










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkNutrición Hospitalaria
versão On-line ISSN 1699-5198versão impressa ISSN 0212-1611
Nutr. Hosp. vol.33 no.1 Madrid Jan./Fev. 2016
https://dx.doi.org/10.20960/nh.10
TRABAJO ORIGINAL / Pediatría
The most significant deficiencies in macro and micro nutrients in adolescents living with HIV/AIDS in antiretroviral therapy
Las deficiencias más significativas de macro y micro nutrientes en adolescentes que viven con el VIH/sida en terapia anti-retroviral
Fernanda Bissigo Pereira1, Fernanda Miraglia2, Caroline Barbosa Schmitz3, Carmem Lúcia Oliveira da Silva4 and Alexandre Ramos Lazzarotto5
1Master's Degree in Social Inclusion and Accessibility by FEEVALE University. Professor at the Nutrition Course of Serra Gaúcha School.
2Master's Degree in Nephrology and Doctor in Child and Adolescent Health by the Federal University of Rio Grande do Sul. Professor at the pre-graduation Course in Nutrition and of Masters in Human Health and Development. Centro Universitário La Salle. Brazil.
3Master's Degree student in Human Health and Development. Centro Universitário La Salle. Brazil.
4Master's Degree in Pediatrics. Hospital de Clinicas de Porto Alegre. Advisor for the Brazilian Health Ministry.
5Sciences of Human Movement. Federal University of Rio Grande do Sul. Professor of Masters in Health and Human Development. Centro Universitário La Salle. Brazil
ABSTRACT
Objective: To evaluate macro and micronutrients intake of adolescents living with HIV/AIDS in use of antiretroviral therapy and compare it to the Dietary Reference Intakes.
Methodology: Cross-sectional study conducted with adolescents of both genders with HIV/AIDS, assessing the dietary composition of macro and micronutrients, using the 24h dietary recall.
Results: 39 adolescents, average age of 15 years, 51.3% males. The participants intake of total calories, total fiber (g/d), liposoluble vitamins (A, D, E, K), vitamin B5 (mg/d), vitamin B9 (mg/d), vitamin C (mg/d), calcium (mg/d), phosphorus (mg/d), potassium (mg/d), and magnesium (mg/d) was lower than recommended. The percentages of intake lower than recommended were 79.5% for calories, 82.1% for total fibers, 89.7% for vitamin A, 100% for vitamin D, 87.2% for vitamin E, 100% for vitamin K, 71.8% for vitamin B5, 82.1% for vitamin B9, 76.9% for vitamin C, 92.3% for calcium, 61.5% for phosphorus, 97.4% for potassium, and 76.9% for magnesium. The participants ingested more carbohydrates (g), proteins (g), vitamins B2 (mg/d), B3 (mg/d), B8 (mg/d) and sodium (g/d) than recommended, the percentages above the recommendations being 92.3% for carbohydrates, 64.1% for proteins and vitamin B2, 56.4% for vitamin B3, 82.1% for vitamin B8, and 59% for sodium. The remaining nutrients were within the amounts recommended by the DRIs.
Conclusion: Food intake was inadequate as compared to the recommendations of the International Nutrition Guidelines.
Key words: HIV. ARV. Macronutrients. Micronutrients. Adolescents.
RESUMEN
Objetivo: identificar la ingestión alimentaria de macro y micronutrientes en adolescentes viviendo con VIH/sida que usan terapia anti-retroviral y compararlos a las Dietary Reference Intakes.
Metodología: estudio transversal realizado con adolescentes de ambos sexos con VIH/sida, en el que se evaluó la composición dietética de macro y micronutrientes a través del recordatorio alimentario de 24h.
