










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
There is a high prevalence of depression in older adults, either clinically diagnosed or with a recognized depressive symptomatology, reportedly between 7 and 49% 1. Despite this incidence, it has been estimated that 70-90% of depression in old age is undiagnosed, misdiagnosed, or dismissed as a normal part of aging.
The objective is to increase the state of wellbeing and quality of life of the population, and especially the elderly. Quality of life is influenced by numerous factors, including certain food habits such as the consumption of fruits, vegetables, olive oil, fish and wine (in moderation), all distinguishing features of the Mediterranean diet, which has been associated with the ability to prevent cognitive deterioration, lower cardiovascular risk and decreased mortality from all causes 2. There is growing evidence that diet -a modifiable lifestyle factor- could be one component of an effective prevention strategy against depression, although no firm conclusion can be drawn at this point 3. A healthy Mediterranean dietary pattern appears to be associated with lower odds of depression and favourable mental and physical health outcomes 4. The Mediterranean dietary pattern refers not only to the type of food consumed, but also to lifestyle and the social customs associated with the way of eating. It therefore seems reasonable to assume that this pattern of healthy eating can modify cognitive status 4,5 and reduce the prevalence of depression in the elderly population 6.
There is a wealth of observations and experimental knowledge showing that effective brain function depends on an adequate and constant supply of nutrients, and that nutrition -particularly of micronutrients and ω-3 polyunsaturated fatty acids- is key for cognitive performance and mental wellbeing 7. The Mediterranean dietary pattern is rich in plant foods and fish. Plant foods have a high content in minerals, vitamins and natural antioxidants, and fish is a good source of ω-3 polyunsaturated fatty acids 2. The elderly population is at higher risk of receiving insufficient levels of these micronutrients that are essential for proper brain functioning, and whose deficiency negatively influences cognitive performance and is associated with age-related cognitive decline 5 and depressive symptoms 6.
Interest in old-age depression has increased due to the ageing population and the increasing demographic importance of elderly people. The study of these variables is interesting at any age, but it has a greater impact on the prevalence of morbidity and mortality when studied in older people. However, there are very few studies in the over-75 y.
OBJECTIVE
The aim of this study was to determine the adherence to the Mediterranean dietary pattern, and its protective role against cognitive decline and depression in a population aged over 75.
METHODS
STUDY DESIGN
A cross-sectional survey, the Garrucha Old Age Health Study, was conducted in very old men and women living in Garrucha (8,626 registered inhabitants), Almería (Spain), located on the Mediterranean coast. All non-institutionalised inhabitants aged 75 and over (n = 464) registered in the municipal census in 2014 were invited by letter delivered personally to participate in the study. The final sample comprised 79 participants (43 women and 36 men). Participants were divided into four age groups: 75-80; 81-85; 86-89; ≥ 90.
Data were collected by interview using comprehensive geriatric and nutritional assessment. Interviews were conducted by trained researchers. Informed written consent was obtained from all participants.
The study was the result of a collaboration agreement between the Universidad Complutense de Madrid (Madrid, Spain) and the Garrucha City Council (Almería, Spain), and conducted according to Declaration of Helsinki guidelines. All procedures were approved by the Ethics Review Board of the Universidad Complutense de Madrid.
FOOD CONSUMPTION
Food consumption data were collected by trained dietitians using three non-consecutive 24-hour diet recalls collected in face to face. In some cases, caregiver assistance was necessary to confirm the correct intake pattern. From three 24-hour diet recalls was calculated the grams of food per day and per person, and subsequently grams were transformed to serving according to recommendations of the food pyramid of Mediterranean diet 8.
ADHERENCE TO THE MEDITERRANEAN DIET
Adherence to the Mediterranean diet was determined by the MEDAS that was developed in PREDIMED study 9. A face-to-face interview with each participant was conducted to complete a questionnaire consisting of 14 questions. The 14-item screener of MEDAS includes 12 items with targets for food consumption and another two items with targets for food intake habits characteristics of the Mediterranean diet focused to know if the surveyed consumes olive oil and if so, to know the amount daily ingested.
