










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
An injury to the spinal cord is a severe chronic neurological disorder. Spinal cord injury (SCI) is a devastating event that results in disability, limitations in participating in various activities, and mental health problems which greatly affects the quality of life of the injured person [1].
The world health organization (WHO) reports that the worldwide incidence of SCI ranges from 250,000 to 500,000 people every year [2]. The developed countries have an incidence rate of SCI 13.1 to 163.4 per million similarly incidence rate was 13 to 220 per million in the non-developed countries [3]. In Pakistan, it was reported that 90% of the people with SCI suffered from paraplegia while 10% were tetraplegia with the majority of the patients were males [4].
In the chronic stages of SCI in which the injury has lasted longer than 3 months many secondary complications like chronic pain, cardiovascular and respiratory complications, contractures, pressure ulcers, infections, bowel and bladder dysfunction and spasticity becomes a challenge for the patient and the health care community to manage due to which recovery will be complex and difficult. In some cases the worsening of the complications can lead to re-admission in hospitals and even can cause death if not properly treated [5].
The lowest levels of physical activity (PA) are among those who are living with SCI. The activity levels are even lower as compared to people with other chronic illnesses such as cancer and diabetes [6]. Physical inactivity and sedentary lifestyle causes many secondary health complications like cardiovascular and respiratory diseases in the general population however, this is especially true for chronic SCI patients [7]. Consequently, the major cause of mortality related to physical inactivity is cardiovascular disease in SCI patients [8]. Disability, depression, anxiety and confined to a wheelchair plays a key role in the inactive lifestyle of the individual with SCI [6]. A meta-analysis was conducted by Martin et al. reported that PA was related to low levels of depression among SCI patients [9]. Similarly, Ganesh et al. reported that there was low level of PA among paraplegic patients which affected there psychological well-being [10].
Depression is the most common psychological issue faced by SCI patients [10]. A study was done by Al-Owesie et al. in Riyadh, Saudi Arabia reported that depression was a major issue among SCI patients especially females [11]. Another study done by Khazaeipour et al. in Iran, reported that 49% of the individuals had mild to severe depression with depression being more common in women, people with tetraplegia, being cared for by their relatives, and individuals whose education level is low [12].
Depression is one of the major factor that delays physical therapy and exacerbates health issues. Furthermore secondary health complications related to SCI are aggravated by depression [13]. Since there is no cure for the treatment of SCI in the current clinical practice the patient’s psychological and social well-being is disturbed causing the patient to get anxious and depressed [14]. A longer stay in the hospital or rehabilitation centres, low quality of life, socially inactive, physical inactivity all are highly associated with depression [15]. Depression can increase the rehabilitation process needed for the recovery of the patient [16]. However, many doctors do not look into the issue of depression that surely affects the mental health problems of the individuals with numerous medical conditions thus resulting in many people committing suicide and dying every year [17].
The aim of this study was to find out the association of physical activity with depression among chronic spinal cord injury patients.
MATERIAL AND METHODS
The data collected from the participants were kept confidential, and the study protocol was approved by the Institute Ethical Committee (IEC), Northwest Institute of Health Sciences, Peshawar (Vide letter No. 02-11/12/NWIHS-COPT/IRB/2020).
It was a cross-sectional survey conducted at Paraplegic Centre Peshawar, Pakistan. The sample size was comprised of 109 subjects. Calculated by openepi.com version 3 with a 95% confidence interval. Non-Probability consecutive sampling was used to recruit the participants. Inclusion criteria included both gender were included, above 19 years of age, minimum 3 months since SCI, use of manual wheelchairs and walkers for primary mode of mobility and neurological impairment secondary to SCI (i.e., traumatic or atraumatic SCI). Participants with neurological level no greater than C5, known cases of Pregnancy, known cases of unstable cardiovascular diseases and known cases of cognitive deficits were excluded from this study. The PA levels were measured using Physical Activity Recall Assessment for People with Spinal Cord Injury (PARA-SCI) and depression was measured using the Centre for Epidemiological Depression Scale Revised 10-items (CESD-R-10).
For data analysis, version 25.0 of the Statistical Package for Social Sciences (SPSS) was used.
Mean age and standard deviation was calculated for numerical Data while categorical variables like gender, marital status, physical activity, and depression was presented in the form of percentages and frequencies. Data was presented in tables. A Chi-square test was used for categorical variables. p<0.05 was defined as statistically significant.
RESULTS
A total of 109 SCI patients participated in this research out of which 85 (78.0%) were male while 24 (22.0%) were female. 43 (39.4%) participants were 19-28 years of age, 30 (27.5%) had age from 29 to 38 years, 28 (25.7%) had the age of 39-48 years, and 8 (7.3%) were of 49-58 years of age. The mean age of participants was 33.97 ± 9.74 years. 80 (73.4%) of the participants had a normal body mass index (BMI) ratio, 11 (10.1%) were underweight, 18 (16.5%) were overweight. Out of the 109 participants 29 (26.6%) had some sort of business, 22 (20.2%) were labourers, 18 (16.5%) were housewives, and 14 (12.8%) were drivers. 69 (63.3%) of the patients were illiterate, and 4 (3.7%) had completed their education up to the secondary level. 79 (72.5%) of the patients had paraplegia and 30 (27.5%) had tetraplegia whereas 54 (49.5%) had ASIA B scale, 40 (36.7%) had ASIA A scale, 9 (8.3%) had ASIA C and 6 (5.5%) had ASIA D. The cause of SCI injury in 57 (52.3%) of the patients was fall from height, 27 (24.8%) was from road traffic accidents (RTA), and 25 (22.9%) had an injury because of gunshots. 90 (82.6%) of the participants had SCI since 3-13 months, 9 (8.3%) had SCI since 14-24 months, and 10 (9.2%) since 25-35 months. As shown below in Table 1.