Resultados: 39 adolescentes con una edad promedio de 15 años, un 51,3% del sexo masculino. Los participantes consumieron menos calorías totales en la dieta, fibra total (g/d), vitaminas liposolubles (A, D, E, K), vitamina B5 (mg/d), vitamina B9 (mg/d), vitamina C (mg/d), calcio (mg/d), fósforo (mg/d), potasio (mg/d) y magnesio (mg/d) que lo recomendado. Los porcentajes de ingestión por debajo de lo recomendado representaron el 79,5% para las calorías, el 82,1% para la fibra total, el 89,7% para la vitamina A, el 100% para la vitamina D, el 87,2% para la vitamina E, el 100% para la vitamina K, el 71,8% para la vitamina B5, el 82,1% para la vitamina B9, el 76,9% para la vitamina C, el 92,3% para el calcio, el 61,5% para el fósforo, el 97,4% para el potasio y el 76,9% para el magnesio. Los participantes consumían más carbohidratos (g), proteínas (g), vitaminas B2 (mg/d), B3 (mg/d), B8 (mg/d) y sodio (g/d) de lo recomendado, representando porcentajes por encima de la ingestión del 92,3% para los hidratos de carbono, del 64,1% para las proteínas y la vitamina B2, del 56,4% para la vitamina B3, del 82,1% para la vitamina B8 y del 59% para el sodio. Los demás nutrientes estaban dentro de lo recomendado por las DRIs.
Conclusión: el consumo alimentario fue inadecuado en comparación con lo recomendado por las Directrices Internacionales de Nutrición.
Palabras clave: Sida. TARV. Macronutrientes. Micronutrientes. Adolescentes.
Introduction
The development of combined antiretroviral therapy (ARVT), which rendered the important sustained suppression of viral replication, modified the clinical course of AIDS and its epidemic profile (1). The free and universal access to ARVT, established by the Brazilian government, caused a profound impact in the history of HIV infection, decreasing mortality and opportunistic infections, and had a consequent increase in the survival of carriers (2). According to the data from the Boletim Epidemiológico de 2014 (3), until October of that year, around 400 thousand people who live with HIV/AIDS (PVHA = PLWHA) had received ARVT for free from the Unified Health System (SUS) (4).
In Brazil there are approximately 20,000 adolescents living with HIV/AIDS, aged between 13 to 19 years. Only half of those are using ARVT (4).
The need for an appropriate approach by health professionals aiming at comprehensive attention to adolescents must consider the specific characteristics and subjective factors, sociocultural as well as demographic, confirming that care goes beyond the indication of treatment regimens and access to laboratory exams (4). The most important difficulties found in providing care for this group are: revealing the diagnosis, orphanhood, unstructured families and the initiation of sexual activity. Part of this group reaches adolescence exposed to many antiretroviral regimens, presenting a range of adverse effects, with few treatment options and the necessity to access to new drugs (5).
In HIV/AIDS carriers there is a high risk of malnourishment, even in the asymptomatic phases of the disease, since the virus generates changes in the demands of the nutritional status, such as protein catabolism, the risk increasing during the course of the infection (6). The importance of food and nutrition for people living with HIV/AIDS is so relevant that some authors advocate that it should receive the same attention as laboratory exams such as viral load and CD4 do, both for the characteristics of the HIV infection and for the possible adverse effects of antiretroviral medications (4).
There are evidences that people who live with HIV/AIDS and who have decreased serum levels of minerals and vitamins with immunomodulatory properties (vitamins C, A, B complex, selenium, zinc, and magnesium), present faster disease progression and higher mortality risk (7). The micronutrients are important to maintain healthy immunologic response and have been associated to the decrease in disease progression (5). It is important to emphasize that adolescence is that last moment of growth and development when nutritional demands are high as a consequence of the growth sprout, weight gain and sexual maturity (8).
Considering the current context of continuous use of ARVT in adolescents, there is a shortage of studies that approach their nutritional aspects. The objective of this study is therefore to identify the food intake of macro and micronutrients of adolescents living with HIV/AIDS in use of ARVT, and compare it to the Dietary Reference Intakes (DRIs).
Methods
Cross-sectional study conducted with adolescents from the HIV/AIDS Pediatric Ambulatory of the Hospital de Clinicas de Porto Alegre (HCPA)-Zona 4 with HIV/AIDS using ARVT. The consecutive sample comprised patients of both genders, from 14 to 18 years of age, with the diagnosis of HIV infection, using ARVT for at least three months. The study was approved by the Ethics in Research Committee of the Hospital de Clínicas de Porto Alegre (n 10-0584).
