










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkNutrición Hospitalaria
versão On-line ISSN 1699-5198versão impressa ISSN 0212-1611
Nutr. Hosp. vol.34 no.6 Madrid Nov./Dez. 2017
https://dx.doi.org/10.20960/nh.1097
Prevalence of hypovitaminosis D and associated factors in adolescent students of a capital of northeastern Brazil
Prevalencia de hipovitaminosis D y factores asociados en adolescentes de una ciudad capital del noroeste de Brasil
Eduarda Pontes dos Santos Araújo, Dayanna Joyce Marques Queiroz, Juliana Padilha Ramos Neves, Lavoisiana Mateus de Lacerda, Maria da Conceição Rodrigues Gonçalves and Alice Teles de Carvalho
Postgraduate Program in Nutrition Sciences. Federal University of Paraíba. João Pessoa. Paraíba, Brazil
ABSTRACT
Background: Hypovitaminosis D is a frequent problem in the world and can be influenced by several factors.
Objective: To estimate the prevalence of hypovitaminosis D and associated factors in adolescent students of a capital city of northeastern Brazil.
Methods: Cross-sectional epidemiological study assessing 220 school adolescents of both sexes aged 15 to 19 years. A questionnaire was applied to assess sociodemographic (skin color, mother's education and receiving social benefits) and behavioral data (number of hours of sleep per day, sun exposure, physical activity and dietary vitamin D intake). Anthropometric nutritional status was assessed by BMI (body mass index) for age. Serum 25 (OH) D concentrations, PTH and serum calcium were measured by blood samples. We identified individuals with hypovitaminosis D as those with 25 (OH) D < 30 ng/dL. The analysis of factors associated with hypovitaminosis D was performed by simple and multivariate Poisson Regression.
Results: The prevalence of hypovitaminosis D was 57.3%. The female population had a significantly higher prevalence than the male. In the final adjusted model, the variable independently associated with hypovitaminosis D in females was the lowest serum calcium concentrations, and for males it was BMI, in which adolescents who had overweight/obesity were 2.4 times more likely to have hypovitaminosis D than the eutrophic ones.
Conclusions: The present study found a high prevalence of hypovitaminosis D in the analyzed population, especially in female adolescents. In addition, the factors independently associated with hypovitaminosis D were found to be overweight/obese in boys and low calcium concentrations in girls.
Key words: Vitamin D. Teen health. School health.
RESUMEN
Introducción: la hipovitaminosis D es un problema frecuente en el mundo y puede verse influenciada por varios factores.
Objetivo: estimar la prevalencia de hipovitaminosis D y factores asociados en adolescentes de una ciudad capital del noreste de Brasil.
Métodos: estudio epidemiológico transversal que evaluó a 220 adolescentes de ambos sexos de 15 a 19 años de edad. Se aplicó un cuestionario para evaluar los datos sociodemográficos y de comportamiento. El estado nutricional antropométrico fue evaluado por IMC para la edad. Las concentraciones séricas de 25 (OH) D, PTH y calcio en suero se midieron mediante muestras de sangre. Se identificaron individuos con hipovitaminosis D como aquellos con 25 (OH) D < 30 ng/dl. El análisis de factores asociados con la hipovitaminosis D se realizó mediante Regresión de Poisson simple y multivariante.
Resultados: la prevalencia de hipovitaminosis D fue del 57,3%. La población femenina tenía una prevalencia significativamente mayor que la masculina. En el modelo ajustado final, la variable independientemente asociada con la hipovitaminosis D en las mujeres fue la más baja de las concentraciones séricas de calcio, y para los hombres fue el IMC, en el que los adolescentes con sobrepeso/obesidad tenían 2,4 veces más probabilidades de tener hipovitaminosis que los eutróficos.
Conclusiones: el presente estudio encontró una alta prevalencia de hipovitaminosis D en la población analizada, especialmente en adolescentes. Además, se encontró que los factores asociados de forma independiente con la hipovitaminosis D fueron el sobrepeso/obesidad en los niños y concentraciones bajas de calcio en las niñas.
Palabras clave: Vitamina D. Salud adolescente. Salud escolar.