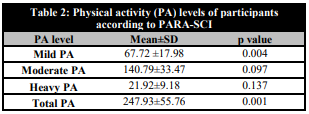
67 (61.5%) of the SCI patients out of n=109 were found having depression and 42 (38.5%) showed no sign of depression as measured by using the CESD-R-10 questionnaire. The depression mean was 11.94 ± 3.75. Table 2 presents the mean of participating in mild PA was 67.72 ± 17.98 minutes/week, moderate PA was 140.79 ± 33.47 minutes/week, heavy PA was 21.92 ± 9.18 minutes/week and total PA was 247.93 ± 55.76 among 109 participants. Additionally It also presents that p value was less than .005 concluding that mild PA and total PA was associated with depression whereas p value was greater than .005 concluding that moderate PA and heavy PA was not associated with depression.
DISCUSSION
To the best of our knowledge this is the first study being conducted in Peshawar, Pakistan which focused on the association of PA with depression among SCI patients using the PARA-SCI and CESD-R-10 scales. Few studies reported the association between PA and depression among the people with SCI. The main aim of our study was to determine the association of PA with depression among SCI patients at the paraplegic center Peshawar Pakistan. Our findings included that the mean participation in mild PA was 67.72 ± 17.98 minutes, moderate PA was 140.79 ± 33.47 minutes, heavy PA was 21.92 ± 9.18 minutes and total PA was 247.93 ± 55.76 on the PARA-SCI scale whereas depression was associated with performing mild PA, but moderate PA and heavy PA was not associated with depression. A study was conducted in Canada by Tawashy et al. reported that PA performed by the SCI patients with mild intensity resulted in a decrease in depressive symptoms [18] on the contrary our study showed opposite results concluding that mild PA was associated with depression while there was no association of depression with moderate and heavy intensity PA. Another cross-sectional study was done in Japan by Muraki et al. on 169 SCI patients which reported that SCI patients who participated in various types of PA had no association with depression compared to those who participated in less PA and inactive SCI patients [19] whereas the current study reported that mild PA performed was associated with depression. Our study stated that moderate PA performed per day by individuals with SCI was higher than mild PA and mild PA was performed more than heavy PA yet Perrier et al. in Canada reported that significantly more time (minutes)/day spend on mild intensity than moderate-intensity and more time (minutes) per day spend on moderate-intensity than high intensity [20].
A meta-analysis was conducted in Canada concluded that PA was related to low levels of depression among SCI patients [9]. Another study conducted in the United States of America by Rosenberg et al. on individuals with physical disabilities reported that there was small amount of association between PA and depression among people with different types of disability (SCI, multiple sclerosis, muscular dystrophy) [21]. Similarly a study was done by Mulroy et al. in the United States of America on patients with SCI concluding that PA was related to decrease in depression [22]. A cohort study was conducted by Gioia et al. in Italy on Italian SCI patients reporting that high PA participation resulted a decrease in depression as compared to inactive SCI patients [23]. The findings from these studies suggests that depression is associated with PA but the studies were limited because it did not measure the number of minutes performed by SCI patients on different intensities of physical activities. Our study measures the minutes and intensity of PA performed by the individual with SCI as well as associating it with depression showing that depression was associated with mild PA.
In this study participation in moderate PA was higher as compared to mild and heavy PA. Whereas a study was done in South Korea reported that mild PA performed by the SCI patients were higher than moderate and heavy PA Although the reports from this study also shows that slight depression was associated with PA but it did not associate depression with different intensity levels of PA [24]. A study was done by Ganesh et al. on paraplegia patients to find out about the PA levels in Odisha, India. The study reported that a low level of physical activity among paraplegia patients was associated with depression and mortality [10] the study was only conducted on paraplegic SCI patients whereas our study included both paraplegic and tetraplegic SCI patients. This study did not associate the different intensities of physical activities performed by the SCI patients with depression while the findings of our study were to associate depression with different levels of PA performed by the SCI patients.
CONCLUSIONS
Our study found out that there was association of depression with mild PA and total PA. The average minutes of participation in mild PA was 67.70 ± 18.91 minutes/week, moderate PA was 141.78 ± 33.22 minutes/week, heavy PA was 21.36 ± 9.67 minutes/week and total PA was 247.93 ± 55.76 minutes/week.
LIMITATIONS OF THE STUDY
There was only one rehabilitation center for SCI patients in Peshawar, Khyber Pakhtunkhwa. There were fewer females present with chronic SCI as compared to males because of which participation of males in this study was more as compared to females.

