










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkNutrición Hospitalaria
On-line version ISSN 1699-5198Print version ISSN 0212-1611
Nutr. Hosp. vol.34 n.1 Madrid Jan./Feb. 2017
https://dx.doi.org/10.20960/nh.986
TRABAJO ORIGINAL / Valoración nutricional
Comparative analysis of height estimation methods in hospitalized adults and elders
Análisis comparativo de los métodos de estimación de altura en adultos y ancianos hospitalizados
Ana Paula Ferreira-Melo1, Raquel Kuerten de Salles1, Francilene Gracieli Kunradi Vieira2 and Marilyn Gonçalves Ferreira1
1Federal University of Santa Catarina. Department of Nutrition. Florianópolis, Santa Catarina. Brazil.
2Federal University of Santa Catarina. Post-Graduate Program in Nutrition. Florianópolis, Santa Catarina. Brazil
ABSTRACT
Introduction: Height is one of the measurements required for the assessment of body composition and for devising a nutritional plan for hospitalized patients. Due to the impossibility to measure the height of such patients in various situations, alternative estimation methods are necessary.
Objective: To compare the self-reported height and different height estimation methods with the real height of adults and elders hospitalized in a public teaching hospital of Santa Catarina.
Methods: The study subjects were 241 adults and elders of both genders. Real height (gold standard), recumbent height, knee height, arm length and demi-span were measured, as well as the self-reported height, which was recorded. Self-reported height and estimated height by different methods were compared to real height through a paired t-test and Bland-Altman analysis.
Results: The most accurate and concordant results were estimated through recumbent height, which was no statistically significant difference (p > 0.05) between real height and all study groups. The height obtained through a formula that uses arm length and demi-span and the self-reported height also had satisfactory results among certain groups. The formulae that uses knee height was the only one that resulted in underestmation of height for all study groups.
Conclusion: The height estimation method that stood out as the most accurate was recumbent height assessed with a stadiometer. The best results in this study were found with methods of easy applicability and low cost.
Key words: Anthropometry. Estimation techniques. Body height.
RESUMEN
Introducción: la altura es una de las medidas necesarias para la evaluación de la composición corporal y para la elaboración de un plan nutricional para pacientes internados. Debido a la imposibilidad de medir la altura de dichos pacientes en ciertas situaciones, los métodos de estimación alternativos se hacen necesarios.
Objetivo: comparar la altura informada y los diferentes métodos de estimación de la altura con la altura real de adultos y ancianos internados en un hospital universitario público de Santa Catarina.
Métodos: estudio de 241 adultos y ancianos de ambos sexos. La medición de la talla real (estándar oro), talla reclinada, altura de la rodilla, la longitud del brazo, la media brazada y talla informada. La autopercepción de talla y la estimada por diferentes métodos fueron comparadas con la altura real a través de una prueba "t" pareada y Bland-Altman análisis.
Resultados: los resultados más precisos y concordantes se obtuvieron a través de la talla reclinada sin diferencia significativa (p > 0,05) con la altura real para todos los grupos del estudio. La altura obtenida a través de una fórmula que utiliza la media brazada y la altura autoinformada también dio resultados satisfactorios en algunos grupos. La fórmula de la altura de la rodilla fue la única que quedó debajo de la altura real para todos los grupos.
Conclusiones: el método de medición de talla que se destacó como el más preciso fue altura reclinada tomada con un estadiómetro. Los mejores resultados en este estudio se encontraron con métodos de fácil aplicación y bajo costo.
Palabras clave: Antropometría. Técnicas de estimación. Estatura.
Introduction
Height is one of the measurements required for the assessment of an individual's body composition (1), since it is employed in the calculation of clinical and nutritional parameters such as the creatinine-height index (CHI), body surface area, basal energy expenditure and especially the body mass index (BMI). The latter is a frequently used parameter for the establishment of nutritional diagnosis, for the choice of therapeutic interventions and for monitoring the health status of individuals, especially hospitalized ones (2-4).