INTRODUCTION
Vitamin D plays an essential role in regulating body levels of calcium and phosphorus, growth and maintenance of bone remodeling (1), which are particularly important processes in childhood and adolescence. However, in recent years this vitamin deficiency has been linked to the pathogenesis of several chronic conditions such as metabolic syndrome, type 2 diabetes, hypertension, obesity, increased risk of cardiovascular disease, autoimmune diseases and cancer (2,3).
The scientific literature has reported high prevalence of hypovitaminosis D in the world, not only in vulnerable individuals, such as older adults and postmenopausal women (4,5), but also reaching children and adolescents (6). Only three studies in Brazil working specifically with adolescents were identified, showing a prevalence above 60% for hypovitaminosis D in adolescents in the south and southeast regions of the country (7-9).
Several factors may be associated with the presence of hypovitaminosis D in the population, among which sun exposure appears to be the main influencer of serum concentrations of this metabolite (10). However, some scientific findings have shown high prevalence of hypovitaminosis D in coastal regions that have high solar incidence (11). Furthermore, significant evidences also relates this phenomenon to behavioral, dietary and genetic factors, since, in regions of high sun exposure, habits such as excessive sunscreen use, low consumption of dietary sources of vitamin D, or the genetic predisposition of individuals could contribute to the increase of hypovitaminosis D in these places (12,13).
The northeastern Brazil presents stronger sun exposure for much of the year than regions already studied, which could favor positively maintaining serum concentrations of vitamin D. On the other hand, it has specific characteristics like the social and economic determinants of population (low human development index and access to financial resources) and that can contribute to the increased prevalence of vitamin D deficiency in the local population.
Thus, besides the need for more population-based studies on the nutritional status of vitamin D in adolescents, it is necessary to investigate the main related factors to identify strategies that can reduce the susceptibility of this population to various diseases in adulthood. Thus, this study aimed to estimate the prevalence of hypovitaminosis D and associated factors in adolescent students in a capital city of northeastern Brazil.
METHODS
Study design, population and sample
A cross-sectional epidemiological study was conducted involving teenagers from 15 to 19 years old enrolled in public schools in João Pessoa-PB, a metropolitan city in northeastern Brazil, held between June and August 2015. The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were submitted to and approved by the Health Sciences Center Committee of Ethics and Research of the Federal University of Paraíba (CCS / UFPB) in compliance with Resolution 466/12 of the National Health Council (CAAE 43097115.2.0000.5188). All participants and their guardians were informed about the purposes of the study and signed the free informed consent form, respectively.
The program OpenEpi (www.openepi.com) was used to define the sample size, considering the prevalence of 60% hypovitaminosis D found by Peters et al. (8), with a margin of error of 10% and a significance level of 5%. The drawing effect was corrected by multiplying by a factor of 2.1, with a total minimum of 194 adolescents and a margin of around 10% for possible losses. In all, 229 adolescents were recruited. However, nine participants did not meet the inclusion criteria or did not complete all stages of the study, totaling a final sample of 220 individuals.
Stratified sampling was conducted with a minimum of 10% of the 32 public schools in the city of João Pessoa, totaling four institutions, distributed in different regions to ensure greater randomness of the sample was performed. After the groups were drawn, three classes were randomly selected from each school, where all the teenagers in the age group of the study were invited to participate, thus 12 classes were part of the study.
Adolescents aged 15 to 19 years of both genders, and adolescents who had already had their menarche or had grown facial hair (according to gender) were included in the sample. All participants were classified in the post-pubertal stage. The following were considered as exclusion criteria: pregnant adolescents, nursing mothers, those using supplements or medications that contained or interfere with the metabolism of vitamin D, patients with chronic diseases (diabetes, hypertension, chronic kidney disease) and chronic alcoholics or smokers. Additionally, renal and hepatic function was also evaluated through specific laboratory tests (urea, creatinine, uric acid, alanine transaminase and aspartate aminotransferase) for purposes of selecting individuals in order to identify possible abnormalities.
Data collecting
Sociodemographic and behavioral data were collected through a semi-structured questionnaire. The sociodemographic variables included age, gender and skin color (self-reported) (14), if receiving social government benefits and maternal education (as indirect indicators of socioeconomic status of participants). Behavioral variables covered hours of sleep per day, daily sun exposure being higher or lower than 30 minutes (7,15), practice of physical activity while being exposed to the sun, performing physical activity or inactivity and habitual dietary intake of vitamin D.