Each question was scored 0 or 1. One point was given for each target achieved. One point was given for using olive oil as the principal source of fat for cooking, preferring white meat over red meat, or for consuming: a) four or more tablespoons (1 tablespoon = 13.5 g) of olive oil/d (including that used in frying, salads, meals eaten away from home, etc.); b) two or more servings of vegetables/day; c) three or more pieces of fruit/day; d) < 1 serving of red meat or sausages/day; e) < 1 serving of animal fat/day; f) < 1 cup (1 cup = 100 mL) of sugar-sweetened beverages/day; g) seven or more servings of red wine/week; h) three or more servings of legumes/week; i) three or more servings of fish/week; j) fewer than two commercial pastries/week; k) three or more servings of nuts/week; or l) two or more servings/week of a dish with a traditional sauce of tomatoes, garlic, onion, or leeks sautéed in olive oil. If the condition was not met, 0 points were recorded for the category. The total MEDAS score ranges from 0 to 14, with a higher score indicating better Mediterranean diet accordance. MEDAS score ≥ 7 (mid-range value) represented a modest accordance, and a score ≥ 9 represented strict accordance with the healthy dietary pattern 10.
COGNITIVE STATUS
Cognitive status was evaluated using the Mini-Mental State Examination (MMSE) 11, which is used for screening for mild cognitive impairment. It consists of a series of questions grouped into six categories that represent significant aspects of intellectual function: time-space orientation, memory loss and attachment, attention, calculation, capacity for abstraction, language and praxis (naming, repetition, reading, order, graphics and copy). A maximum of 35 points is awarded. Scores below 24 indicate cognitive limitations. Participants with a physical or mental disability that prevented them performing the tests were excluded.
DEPRESSIVE SYMPTOMS
Depressive symptoms were evaluated using the short version of the Geriatric Depression Scale (GDS) 12. The GDS was used to screen for any elements of depression. This scale was developed to assess many of the problems associated with depression, and to identify depressive symptoms in older adults (life outlook, mood, feelings of abandonment, predisposition for activities, fear of disease and death). Total scores were obtained by adding one point for each response which was symptomatic of depression, giving a score range of 0-15. This score was then classified into three categories of affective state: no depression (0-5), slight depression (6-9) and severe depression (> 9). Participants with a physical or mental disability that prevented them performing the tests were excluded.
OTHER MEASUREMENTS
The baseline examination included other questionnaires designed to collect information on leisure time physical activity, body mass index (BMI), health conditions, smoking habits, history of illness, use of medication, and educational level.
Statistical analysis
A descriptive analysis was conducted on the frequencies, averages and percentages of the population segmented by sex and age groups. The results were stratified into categorical variables as the scoring criteria for each determination. The results for the categories were compared using contingency tables. Differences between categorical variables were analysed with the Chi-square Pearson test. The average score in each category in terms of sex and age was compared using analysis of variance (ANOVA). p-values ≤ 0.05 were considered statistically significant. V22 SPSS statistical software was used for data analysis and processing.
RESULTS
The characteristics of the participants are shown in table I. The dispersion of data was very high and the differences between men and women were not significant in most of the parameters measured. However, there were significant differences in physical activity, and women showed poorer outcomes than men.
The mean age of the subjects in the study was 81.0 ± 4.6 years, with the most numerous group aged between 75 and 80. Most of population had a primary education level, less six diseases, a daily consumption of less five drugs and they were non-smokers, only one subject was smoker. The mean BMI was 27.9 ± 4.1 kg/m2. They had a moderate level of physical activity, with an average of over 69 minutes of activity a day, particularly walking, cycling, swimming and gymnastics adapted to the elderly (Table I).
Table I Characteristics of study populationaa

a. Values were expressed as mean ± standard deviation and number of subject and percentage respect to total sample, n(%). b. ANOVA and Chi-square Pearson test, p ≤ 0.05 corresponds to significant differences between women and men.
Regarding food consumption, most subjects routinely used olive oil for cooking and salads and frequently ate fresh fish.
Table II shows the percentage of senior citizens who met the MEDAS targets and adhere to the Mediterranean diet. All the participants used olive oil as their main cooking fat, almost 90% met the targets for using olive oil as their frying fat, and 94.9% consumed dished seasoned with tomato sauce, onion or leek with olive oil. The majority met the target for low consumption of red meat (92.4%), carbonated/sweetened beverages (79.7%), animal fat (77.2%), and commercial sweets and pastries (62%). In addition, more than 69% of the sample consumed more than three servings of fish per week. The population tended to consume vegetables, fruits and legumes. In contrast, consumption of wine and nuts was low. Less than 21% of individuals meet the targets.
Table II Participants who achieve each target of the MEDASa score, and accordance of food consumption with the Mediterranean dietb

a. MEDAS, Mediterranean Diet Adherence Screener. b. Accordance of food consumption with Mediterranean diet is defined as achieving ≥ 9 targets of MEDAS 10.