The variables collected from patients' medical records were: clinical (gender, age, time from HIV diagnosis, and current treatment regimen), virological (viral load), and immunological (TCD4+, TCD4+%, TCD8+, TCD8+% and TCD4+/TCD8+ ratio). The variables on diet (food and liquids) were collected by the researcher at the moment of the clinical visit talking to the adolescents and their tutors.
Food intakes were obtained by means of a 24-hours dietary recall adapted from Fisberg et al. (9). They were analyzed by DietWin Professional 2.0 2008 software for the calculation of diet. Energetic needs, macro and micronutrients were evaluated according to the recommendations of the Dietary Reference Intakes (DRI) (2005). The evaluation of total fat, saturated fat, and cholesterol intakes was based on the recommendations of the American Heart Association (AHA) that advocates 20%-30% of lipids for total energetic value, < 10% of saturated fat, and < 300 mg of cholesterol/day. For the macronutrients the values of 55%-60% of carbohydrates and 12%-15% of proteins were considered adequate. The energetic needs as well as the need for macro and micronutrients were then compared to the DRIs recommendations (14).
The continuous variables were described by medians (md) and the width of the interquartile range. The categorical variables were described by absolute and relative frequencies, and percentages.
The analyses were done using the SPSS® software (Statistical Package for the Social Sciences) version 18.0 (p<0.05).
Results
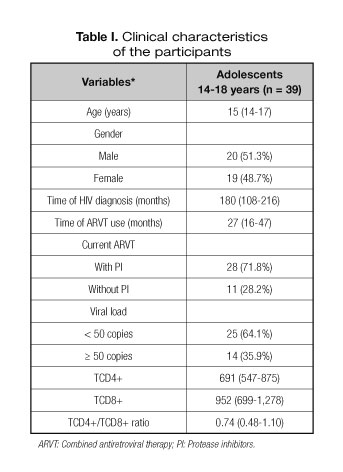
Participants were 39 adolescents of both genders, infected by vertical transmission. In spite of the mean time of diagnosis be longer than 10 years, the median time of ARVT use was a little longer than 24 months, with the predominance of protease inhibitors in the treatment regimen. Most subjects were clinically stable, with undetectable viral load (< 50 copies) and TCD4+ cells above 500. Table I depicts the clinical characteristics of the participants.
Tables II and III show food intake and DRIs recommendations. Participants ingested less total calories, total fiber (g/d) (Table II), liposoluble vitamins (A, D, E, K), vitamin B5 (mg/d), vitamin B9 (mg/d), vitamin C (mg/d), calcium (mg/d), phosphorus (mg/d), potassium (mg/d), and magnesium (mg/d) compared to the recommended amounts (Table III). The percentages of intake below recommendations were 79.5% for calories, 82.1% for total fiber, 89.7% for vitamin A, 100% for vitamin D, 87.2% for vitamin E, 100% for vitamin K, 71.8% for vitamin B5, 82.1% for vitamin B9, 76.9% for vitamin C, 92.3% for calcium, 61.5% for phosphorus, 97.4% for potassium, and 76.9% for magnesium.


The participants ingested more carbohydrates (g), proteins(g) (Table II), vitamins B2 (mg/d), B3 (mg/d), B8 (mg/d), and -sodium (g/d) (Table III) than the recommended amounts, the percentages above the recommendations being 92.3% for carbohydrates, 64.1% for proteins and vitamin B2, 56.4% for vitamin B3, 82.1% for vitamin B8, and 59% for sodium. The remaining nutrients were within DRIs recommendations.
Discussion
In this study, it was noted that the participants presented a diet intake below the recommendations for total energetic value, micronutrients and food fibers, and above the recommendations for macronutrients, demonstrating feeding standards similar to the Brazilian population (5) in the ingestion of carbohydrates and proteins, but with deficient food quality (8,11). Even though those adolescents were clinically stable, nutritional deficiency may have short term or medium term impact in immunity, musculature, and quality of life. In a study by Ziegler et al. (11) with a sample of young North American subjects, which compared food intake to DRIs recommendations, a low intake of micronutrients was also observed.