The anthropometric evaluation measurements followed the recommendations of the Anthropometric Standardization Reference Manual (16). Adolescents were weighed on a digital scale (BAL-20 PM model) with a capacity of 150 kg and range of 100 g, and height was measured by a metal rod vertical stadiometer with capacity height of 2.04 m and sensitivity of 0.5 cm. All measurements were performed by trained examiners in duplicate. Weight and height measures made it possible to calculate the body mass index (BMI) and the determination of the anthropometric nutritional status was classified according to the World Health Organization curves (BMI / age) for each gender (17).
Physical activity
Physical activity was assessed using a questionnaire developed and validated for adolescents by Florindo et al. (18). In order to classify the level of physical activity, the final score as a dichotomous variable was used, with the cutoff point being ≥ 300 min/week (active) and < 300 min/week (inactive).
Food consumption assessment vitamin D
Vitamin D intake was evaluated by applying a 24-hour recording with all participants and a new subsequent application to 40% of the sample in non-consecutive days, as described by Verly, Jr. et al. (19), following a minimum period of 30 days and a maximum of 45 days between the application of a recording and the next. Vitamin D intake was calculated using the Avanutri Revolution software version 3.0. After standardization of the household measurements and preparation of the datasheets, food or preparations that were not present in the software database were entered by means of food chemical composition tables (20,21) or processed food labels.
The residual nutrients method was used to control the power consumption interpersonal effects in the evaluation of micronutrients (22). The assessment of vitamin D consumption was made by comparing the values obtained to the recommendations of the dietary reference intakes (DRI´s) (23). Since no participant presented an intake above the recommended amount (10 µg/day), median adjusted one was used as Cutoff point to categorize the vitamin D consumption of adolescents. The set value was 1.48 µg/day.
Biochemistry evaluation
Blood samples were collected at the schools by a team of qualified professionals. All participants were instructed to remain fasting for 12 hours for blood collection and subsequent analysis of vitamin D, PTH, calcium and assessment of renal and hepatic function (urea, creatinine, uric acid, alanine transaminase and aspartate amino transferase). Serum concentrations of 25 (OH) D and PTH were measured by chemiluminescence immunoassay (UniCel DxI 800 - Beckman Coulter). The cutoff points used for classification of vitamin D were adopted from the Endocrine Society, which considers 25 (OH) D < 20 ng/mL deficient 21-29 ng/mL being insufficient and greater than 30 ng/mL being sufficient (24). Severe deficiency was considered as values < 10 ng/mL. They identified individuals with hypovitaminosis D as those with 25 (OH) D < 30 ng/mL. All blood samples for 25 (OH) D were obtained in the winter in Brazil. The PTH concentrations had values of normality established between 15-65 pg/mL. Serum calcium was carried out by automated colorimetric technique using Calcium Arzenazo commercial kits (Bechman Coulter) according to the manufacturer's guidelines. The median serum calcium level of the population (10.1 mg/dL) was defined as the reference cutoff point for evaluation. The markers used to evaluate renal and hepatic function were performed using commercial kits from Labtest (Minas Gerais, Brazil), following the manufacturer's recommendations.
Statistical analysis
Absolute and relative frequencies, mean and standard deviation of the variables were calculated. The prevalence of hypovitaminosis D was calculated for the general population and gender. Proportions were compared using the chi-square test considering a significance level of p < 0.05.
Intergroup differences were tested by the independent t-test or its non-parametric correspondent, the Mann-Whitney test. Poisson Regression with robust variance was used to determine the association between the independent variables with the outcome (hypovitaminosis D), which were used to estimate the crude and adjusted prevalence ratios with their respective confidence intervals (95% CI). The final dataset included variables with significance level of less than or equal to 0.20 in the unadjusted model. Data were analyzed by SPSS software version 21 and STATA, version 13.0 SE.