Monitoring anthropometric measurements can aid the prevention, control and treatment of several health issues (5). A study of 98 adult and elderly patients hospitalized has found a prevalence of malnutrition of 4,1% according to the BMI (6), which is a much lower prevalence than national data obtained through the Brazilian Survey of Hospital Evaluation (IBRANUTRI) from 1996, which evaluated 4,000 patients from public hospitals and revealed that 48% of them were malnourished (7).
It is worthy of note that the methods for nutritional status tracking invariably use the BMI, thereby making height measurement indispensable. Due to the impossibility to measure the height of inpatients in various situations, alternative estimation methods are necessary (2).
Self-reported height and predictive height formulas can be cited among the methods recommended by the literature to estimate stature. These estimations can be derived from isolated measurements of body parts or from the association of several anthropometric measurements, such as arm length (AL), knee height (KH), span or demi-span (DS) (8-13).
Considering the importance of height estimation in patients whose real height cannot be measured, this study aims to compare the real height of hospitalized patients (standard method) with their self-reported height, recumbent height (RH) and height estimated by the formulae of Chumlea et al. (8,9) and Rabito et al. (12).
The end purpose is, upon completion of this study, to suggest the methods that most accurately estimate height, which can thus be used specifically in adult and elderly bedridden patients admitted to the hospital where the research was conducted.
Material and methods
This in an analytical, quantitative, cross-sectional study, carried out in a general teaching hospital in the south of Brazil, between June and October 2013.
The study subjects were adults (20 to 60 years old) and elders (60 years old or more), of both genders, able to ambulate, admitted to the Internal Medicine and Surgery wards, who signed the informed consent form. Exclusion criteria were patients with amputated limbs, those with limb paralysis or those with cognitive impairment that would preclude self-reported data collection. Sample size was calculated using the SEstatNet (14) software. The number of patients considered for such were those admitted in medical and surgical clinics of the hospital in a period of five months (n = 2.400). The calculation resulted in a sample of 243 individuals, with a standard deviation of 10, sample error of 2 and 99.9% confidence level. The research was approved by the Ethics Committee for Research with Humans of the Federal University of Santa Catarina (UFSC) under the protocol number 1107/13. All the participants signed the informed consent form.
Identification and sociodemographic data and the anthropometric measurements necessary for the stature estimation methods analyzed were recorded by two of the researchers who were trained for data collection, rigorously following the study protocol. Data were entered into a protocol designed specifically for this study. The anthropometric evaluation included measurements of height, RH, KH, AL and DS. All measurements were made on the right side of the patients' bodies. The real height was measured with a Alturaexata® stadiometer of 2.00 meters, divided in centimetres and subdivided in millimetres, which was fixed to a wall without a footer, according to the standards recommended by Jelliffe (15).
RH was obtained with the help of the Alturaexata® stadiometer by measuring the distance between the top of the head and the sole of the foot of individuals lying on a stretcher in the supine position (13). KH was measured forming a 90 degree angle between the knee and the ankle of an individual in the supine position (16). A calliper rule with a 0.1 cm sensitivity was used, with a fixed part positioned on the sole of the patient's foot and a mobile part pressed against the patella. AL was measured with the patient in the orthostatic position, with the arm flexed alongside the torso, forming a 90 degree angle with the forearm, and the palm facing inward (17). A tape measure was used to quantify the distance between the superior edge of the acromion and the proximal end of the radium.
The DS was measured with the patient standing, in order to quantify the distance between the sternum and the distal phalanx of the middle finger, with the help of a flexible, inelastic tape measure that ran parallel to the clavicle (11). The height estimation formulae used in the present study are listed on table I. Patients were also asked whether they knew their stature. Those who did not offer a self-reported height were excluded only from this subset of the analysis, but maintained for the other comparisons. The database was built on Microsoft Excel® software. Statistical analysis was performed on the STATISTICA software version 7.0. All the variables were tested for normality of data with the Kolmogorov-Smirnov test. Since all variables were normally distributed, the paired t-test and the Bland and Altman (18) analysis were used to evaluate agreement, taking real height as the standard method with which were compared the others methods. In the Bland and Altman method the agreement is determined to compare the means of the results obtained by using each method and the limits of agreement are defined as the mean difference ± 1.96 SD and show to what extent the tested method varies compared to the standard method, with 95% of the differences falling within these limits. The mean difference between real height and self-reported height was verified according to age groups and years of education through analysis of variance (ANOVA). For all analyses, the significance level was p < 0.05.