Some studies report abnormalities in the nutritional status of patients living with AIDS and the importance of adequate nutritional therapy, nutrient deficiency being one of the most important issues in those patients since they present poor food intake and bear metabolic modifications, such as increased protein catabolism (12).
The low intake of total fibers is consonant to the results by Werner et al. (13), where inadequate intake of this nutrient prevailed in subjects above 9 years of age. This fact may contribute to the concentration increase of serum cholesterol, because fibers have the capacity of binding to some substances, such as cholesterol, in the bowel, decreasing its absorption. Furthermore, the low intake of food fibers correlates to increased cardiovascular risk and to the development of colon cancer (14). Eating highly processed food as well as junk food that are rich in fat and sodium also contributes to a diet poor in food fibers and micronutrients (15).
A low intake of vitamin A was noted. Ferraz (16) reports that vitamin A deficiency intensifies the severity of diseases such as diarrhea and other infectious processes, and it may cause states of immunodeficiency of nutritional origin alone. Ziegler et al. (11) noted intake below DRIs recommendations after evaluating regular food intake in a population of North American subjects aged from 1 to 25 years.
Low intake of vitamins C and E was also noted. Maggini et al. (17) also report vitamins C and E deficiencies in patients with AIDS. It is well known that vitamin C acts as immunity-promoter along with vitamin E in the anti-oxidative process, being considered micronutrients necessary to maintain physiologic functions and body integrity (18). Vitamin C deficiency affects physical and mental growth in children in a negative way and may cause immune deficiencies (17).
Vitamins A, E and C are considered immune nutrients since they modulate the immunologic system, thus helping the body defense mechanism (19).
In this study we found a low intake of vitamin B9. Remacha (20) mentions that the low concentration of B12 and folate deficiency may be indicators of disease progression in HIV-infected subjects. Furthermore, it is known that the deficiency of vitamins B12 and B9 may cause megaloblastic anemia (21).
Vitamin D also showed intake values much lower than the ones considered adequate according to DRIs. It is known that vitamin D is related to the immune function and it may affect the progression of HIV infection. Its serum level depends on two factors: food intake and sun exposure. In addition, in the long run, if associated to low calcium intake it may impair bone health (21,22). This study did not evaluate the use of vitamin D supplementation.
Calcium intake as compared to the recommendations was deficient: skipping breakfast, something common in this age group (23), may contribute to the low intake of this micronutrient. It is known that calcium has an important role in adolescence, especially with regard to retention to form bone and in bone mineralization, involved in bone formation and skeleton preservation (24). A research in a population of teenagers living with AIDS also found low calcium intake, 60.4% of the subjects presenting low intake of that mineral (25). With positive adolescents of the city of Granada, Spain, the authors noted an intake higher than expected for the RDA for this age group among boys (22). Such differences may be attributed to different cultural eating habits.
Other nutrients as phosphorus, potassium and magnesium showed lower intake than recommended. Carter et al. (26) in a meta-analysis on the micronutrients in HIV noted that studies report that those micronutrients are supplemented in the diet, providing no information on their intake as food. Our work is among the pioneers in the approach to those micronutrients in food intake.
Sodium intake was high. A study conducted by Leitte (18) in Rio de Janeiro with HIV-infected adults noted that the subjects' diets were with high sodium content, with a percentage of 82% above recommendations, thus inadequate for the primary prevention of cardiovascular diseases. Goldstein (27) mentions that arterial hypertension is dependent on nutritional factors such as excessive sodium intake.
The results of this study point to relevant gaps for the planning of clinical and nutritional interventions in HIV/AIDS adolescents in use of ARVT.
Feeding has an important role in the immunologic system, since enough quantities of macro and micronutrients are necessary for its normal function (27); nevertheless, few studies have been conducted to evaluate the diets of adolescents with HIV/AIDS. The few existing studies reported inadequate diets (28,29). In this study we suggest that the macro and micronutrients deficiencies found may be associated to the lack of adequate nutritional information and counseling. Inadequate feeding is connected to the stimulation of excessive food amounts and inadequate quality. The possibility of nutritional counseling for the adolescents in regard to adequate food intake may correct feeding errors and decrease their deleterious effects (30).