RESULTS
The mean age (SD) of the 220 adolescent participants was 16.8 ± 1.1, with the majority consisting of females. Regarding socioeconomic characteristics, almost half of the individuals were receiving social benefits and the mothers presented an education level < 9 years of study. Moreover, the results show that both the daily sun exposure and the practice of physical activity while exposed to the sun were more prevalent in adolescent males (p < 0.0001). Similarly, they showed a mostly higher prevalence in the consumption of vitamin D above the median (p = 0.004) (Table I).

Considering the overall sample, the classification of BMI/age, according to gender, indicated that 22.7% of adolescents were overweight/obese. Moreover, it was observed that women had a higher prevalence of being overweight / obese than men (p = 0.016), with the latter being mostly classified as physically active (p = 0.002) (Table I).
The prevalence of hypovitaminosis D in the study population was 57.7%, with 42.7% being insufficiency and 8.2% deficient in vitamin D. No study participants had severe deficiency (< 10 ng/mL). The insufficiency/deficiency of 25 (OH) D made up 74% of the female population and 30.6% of men. This difference was statistically significant and remained associated even after adjusting for all variables confirming that female adolescents had twice the chance hypovitaminosis D than adolescent males (p < 0.0001) (Data not shown). Regarding the individuals with only 25 (OH) D deficiency, 83.3% were composed of female adolescents.
The mean concentrations of 25 (OH) D in the general population were 29.6 ng/dL. No significant associations were found between vitamin D and PTH (p = 0.732) values. However, there was a direct and positive association between serum calcium and vitamin D in both genders (p < 0.000; r = 0,287). In addition, no cases of secondary hyperparathyroidism were found in the population. It was observed that females had average concentrations of vitamin D above 30 ng/dL for any variable analyzed. On the other hand, males had average concentrations of 25 (OH) D greater than recommended, except for the variable BMI/age (Table II).
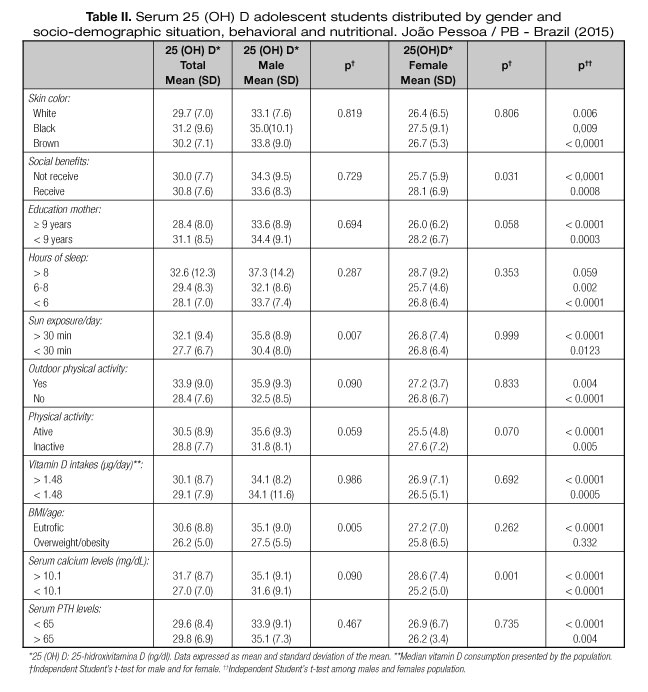
Table III shows the results of univariate analyses, showing that male BMI and serum calcium levels in females were associated with hypovitaminosis D. The results of the adjusted analyzes indicated that male adolescents who presented as being overweight/obese had 2.41 (1.28 to 4.55) times more chance to have hypovitaminosis D (p = 0.006). By contrast, hypovitaminosis D in female adolescents was more prevalent in the group with lower serum calcium concentrations (p = 0.046) (Table IV).


DISCUSSION
This study has found significant proportion of hypovitaminosis D among adolescents in school. In the analysis by gender, adolescent females showed much higher prevalence than males. In addition, hypovitaminosis D was independently associated with increased BMI in adolescent males, as well as there being low serum calcium concentrations present in females.