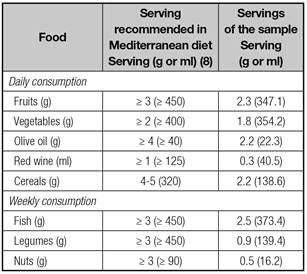
Table III shows the relationship between consumption of foods of the study population and their adherence to the Mediterranean dietary pattern. Study population consumed similar serving of fruit, vegetables, and fish corresponding with the serving recommended of the food pyramid of Mediterranean Diet (Table III).
The mean MEDAS score was 9.4 ± 1.6, denoting strict adherence to the Mediterranean diet. 69.6% of individuals attained a MEDAS score of over 9, while 27.9% had a MEDAS score of 7 to 8, representing modest adherence to the Mediterranean diet. Only 2.5% showed values of low adherence to the Mediterranean diet pattern. No differences were found due to sex but there were significant differences due age. Group aged over 90 showed a lower MEDAS (8.3 ± 1.2) (Table IV).
Tabla IV Adherence to Mediterranean diet, cognitive status and depressive symptoms of a population over 75 year

a. Data are presented as mean ± standard deviation; MEDAS (Mediterranean Diet Adherence Screener); MMSE (Mini-Mental State Examination); GDS (Geriatric Depression Scale). b. ANOVA; p ≤ 0.05 were considered to be statistically significant. cChi-square Pearson test; p ≤ 0.05 were considered to be statistically significant.
MMSE values were high for all participants, especially for men and subjects aged over 90. Significant gender differences were not found. 87.5% of people -especially men- showed no cognitive limitations, while 9.7% of women and 2.8% of men had cognitive limitations (Table IV).
The number of individuals with cognitive problems increased with age. It is worth noting that no cognitive limitation was detected in the group aged over 90, although this result is only indicative and cannot be generalized, as there were few participants in the study.
The average value of GDS indicated that the population had no depressive problems. No differences due to sex and age were found. Seventy-five per cent of population showed no depressive problems. However, 23.6% of study population showed symptoms of slight depression (15.3% women and 8.3% men). Only 1.4% reached values of severe depression. In terms of age, the group aged 81-85 years presented slightly higher values than the other age groups (Table IV).
We studied the relation between MMSE and GDS values with the three categories of degree of adherence to the Mediterranean diet: low degree of adherence (MEDAS score < 6), moderate degree of adherence (MEDAS score 7-8) and strict adherence (MEDAS score > 9) (Table V). As the degree of adherence rose, the percentage of individuals that had no cognitive limitations also increased, p < 0.05.
Table V Distribution of cognitive status and depressive symptoms according to the Mediterranean Diet Adherence Screener (MEDAS)

a. MEDAS SCORE: low (≤ 6), medium 7-8, high (≥ 9). b. Chi-square Pearson test, p ≤ 0.05 were considered to be statistically significant.
In terms of depression, it was observed that none of the subjects suffered severe depression; a few individuals had values indicating mild depression, but these do not appear to be related to the quality of the diet.
DISCUSSION
The Mediterranean diet is an eating pattern that is culturally rooted and transmitted by eating habits learned from previous generations. The older population have followed these customs throughout their lives and been less influenced by the Westernization of their diet. This may be an important reason to explain the high MEDAS score found in this population, when currently the score for the Spanish population stands at around 6.3 9. León-Muñoz et al. 9 considered that the MEDAS score using cutoffs > 9 defines a strict adherence to the Mediterranean diet, while the use of cutoffs > 7 denotes a modest adherence. The elderly population in the study had very high mean MEDAS scores (> 9). However, the results were quite different when the cutoff used in the MEDAS was modified to 7. It is interesting to note that some results observed in the answers to the 14 MEDAS questions may not reflect the real situation. For example, only 41.8% of older people met the goal of consuming legumes at least three times a week. However, the more detailed answers on food consumption indicated that most of the population frequently consumed legumes (twice a week). A similar situation occurred with the results for wine consumption. Most participants considered wine consumption to be beneficial for the health and had routinely consumed wine throughout their adult lives. However, they had abandoned or reduced their intake in recent years due to the greater prevalence of disease and the increased necessity of consuming medicines, some of which interacted with alcohol. In both examples it can be said that the consumption of legumes and wine were two eating habits that were deeply-rooted in this population.
