Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
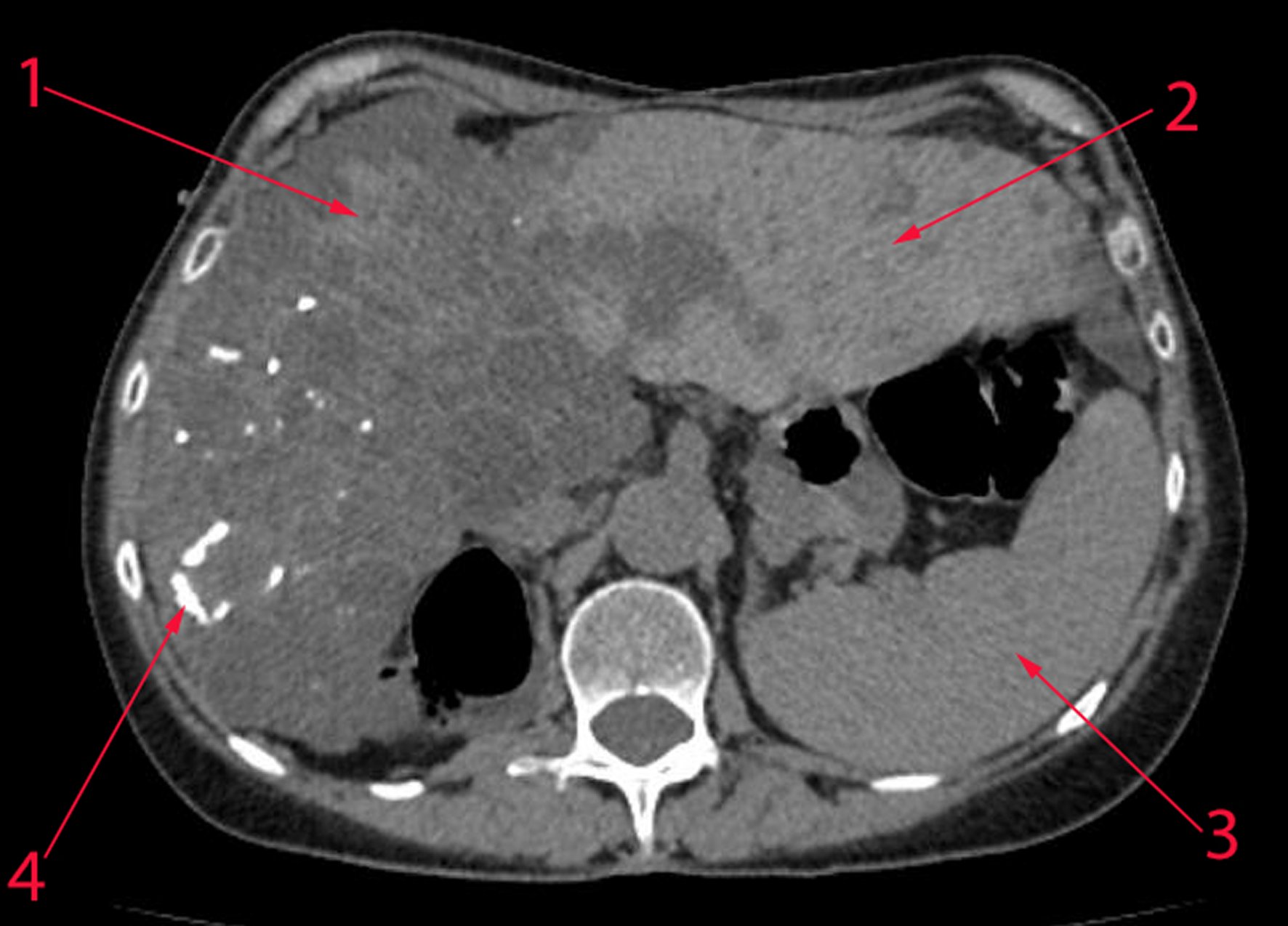
PermalinkA 54, year's old female patient was admitted to the clinic with sudden onset of abdominal pain in the epigastric and right hypogastric area followed by nausea. Her complete blood count was normal and biochemical analysis revealed mild elevation of liver enzymes (ALT – 49 u/L [normal range 8-40] AST – 45 u/L [normal range 5-42]). Abdominal USG revealed hepatomegaly with multiple cysts. The patient had a kidney transplant five years earlier due to terminal chronic renal failure caused by autosomal dominant polycystic kidney disease (ADPKD). Otherwise her medical history was unremarkable and the kidney function was not altered. A CT scan of the abdomen revealed multiple liver cysts that occupied most of the right lobe with areas of calcification (Figure 1). Calcification of liver cysts in polycystic liver disease is rare and is usually due to prior hemorrhage or infection [1]. The incidence of comorbidities in patients with ADPKD increases with age. Liver cysts are seen in 11-27% of patients younger than 30 and in 77-83% of patients over 60 with ADPKD. Enlargement of the cysts can lead to symptoms related to hepatomegaly. Some cysts can complicate with hemorrhage, infection or torsion thus requiring surgical treatment [2]. The most frequently used classification of liver cysts was proposed by Gigot and coworkers [3]. Gigot et al. proposed the classification as a stratification option to guide surgeons which operation to offer. Based on this classification there are three types of liver cyst: type I – less than 10 cysts, with a diameter more than 10 cm and a total affected zone less than 25%; type II – diffuse zone with multiple cysts that affect 25-50%; type III – large zone (>75%) is affected by small and medium cysts. Patients with first and second types should undergo aspiration and fenestration or partial resection of the liver [4]. The third type requires liver transplant [5]. The current case was managed conservatively with an improvement of laboratory parameters. Mild cases of polycystic liver disease should be managed conservatively especially in cases of exacerbation. If the symptoms persist the patient can undergo a planned intervention based on the cyst size, location and percent of liver parenchymal involvement.