In the scientific literature, similar proportions of high hypovitaminosis D prevalence in adolescents have been found (25). In the countryside of São Paulo in Brazil, a study of 136 adolescents of both genders and ages between 16 and 20 years found hypovitaminosis D in 60% of participants (8). Likewise, Santos et al. (9) analyzed the serum concentrations of 25 (OH) D in 234 girls aged 7-18 years old in Curitiba-PR, observing that 90.6% of the population showed concentrations of this biomarker ≤ 30 ng/mL. In the town of Juiz de Fora-MG, 160 adolescents aged between 15 and 17 years were analyzed, and it was found that vitamin D insufficiency and deficiency was present in 70.6% of adolescents (7). All three studies were concentrated in south and southeastern Brazil.
The high prevalence of vitamin D deficiency in Brazil and around the world raise questions about the reference values used for classification. To date there is no international consensus that defines the optimal cutoff values for serum concentrations of 25 (OH) D, representing a major difficulty in establishing an overview of hypovitaminosis D in the world, especially in adolescents. After reviewing the literature the cutoffs established by the Endocrine Society (24) for adults was chosen as it is widely used in such studies, but it is possible that these values are below ideal, since adolescence is a phase that requires increased nutrient demands for proper skeletal development.
Thus, further research is needed to establish what would be the optimal levels of vitamin D to ensure optimal nutritional support during this period.
Another fact that draws attention to the high prevalence of vitamin D deficiency in adolescents studied is the fact that the study was conducted in a coastal region and has sunny days almost all year. Given this premise, the question arises about the isolated role that sunlight has on the serum concentrations of 25 (OH) D. Several studies show that even in tropical regions, the prevalence of hypovitaminosis D has been elevated (26,27).
A study conducted with 15 Brazilian male and female surfers found that after five hours with 75% of the area of the body exposed to the sun without sunscreen and at a time of greater direct impact of ultraviolet rays, they produced only 40% of the vitamin D required for daily consumption (27). In contrast, another study realized in Germany found that serum concentrations of individuals varied according to factors like the seasons, living in an urban or rural environment and the body mass index, in addition to time spent in sunny regions and the consumption of vitamin D. These findings suggest that the individual behavior of participants also influences the serum concentrations of vitamin D (28). Thus, this evidence leads us to conclude that factors other than sun exposure, traditionally established as the main way of obtaining vitamin D, can be listed as associated with this condition, such as gender and high BMI as demonstrated in our study.
Our results demonstrate that gender may be a determining factor that is strongly associated with vitamin D deficiency, since female adolescents had higher prevalence than males. Similar results have been found in other studies around the world (25,29). A recent cohort study conducted in the United States showed that in a model adjusted for several variables similar to ours, male participants had higher concentrations of 25 (OH) D over time when compared to females (30). Evidence has shown that this association can be explained by behavioral as well as physiological issues. However, this information has not been shown to be significant in our study nor is it well established in the literature, requiring further investigation.
Recent studies in animals and in humans have suggested that vitamin D plays an important role in hormonal modulation of the female reproductive system, due to the presence of vitamin D receptors (VDR) and enzymes associated with metabolism in the female reproductive tissues (31). Particularly in female population, vitamin D deficiency may be related to the development of future highly prevalent diseases in this population, such as breast cancer, polycystic ovary syndrome, endometriosis and even infertility according to research (32).
The high BMI was independently associated with insufficiency/deficiency of vitamin D in our results. In a study conducted with obese children, insufficient vitamin D concentrations < 20 ng/mL) were found in 5% of eutrophic children in the control group and in 30% of those who were obese (33). In another recent study, it was observed that the risk of developing vitamin D deficiency was strongly associated with increased adiposity in children and adolescents aged 6-18 years old (34). BMI also seems to exert influence on individuals' response to different doses and types of vitamin D supplementation, as demonstrated by the recent Hammami and Yusuf study (35). However, it is believed that the combination of low concentrations of 25 (OH) D in overweight/obese individuals goes beyond sun exposure and food intake.
Some evidences suggest that one of the causes of 25 (OH) D deficiency in individuals with obesity may be related to storage of this vitamin in the adipocytes, reducing its bioavailability. In addition, it has been reported that adipose tissue has a lower expression of the enzymes responsible for the hydroxylation of vitamin D, as well as from 1-α-hydroxylase, suggesting a compromise in its activities in obesity (36). Alternatively, some experimental data suggest that vitamin D deficiency can cause greater adiposity, promoting elevation of PTH, which promotes calcium entry into adipocytes and thus, increases lipogenesis (37). This cyclical association requires further research to clarify and direct the relationship between vitamin D and obesity.