Conclusion
The adolescents under study had inadequate food intake since they had a smaller amount of calories, total fiber, liposoluble vitamins, vitamins B5, B9, C, calcium, phosphorus, potassium and magnesium, and excessive sodium as compared to the Food-based International Dietary Guidelines. Considering that they carry a chronic disease and the increase in their life expectancy, the development of specific protocols that incorporate the clinical characteristics of the infection, pharmacotherapy and its adverse effects, as well as the cultural aspects of adolescence is a key issue. This is the first article to evaluate feeding habits in ARVT-using adolescents and stressing the importance of nutritional counseling.
References
1. Romancini JLH, Guariglia D, Nardo JN, Herold P, Pimentel GGA, Pupulin ART. Níveis de atividade física e alterações metabólicas em pessoas vivendo com HIV/AIDS. Rev Bras Med Esporte (serial on the Internet) 2012 Dec. (cited 2014 Nov 15); 18(6):356-60. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S151786922012000600001&lng=en. http://dx.doi.org/10.1590/S1517-86922012000600001. [ Links ]
2. Sprinz E, ALVES MD, Brites C. HIV-associated lipodystrophy: a review from a Brazilian perspective. Therapeutics and Clinical Risk Management 2014;10:559-66. [ Links ]
3. BRASIL. Ministério da Saúde. Secretaria de Atenção em Saúde. Departamento de Ações Programáticas Estratégicas. Diretrizes nacionais para a atenção integral à saúde de adolescentes e jovens na promoção, proteção e recuperação da saúde. Brasília, 2014. [ Links ]
4. Informe del ONUSIDA para el día internacional del SIDA 2013. [ Links ]
5. BRASIL. Ministério da Saúde. Secretaria de Atenção em Saúde. Departamento de Ações Programáticas Estratégicas. Diretrizes nacionais para a atenção integral à saúde de adolescentes e jovens na promoção, proteção e recuperação da saúde. Brasília; 2010. p. 46. [ Links ]
6. BRASIL. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. Recomendações para a Atenção Integral a Adolescentes e Jovens Vivendo com HIV/Aids. Ministério da Saúde; 2013. [ Links ]
7. Kruzich LA, Marquis GS, Carriquiry AL, Wilson CM, Stephensen CB. US youths in the early stages of HIV disease have low intakes of some micronutrients important for optimal immune function. J Am Diet Assoc 2004;104:1095-101. [ Links ]
8. Chiarelli G, Ulbrich AZ, Bertin RL. Composição corporal e consume alimentar de adolescentes da rede pública de ensino de Blumenau (Brasil). Rev. bras. Cineantropom. desempenho hum. V.13, n.4, jul/ago 2011. [ Links ]
9. Fisberg RM, Berzabeth S, Marchioni CML, Martini LA. Inquéritos alimentares métodos e bases científicas. São Paulo: Ed. Manole; 2005. [ Links ]
10. Taquette SR, Rodrigues AD O, Bortolotti LR. HIV infection in female adolescents: a qualitative study. Rev Panam Salud Publica 2015;37(4-5):324-9. [ Links ]
11. Ziegler TR, Mc Consey GA, Frediani Jk, Millson EC, Tangpricha V, Eckard AR. Habitual nutrient intake in HIV-infected youth and associations with HIV-related factors. AIDS Res hum retorviruses 2014;30(9):888-95. [ Links ]
12. Tanaka LF, Lactorre MRDO, da Silva AM, Konstantyner TCRO, Mendes EC, Marques HHS. Poor diet quality among Brazilian adolescents with HIV/AIDS. J Pediatr (Rio J) 2015;91(2):152-9. [ Links ]
13. Werner ML, Pone MV, Fonseca VM, Chaves CR. Lipodystrophy syndrome and cardiovascular risk factors in children and adolescents infected with HIV/AIDS receiving highly active antiretroviral therapy. J Pediatr (Rio J) 2010;86:27-32. [ Links ]