Results
Among the individuals eligible for the study there was a loss of 66 subjects for refusal and 2 for missing data. The study subjects were 241 patients, of whom 117 (48.5%) were men and 124 (51.5%) were women. Among men, there were 71 adults (61%) and 46 elders (39%), whereas among women there were 88 adults (71%) and 36 elders (29%). The average age was 53-98 years among male subjects and 49-71 among females. Men had an average of 7-39 years of education, while women had 6-83 years. Adults of both genders had more years of education than the elderly (Table II). In the adult men group, there was no statistically significant difference (p > 0.05) between real height, RH and height estimated by Rabito et al. (12), which employs AL and DS. The aforementioned authors' formula which employs only DS and the formula developed by Chumlea et al. (8) resulted in underestimated heights, whereas self-reported height was significantly overestimated (Table III).
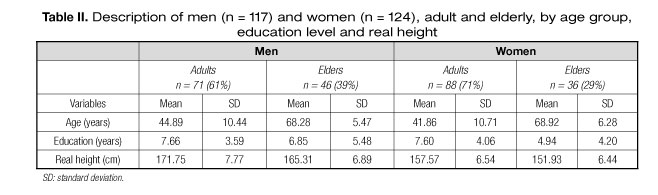

Table III also shows that, in the elderly men group, the only height estimation method that showed greater agreement and no difference to real stature was RH. All other methods disagreed significantly with real height by overestimating it, except that of Chumlea et al. (9), which resulted in underestimation. Therefore, the most accurate height estimation methods among men were RH, height estimated by the formulae of Rabito et al. (12) and self-reported height, the largest difference being 2.76 cm when employing one of the formulae of Rabito et. al. (12) in elderly men. Using the method of Chumlea et al. (8,9) resulted in significant underestimation as long as 8.04 cm. The only method to achieve values statistically similar and greater agreement to real stature among adult women was RH. There was significant overestimation with self-reported height and the height estimation formulae, except with that of Chumlea et al. (8), which resulted in underestimation of real stature (Table IV). In the elderly women group, there was no statistically significant difference between real height, self-reported height and RH. The remaining estimation techniques showed significant difference, once more by overestimating the patients' statures, except for that of Chumlea et al. (9), which resulted in underestimation (Table IV). Similarly to height estimation among men, the most accurate formulae among women were self-reported height and the formulae of Rabito et al. (12) (the largest difference was of 2.6 cm when employing one of Rabito et al. (12) formulae among elderly women). Other methods resulted in larger differences between estimated and real height, with the notable overestimation of 6.89 cm in the adult women group when using the formula of Chumlea et al. (8). The self-reported stature of adult women was more overestimated than that of elderly women. Regarding self-reported height, it was clear that 90.7% of men stated knowing their stature (comprising 89% of the adult men and 93% of the elderly men), while 73% of women reported their stature (comprising 82% of adult women and 53% of elderly women). As figure 1 shows, in both genders, the mean difference between real height and self-reported height was similar according to age groups and stratification by education years (p < 0.05).