The median intake of vitamin D was much lower than that of DRI's recommendations, for both genders in this study. Low intake has been reported in other regions of Brazil and other countries (7,38). Vitamin D food sources are limited and are not usually consumed in Brazil by adolescents, such as the liver oil of fish and salmon. Furthermore, there is no mandatory food enrichment in Brazil and only recently some products like milk and yogurt have begun to be enriched with vitamin D. Another factor that may explain the low intake of vitamin D is the high prevalence of unhealthy eating habits at this stage of life, such as the high consumption of processed foods, replacing main meals with snacks or simply not eating at correct times (39); data also observed in our population.
Lower calcium serum concentrations were related to a higher prevalence of hypovitaminosis D in females. Particularly in adolescence there is a growing concern about vitamin D, since this period requires an increased mobilization of nutrients for the formation and growth of body tissues. Moreover, a major function of vitamin D is to promote calcium absorption. It is known that low concentrations of the active form of 1.25 (OH) 2D result in decreased absorption from the intestinal calcium and decreased bone reabsorption (40), and that this association can cause future implications to the health of these young people. Furthermore, it has been found recently that vitamin D may influence the formation of female hormones such as estradiol, for which a deficiency can lead to outcomes associated to bone metabolism (32).
Some limitations of this study should be considered. The difficulty of food composition tables used for dietary assessment may have contributed to low vitamin D intake among the adolescents. In addition, the criteria used to evaluate the sun exposure of adolescents may have been a little too specific to that function, requiring validated studies comparing different measures of sun exposure according to age groups, since the habit of sun exposure may vary with age. Extrapolation of the results to the general population of Brazilian adolescents should be cautious, since the region where the study was carried out has particular characteristics of sun exposure and dietary intake. Finally, being a cross-feature study, it is not possible to infer causality between the outcome (vitamin D deficiency) and the factors that were associated.
Some of the study capabilities also need to be listed. This is a pioneer study conducted in a city in northeastern Brazil, and in this way the results contribute to chart a situational overview of vitamin D deficiency in Brazilian adolescents. The identification of potentially associated factors may contribute to the prevention of various diseases in adulthood that have their pathophysiology related to hypovitaminosis D. In addition, the data from this study awakens the need to encourage debate about the main important measures to combat this phenomenon.
CONCLUSION
The data of this study estimate a high prevalence of hypovitaminosis D in a population of adolescent students in northeastern Brazil, especially female. The following factors were independently associated: nutritional status (overweight/obesity) in males and lower serum calcium concentrations in females. For future research, it is suggested that retrospective and prospective longitudinal studies be done that are able to assess the change in serum levels of 25 (OH), as well as to more deeply examine the background of this population.
Lastly, besides the commonly known measures that help minimize this condition such as regular sun exposure, other strategies such as mandatory enrichment of vitamin D in food sources and possible supplementation of individuals in adolescence need to be considered by public health organizations in Brazil and throughout the world, especially for females or those with associated risk factors.
REFERENCES
1. Bikle DD. Vitamin D and bone. Curr Osteoporos Rep 2012;10:151-9.
2. Leu M, Giovannucci E. Vitamin D: Epidemiology of cardiovascular risks and events. Best Pract Res Clin Endocrinol Metab 2011;25:633-46.
3. Muscoqiuri G, Sorice GP, Aijan R, Mezza T, Pilz S, Prioletta A, et al. Can vitamin D deficiency cause diabetes and cardiovascular diseases? Present evidence and future perspectives. Nutr Metab Cardiovasc Dis 2012;22:81-7.
4. Neves JPR, Silva AS, Morais LCSL, Diniz AS, Costa MJC, Asciutti LSR, et al. 25-hydroxyvitamin D concentrations and blood pressure levels in hypertensive elderly patients. Arq Bras Endocrinol Metab 2012;56:415-22.
5. Cheng TY, Millen AE, Wactawski-Wende J, Beresford SA, Lacroix AZ, Zheng Y, et al. Vitamin D Intake Determines Vitamin D Status of Postmenopausal Women, Particularly Those with Limited Sun Exposure. J Nutr 2014;144:681-9.