14. Denipote FG, Trindade EBSM, Burini RC. Probióticos e prebióticos na atenção primária do câncer de cólon. Arq Gastroenterol (São Paulo) 2010;47(1):93-98. [ Links ]
15. Zahedi, et al. Association between junk food consumption and mental health in a national sample of Iranian children and adolescents: the CASPIAN-IV study. Nutrition 2014;30(11-12):1391-7. [ Links ]
16. Ferraz IS, Daneluzzi JC, Vannucchi H, Jordão AA Jr, Ricco RG, Del Ciampo LA, et al. Prevalence of iron deficiency and its association with vitamin A deficiency in preschool children. J Pediatr (Rio J) 2005;81:169-74. [ Links ]
17. Maggini S, Wenzlaff S, Horing D. Essential role of vitamin C and zinc in child immunity and health. J Int Med Res 2010;38:386-414. [ Links ]
18. Leite LHM, Sampaio ABMM. Risco cardiovascular: marcadores antropométricos, clínicos e dietéticos em indivíduos infectados pelo HIV. Rev. Nutr., Campinas, jan./fev. 2011;24(1):79-88. [ Links ]
19. Remacha AF, Cadafalch J, Sardá P, Barceló M, Fuster M. Vitamin B metabolism in HIV-infected patients in the age of highly active antiretroviral therapy: role of homocysteine in assessing vitamin B12 status. Am J Clin Nutr 2003;77:420-4. [ Links ]
20. Romanelli F, Empey K, Pomeroy C. Macrocytosis as an indicator of medication zidovudine adherence in patients with HIV infection. AIDS Patient Care STDS 2002;16:405-11. [ Links ]
21. Stephensen CB, Marquis GS, Kruzich LA, Douglas SD, Aldrovandi GM, Wilson CM. Vit D status in adolescents and young adults with HIV infection. Am J Clin Nutr 2006;83(5):S 1135-1141. [ Links ]
22. Hirota T, Hirota K. Bone and nutrition: nutritional management of osteoporosis. Clin Calcium 2015;25(7):1049-55. [ Links ]
23. Bernheimer JM, Patten G, Makeleni T, Mantangana N, Dumile N, Goemaere E, Cox V. Pediatric HIV treatment failure: a silent epidemic. J Int AIDS Soc 2015;18(1):20090. DOI: 10.7448/IAS.18.1.20090. eCollection 2015. [ Links ]
24. Lima LRA, Silva RCR, Giuliano ICB, Sakuno T, Brincas SM, Carvalho AP. Bone mass in children and adolescents infected with human immunodeficiency virus. J Pediatr (Rio J) 2013;89(1):91-9. [ Links ]
25. Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, et al. Primary prevention of ischemic stroke: a guideline from the American Heart Association. American Stroke Association Stroke Council. Circulation 2006;113(24):873-923. [ Links ]
26. Carter GM, Indyk D, Johnson M, Andreae M, Suslov K, Busani S, Esmaeili A, Sacks HS. Micronutrients in HIV: A Bayesian Meta-analysis. PLoS ONE 2015;10(4):e0120113. [ Links ]
27. Werner ML, Pone MV, Fonseca VM, Chaves CR. Lipodystrophy syndrome and cardiovascular risk factors in children and adolescents infected with HIV/AIDS receiving highly active antiretroviral therapy. J Pediatr (Rio J) 2010;86:27-32. [ Links ]
28. Joint United Nations Programme on HIV/AIDS: UNAIDS.org . Global Report: UNAIDS report on the global AIDS epidemic 2012. Available at: www.unaids.org. [ Links ]
29. Miller TL. The next decade: cardiovascular risks, outcomes, prevention, and treatment in pediatric HIV infection. J Pediatr (Rio J) 2010;86(1):3-5. [ Links ]
30. BRASIL. Ministério da Saúde. Boletim Epidemiológico AIDS e DST 2012. Ano II - n.o 1 - até semana epidemiológica 26a - dezembro de 2012. [ Links ]
![]() Correspondence:
Correspondence:
Fernanda Miraglia
e-mail: fernandamiraglia@terra.com.br
Received: 12/09/2015
Accepted: 08/11/2015