Discussion
The subject composition of the present study was predominantly of adults, mostly of the female gender. This feature follows the characteristics of Brazilian population, of which women make up 51.5% and men, 48.5%, while people over 60 years old are a minority, amounting up to 12%. The average education levels of the study sample, of 6.8 years among women and 7.3 years among men, were also consistent with the national average, which is 7.3 years (19). Three of the height estimation methods assessed in this study did not show significant difference in relation to real height: RH for all groups; self-reported height for elderly women and height estimated by the formula of Rabito et al. (12) (which takes into account two variables for adult men). These were also the techniques that resulted in the smallest mean differences in relation to real height for all study groups. RH was the only method that was accurate and concordant in estimating the stature of adults and elders of both genders. This technique is widely used in clinical practice due to its ease of measurement and independence from specific equipment, since it is usually obtained with a tape measure (10). In this study, however, there was a choice for measuring RH with the aid of a stadiometer, equipment which is also usually available in hospital units for the assessment of stature. The goal was to verify whether the measurement precision achieved with the stadiometer would result in higher accuracy, considering that a previous study of 142 adults of both genders in the same hospital had observed significant overestimation of real height through measurements of RH in adult men and women with a tape measure, with an average difference of 3 cm (20). Luft et al. (13) developed an instrument similar to the stadiometer, called the Luft® ruler, and tested its utilization in a report akin to the present one. In this report, estimated height was also approximate to real height, but the lack of significant difference was only present among adult men. Among women and elderly men, there was statistical difference between estimated and measured stature. Despite the good results, attention must be paid to the fact that the assessment of this measurement may be compromised in the case of skeletal or joint deformities, when the patient cannot be positioned supine (21). Self-reported- height also resulted in a small mean difference in relation to real height, however the absence of significant difference was restricted to elderly women. All study groups showed a tendency towards overestimation, especially elderly men, where stature was overestimated by 1.72 cm.
The recommendation of using self-reported height when real height measurement is infeasible has been frequent in the literature (5,22-27). Nevertheless, many of these authors have found that self-reported height overestimated real height. This is thought to be associated with a desire for certain social patterns to be reached (28). Unlike the findings of Virtuoso Junior and Oliveira-Guerra (29) and Del Duca et al. (30), in which higher levels of education were associated with larger overestimation of stature, this study showed no such relations. Although the attainment of self-reported height is practical, one of the limitations of this method is that it requires people to know their own height. This study showed that approximately one third (27%) of women did not know this information, especially among elderly women (47%). On the other hand, the same group that denied knowing their height was the group that reported it most accurately. Some authors do not recommend the use of self-reported stature measurements for elderly individuals (30,31). The rationale is that, in ageing, there is a natural process of height reduction due to compression of intervertebral discs and reduction of the mineral content of the vertebrae. Possibly due to the lack of periodic assessments of stature, elderly individuals report information less precisely than young adults, since they use height measurements from their youth as a reference (30). Such a recommendation is not consistent with the results found in the present study regarding the self-reported height of elderly women. The findings of this study regarding the height estimation formulae developed by Rabito et al. (12), especially the one that employs AL and DS concomitantly, showed no significant difference to real height in adult men. Conversely, a survey by Souza et al. (32) of hospitalized elders in the south of Brazil has shown no significant difference between the real height and the height estimated by the formula of Rabito et al. (12) that uses DS individually. Rabito et al. (12) developed their equations based on a population similar to the sample of this study: hospitalized Brazilian adults and elders. Such similarity may have contributed to the positive results, given that when equations are applied to populations similar to the derivation sample, the difference between estimated and real height seems to be minimized. This fact is likely due to the ethnical and geographical influence on individuals' statures, as well as on the length of body segments according to ethnicity (32). There must be caution, however, in case the patient has upper limb deformities, since the variables in this equation are DS and/or AL.
Although the formulae of Chumlea et al. (8,9) are widely recommended by international literature and frequently used in clinical practice, the findings of this study do not support their use as first-choice height estimation methods, since both showed large differences in relation to real height. The formula of Chumlea et al. (8,9) underestimated real height by as much as 8.04 cm. Such differences may be associated with divergent characteristics between the populations, since these formulae were based on the American population. Differences this large may lead the professional to erroneous decisions regarding nutritional status assessment and diet prescription. However, these results were inconsistent with others which showed no significant difference between height estimated by Chumlea et al. (8,9) and real height (4,20,34,35).
Conclusion
The technique that stood out as the most accurate and concordant for all study groups was recumbent height assessed with a stadiometer, an instrument that enhanced the precision of the measurement, contributing to results that were better than those assessed with a tape measure, according to the original methodology described in a previous study.
