressor T lymphocytes (CD8) 6.63. 8% of the cellularity of the sample corresponds to elevated CD19++/CD5-/CD10+d FSC and SSC B cells with restriction of Kappa+ light chains, similar to those described in the lymph node study. Conclusion: Study compatible with infiltration by SLP-B |
*Polymerase chain reaction to detect: E.coli K1, H.influenzae, L.monocytogenes, N. meningitidis, S.agalactiae, S.pneumoniae, C.neoformans/gattii, Cytomegalovirus, Enterovirus, Herpes simplex virus type 1 and 2, Herpesvirus humano 6, Parechovirus y Varicella-Zoster virus.
Magnetic Resonance Imaging (figure 1) showed mononeuritis multiplex and leptomeningeal uptake. Computed tomography revealed a mass in the mediastinum and right lung hilum, a second mass in the retroperitoneum with extension to the psoas muscle, and multiple mesenteric and retroperitoneal adenopathies.
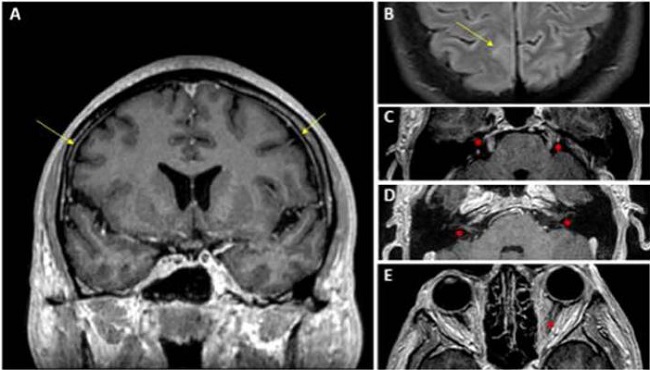
Figure 1. Brain magnetic resonance imaging with intravenous contrast administration: (A) T1 sequence with contrast in the coronal plane; (B) FLAIR sequence with fat suppression after contrast administration in the axial plane. In both images, the leptomeningeal uptake is marked with yellow arrows, appreciating the involvement of the convexity grooves in image B; (C, D, E) different sections of the T1 sequence with contrast in the axial plane in which contrast uptake of cranial nerves V (image C), VII and VIII (images C and D) and the left optic nerve is observed (image E) all of them indicated with red asterisks.
In the third sample obtained of CSF, flow cytometry was compatible with B-type Lymphoproliferative Syndrome. After flow cytometry result, cytology of this third sample was revised and is shown in figure 2.
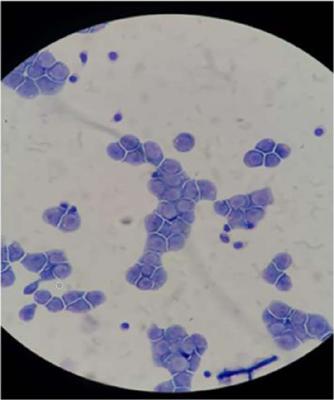
Figure 2. Cerebrospinal fluid cytology. Monomorphous infiltration of large cells with a blastoid appearance. They resemble the lymphoid series, presenting abundant intensely basophilic cytoplasm and the presence of several vacuoles. The nucleus is large, with loose chromatin on occasions and the presence of a prominent nucleolus in most of them.
A biopsy of the lymph node and the mediastinal mass was compatible with type B high-grade lymphoma. A bone marrow biopsy showed type B lymphoproliferative syndrome infiltration. Immunohistochemistry and FISH were consistent with triple HIT high-grade B lymphoma. The patient received high-dose systemic and intrathecal chemotherapy treatment with methotrexate (MTX). Despite this, progression continued in the central nervous system, with no response to several lines of chemotherapy treatment, with subsequent death of the patient.
DISCUSSION
High-grade lymphoma is a type of aggressive lymphoma made up of mature B cells that, for biological and clinical reasons, should not be classified as diffuse large B-cell lymphoma (DLBCL), lymphoma NOS (not otherwise specified), or Burkitt's lymphoma. It constitutes a lymphoma with intermediate features between DLBCL and Burkitt's lymphoma at the morphological level [2].
In general, lymphoma's involvement in the central nervous system (CNS) is rare except for external invasion or compression. Although, as in this case, it can occur at diagnosis, the involvement of the CNS is more common in recurrences (between 2.8 to 24.4%) [3]. The histological subtype is the most important risk factor for the involvement of the CNS. Other risk factors are CNS-International prognostic Index, kidney and adrenal gland involvement, and double or triple hit lymphomas [4].
The cranial nerve involvement is more common in LC secondary to hematological processes than when it is secondary to solid tumors [5]. A study of 45 patients found root or spinal involvement in 53% of LC secondary to solid tumors. In contrast, in LC of hematological origin, cranial nerve involvement occurred in up to 53%, and 67% among all 45 patients with multifocal neurological symptoms [6]. Kaplan et al. reviewed 63 patients whose most frequent form of LC presentation was headaches, seizures, lethargy, and cranial nerve involvement [7]. The presentation of our patient was “atypical” because it presents bilateral optic neuritis with rapidly progressive total amaurosis as a predominant clinical feature.
LC is a diagnostic challenge. In CSF, flow cytometry (FCM) has a higher sensitivity than cytology for the diagnosis of CL [8]. Three CSF samples were negative in our patient, and finally, FCM gave the diagnosis. A positive result on CSF cytology depends on the proportion of malignant cells in the sample and the sample's integrity, and repeated lumbar puncture is sometimes required to obtain positive results in patients with LC. It is recommended to send two separate samples with at least 30 ml to increase the diagnostic possibilities of cytology. Despite these measures, CSF cytology may be negative in up to 20% of patients.
Another factor that made diagnosis difficult was elevated adenosine deaminase (ADA) activity in CSF (Table 1). Our patient had a history of treated tuberculosis and currently had elevated CSF ADA, so initially, meningeal tuberculosis was suspected. ADA is an enzyme involved in the catabolism of purines, and its main activity is related to lymphocyte proliferation and differentiation. High ADA levels pose a differential diagnosis, including diseases with increased lymphocytes such as infections (tuberculosis or other bacterial or viral meningitis), and LC [9].
In conclusion, LC is a diagnostic challenge, and early diagnosis is essential to start chemotherapy treatment as soon as possible. The differential diagnosis arises with infectious processes (tuberculosis) and autoimmune diseases. If involvement by Lymphoma is suspected, FCM is more profitable than cytology and should be performed from the outset.