In summary, oldest people still adhere to the main features of the Mediterranean diet pattern, such as high consumption of olive oil as the main source of fat, a high consumption of fish, low glycemic fruits and foods with added sugars, a moderate wine intake, and low consumption of red meat.
Cognition involves a variety of domains, and age-related decline varies considerably across these cognitive domains and between individuals. The cognitive functions that are most affected by ageing -independently of Alzheimer's and other dementias- often relate to attention, memory, perception, and executive function 13. Most of the population studied did not present cognitive limitations evaluated with the MMSE. These results were similar 14 -and in some cases higher 15,16,17 - to those found in other studies. It is worth noting that the over 90y were the age group without cognitive limitations. Similar results were found in the Octabaix study 14 .
The population study had no depressive problems measured with the GDS. Depression during aging is an important public health problem, and causes suffering to many who go undiagnosed 6. Often neither the elderly themselves nor the healthcare providers recognize the symptoms in the context of the multiple physical problems affecting many elderly people 6. Certain depressive symptoms like low mood may be less prominent than others such as loss of appetite, sleeplessness, lost of interest and so on. Studies of depressed adults report that those with depressive symptoms -with or without a depressive disorder- have poorer functioning than non-depressed adults, and could function similarly to or worse than adults with chronic medical conditions 6,18. Depression is common in later life, but methodological differences between studies preclude firm conclusions about cross-cultural and geographic variation 19.
Depression, decline in cognitive function and problems in nutritional status are common in aging 19. In this study of the relationship between cognitive status and depressive symptoms and the degree of adherence to the Mediterranean diet pattern, we observed that the cognitive function and quality of the diet were positively related. However, no relation was observed with the depressive symptomatology.
Numerous studies have found a relationship between reduced cognitive decline 20 and lower risk of clinical depression with a greater adherence to the Mediterranean diet 18 and a higher quality of life 21. Skarupski et al. 6 reported that greater consumption of the characteristic food groups in a Mediterranean-based diet was associated with a lower likelihood of depressive symptoms in older adults over time. Diet influences the physiological processes that may be involved in the development of depression in different ways, such as inflammation, oxidative stress or hormonal factors 6. In contrast to several other non-communicable diseases, the preventive potential of diet in regard to depression is a relatively new research area 5. A recent review study 3 determines that dietary patterns may have an influence on the onset of depression, although the relationship is unclear.
The possible role of lifestyle-related factors has been proposed for age-related changes in cognitive function, pre-dementia syndromes and cognitive decline of degenerative or vascular origin. Among these factors, the type of diet (amount and type of food) and the socio-cultural habits related to eating habits could be important in the impairment of the cognitive and affective state 19. Féart et al. 2 reported that stricter adherence to a Mediterranean diet was associated with slower MMSE cognitive decline, but not consistently with other cognitive tests; and not with risk for incident dementia 2.
The Mediterranean diet combines several foods and micro- and macronutrients already proposed separately as potential protective factors against dementia and pre-dementia syndromes. The Mediterranean diet can be linked to mental health outcomes via a high number of dietary constituents such as B-vitamins, antioxidants (nutrients and bioactive compounds) and fat composition -namely a high content in unsaturated fatty acids (mono- and poly-). Several foods such as legumes, nuts and fish are important contributors to polyunsaturated fatty acids, which may be involved in the neurodegenerative process 22-24. A clear reduction of risk for cognitive decline has been found in population samples with elevated fish and olive oil consumption and a high intake of monounsaturated and polyunsaturated fatty acids, but not when the disease has already taken over 7.
Epidemiological studies indicate a higher risk of cognitive decline in people with low ω-3 fatty acid intake, although the available evidence does not prove that polyunsaturated fatty acid supplements can protect against cognitive decline or dementia 25. These issues still require clarification. Nonetheless, there is much experimental evidence pointing to the beneficial role of consuming ω-3 fatty acids on the development of cognitive and emotional impairment.
Legumes, vegetables and fruits are an important source of vitamins and natural antioxidants. The limited epidemiological evidence available on fruit and vegetable consumption and cognition has generally highlighted the protective role of these foods against cognitive decline and dementia.
In summary, most people of this elderly group showed a very high adherence to the Mediterranean diet pattern, and did not present cognitive limitations. According to this study dietary habits appeared to be related with cognitive limitations but not with depressive symptomatology; however, efforts to decrease the prevalence of depression in the elderly should target risk factors. Prevention appears to require improvements in physical activity, diet and other lifestyle factors. The Mediterranean diet pattern includes a balanced combination of foods and a healthy lifestyle that positively affects the quality of life of the elderly.