It is noteworthy that the best results in this study were found with methods of easy applicability and low cost, which require only a stadiometer and a tape measure, appliances usually present in hospitals.
References
1. Canda A. Stature Estimation from Body Segment Lengths in Young Adults: Application to People with Physical Disabilities. J Physiol Anthropol 2009;28(2):71-82. [ Links ]
2. Beghetto MG, Luft CV, Mello ED, et al. Accuracy of nutritional assessment tools for predicting adverse hospital outcomes. Nutr Hosp 2009;24(1):56-62. [ Links ]
3. Brown JK, Feng JY, Knapp TR. Is Self-Reported Height or Arm Span a More Accurate Alternative Measure of Height? Clin Nurs Res 2002;11(4):417-32. [ Links ]
4. Rezende FAC, Rosado LEFPL, Franceschinni SCC, et al. Avaliação da aplicabilidade de formulas preditivas de peso e estatura em homens adultos. Rev Nutr 2009;22(4):443-51. [ Links ]
5. Castro V, Moraes SA, Freitas ICM. Concordância de medidas antropométricas em estudo epidemiológico de base populacional. Ribeirão Preto: Projeto OBEDIARP. Rev Bras Epidemiol 2010;13(1):58-68. [ Links ]
6. Scheunemann L, Wazlawik E, Bastos JL, et al. Agreement and association between the phase angle and parameters of nutritional status assessment in surgical patients. Nutr Hosp 2011;26(3):480-7. [ Links ]
7. Waitzberg DL, Caiaffa WT, Correia MI. Hospital malnutrition: the Brazilian national survey (IBRANUTRI): a study of 4000 patients. Nutrition 2001;17:573-80. [ Links ]
8. Chumlea WMC, Guo SS, Steinbaugh ML. Prediction of stature from knee height for black and white adults and children with application to mobility impaired or handicapped persons. J Am Diet Assoc 1994;94(12):1385-8. [ Links ]
9. Chumlea WMC, Guo SS, Wholihan KMS, et al. Stature prediction equa-tions for elderly non-hispanic white, non-hispanic black, and mexican-american person developed from NHANES III data. J Am Diet Assoc 1998;98(2):137-42. [ Links ]
10. Gray DS, Crider JB, Kelley C, et al. Accuracy of recumbent height measurement. J Parenter Enteral Nutr 1985;9(6):712-5. [ Links ]
11. Mitchell CO, Lipschitz DA. Arm length measurement as an alternative to height in nutritional assessment of the elderly. J Parenter Enteral Nutr 1982;6(3):226-9. [ Links ]
12. Rabito EI, Vannucchi GB, Suen VMM, et al. Weight and height prediction of immobilized patients. Rev Nutr 2006;19(6):655-61. [ Links ]
13. Luft VC, Beghetto MG, Castro SMJ, et al. Validation of a New Method Developed to Measure the Height of Adult Patients in Bed. Nutr Clin Pract 2008;23(4):424-8. [ Links ]
14. Nassar SM, Wronscki VR, Ohira M, et al. SEstatNet -Sistema Especialista para o Ensino de Estatística na Web. Florianópolis-SC, Brasil (2013 mar 04). Available from: http://www.sestat.net. [ Links ]
15. Jelliffe DB. The assessment of the nutritional status of the community. Geneva; 1966. (2013 mar 20). Available from: <http://www.ernaehrungsdenkwerkstatt.de/fileadmin/user_upload/EDWText/TextElemente/PHNTexte/WHO_FAO_Report/Jelliffe_Assessment_Buch_WHO_MONO_53_assessment_part1.pdf> [ Links ].
16. Chumlea WMC, Roche AF, Mukherjee D. Nutritional assessment of the elderly through anthropometry. Columbus (OH): Ross Laboratories; 1987. [ Links ]
17. Petroski EL. Antropometria: técnicas e padronizações. Porto Alegre: Palotti; 1999. [ Links ]
18. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307-10. [ Links ]
19. PNAD-Pesquisa Nacional Por Amostra De Domicílios. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística 2011;31:1-135. [ Links ]
20. Melo APF, Salles RK, Vieira FGK, et al. Análise comparativa de métodos de estimativa de peso e altura em adultos hospitalizados. Rev Bras Cineantropom Desempenho Hum 2014;16(4):475-84. [ Links ]
21. Mourrilhe C, Rosenblatt M, Coelho SC. Semiologia nutricional no doente grave. In: Duarte ACG. Avaliação nutricional: aspectos clínicos e laboratoriais. São Paulo: Atheneu 2007;20:285-8. [ Links ]
22. Dahl AK, Hassing LB, Fransson EI, et al. Agreement between self-reported and measured height, weight and body mass index in old age-a longitudinal study with 20 years of follow-up. Age Ageing 2010;39:445-51. [ Links ]
23. White MA, Masheb RM, Grilo CM. Accuracy of Self-reported Weight and Height in Binge Eating Disorder: Misreport Is Not Related to Psychological Factors. Obesity 2010;18(6):1266-9. [ Links ]
24. Lucca A, Moura EC. Validity and reliability of self-reported weight, height and body mass index from telephone interviews. Cad Saúde Pública 2010;26(1):110-22. [ Links ]
25. Peng S, Korda R, Clements M, et al. Validity of self-reported height and weight and derived body mass index in middle-aged and elderly individuals in Australia. Aust NZ J Public Health 2011;35(6):557-63. [ Links ]
26. Haverkort EB, Haan RJ, Binnekade JM, et al. Self-reporting of height and weight: valid and reliable identification of malnutrition in preoperative patients. The American Journal of Surgery 2012;20:700-7. [ Links ]
27. Fillenbaum GG, Kuchibhatla MN, Whitson HE, et al. Accuracy of Self-reported Height and Weight in a Community-Based Sample of Older African Americans and Whites. J Gerontol A Biol Sci Med Sci 2010;65(10):1123-9. [ Links ]
28. Gorber SC, Trembla YM, Moher D, et al. A comparison of direct vs. self report measures for assessing height, weight and body mass index: a systematic review. Obes Rev 2007;8:307-26. [ Links ]
29. Virtuoso-Júnior JS, Oliveira-Guerra R. Validade concorrente do peso e estatura auto-referidos no diagnóstico do estado nutricional em mulheres idosas. Rev salud pública 2010;12(1):71-81. [ Links ]
30. Del Duca GF, González-Chica DA, Santos JV, et al. Peso e altura autorreferidos para determinação do estado nutricional de adultos e idosos: validade e implicações em análises de dados. Cad Saúde Pública 2012;28(1):75-85. [ Links ]
31. Lee DH, Shin A, Kim J, et al. Validity of self-reported height and weight in a Korean population. J Epidemiol 2011;21(1):30-6. [ Links ]
32. Souza R, Fraga JS, Gottschall CBA, et al. Avaliação antropométrica em idosos: estimativas de peso e altura e concordância entre classificações de IMC. Rev Bras Geriatr Gerontol 2013;16(1):81-90. [ Links ]
33. Monteiro RSC, Cunha TRL, Santos MEN, et al. Estimativa de peso, altura e índice de massa corporal em adultos e idosos americanos: revisão. Com Ciências da Saúde 2009;20(4):341-50. [ Links ]
34. Cereda E, Bertoli S, Battezzati A. Height prediction formula for middle-aged (30-55y) Caucasians. Nutrition 2010;26(11-12):1075-81. [ Links ]
35. Yugue SF, Ide HW, Tiengo A. Comparação da avaliação antropométrica em pacientes internados por intermédio de métodos estimativos e diretos. Revista Ciências da Saúde 2011;1(3):1-10. [ Links ]
![]() Correspondence:
Correspondence:
Raquel Kuerten de Salles.
Departamento de Nutrição.
Centro de Ciências da Saúde.
Universidade Federal de Santa Catarina.
Campus Universitário Reitor João
David Ferreira Lima, s/n. Trindade.
88040-900 Florianópolis-SC.
Brazil
e-mail: raquel.k@ufsc.br
Received: 31/05/2016
Accepted: 25/11/2016