6. Van Horn LV, Bausermann R, Affenito S, Thompson D, Striegel-Moore R, Franko D, et al. Ethnic differences in food sources of vitamin D in adolescent American girls: the National Heart, Lung, and Blood Institute Growth and Health Study. Nutr Res 2011;31:579-85.
7. Oliveira RM, Novaes JF, Azeredo LM, Cândido AP, Leite IC. Association of vitamin D insufficiency with adiposity and metabolic disorders in Brazilian adolescents. Public Health Nutr (2013);17:787-94.
8. Peters BS, Dos Santos LC, Fisberg M, Wood RJ, Martini LA. Prevalence of Vitamin D Insufficiency in Brazilian Adolescents. Ann Nutr Metab 2009;54:15-21.
9. Santos BR, Mascarenhas LP, Satler, Boguszewski MCS, Spritzer PM. Vitamin D deficiency in girls from South Brazil: a cross-sectional study on prevalence and association with vitamin D receptor gene variants. BMC Pediatr 2012;12:1-7.
10. Castro LC. The vitamin D endocrine system. Arq. Bras Endocrinol Metab 2011;55:566-75.
11. Bandeira F, Griz L, Freese E, Lima DC, Thé AC, Diniz ET, et al. Vitamin D deficiency and its relationship with bone mineral density among postmenopausal women living in the tropics. Arq Bras Endocrinol 2010;54:227-32.
12. Roomi MA, Farooq A, Ullah E, Lone KP. Hypovitaminosis D and its association with lifestyle factors. Pak J Med Sci 2015;31:1236-40.
13. Jollife DA, Walton RT, Griffiths CJ, Martineau AR. Single nucleotide polymorphisms in the vitamin D pathway associating with circulating concentrations of vitamin D metabolites and non-skeletal health outcomes: Review of genetic association studies. J Steroid Biochem Mol Biol 2016;15:30153-9.
14. Instituto Brasileiro de Geografia e Estatística. Pesquisa de orçamentos familiares 2008-2009: despesas, rendimentos e condições de vida; 2010.
15. Hanwell HEC, Vietha R, Cole DEC, Scillitani A, Modoni S, Frusciane V, et al. Sun exposure questionnaire predicts circulating 25-hydroxyvitamin D concentrations in caucasian hospital workers in southern Italy. Steroid Biochem Mol Biol 2010;121:334-7.
16. Lohman TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Champaign, Illinois: Human Kinetics Books; 1991.
17. World Health Organization. Nutrition in Adolescence: Issues and Challenges for the Health Sector. Issues in Adolescent Health and Development. Geneva: WHO; 2005.
18. Florindo AA, Romero A, Peres SV, Silva MV, Slater B. Desenvolvimento e validação de um questionário de avaliação da atividade física para adolescentes. Rev Saúde Pública 2006;40:802-9.
19. Verly-JR E, Castro MA, Fisberg RM, Marchioni DM. Precision of usual food Intake Estimates According to the Percentage of Individuals with a second dietary Mensurement. J Acad Nutr Diet 2012;112:1015-20.
20. Philippi ST. Tabela de Composição de Alimentos: Suporte para Decisão Nutricional. São Paulo: Manole; 2015.
21. Pinheiro ABV, Lacerda EMA, Benzecry EH, Gomes MCS, Costa VM. Tabela de Composição de Alimentos. São Paulo: Ed. Atheneu; 2004.
22. Willet W, Stampfer M. Implications of total energy intake for epidemiological analyses. In Nutritional Epidemiology. 2nd ed. New York: Oxford University Press; 1998.
23. Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D. Fluoride. Washington, DC: National Academy Press; 2010.
24. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96:1911-30.
25. Durá-Travé T, Gallinas-Victoriano F, Chueca GMJ, Berrade-Zubiri S. Vitamin D deficiency among children and adolescents with normal nutritional status. Nutr Hosp 2015;32:1061-6.
26. Cabral MA, Borges CN, Maia JM, Aies CA, Bandeira F. Prevalence of vitamin D deficiency during the summer and its relationship with sun exposure and skin phototype in elderly men living in the tropics. Clin Interv Aging 2013;8:1347-51.
27. Carvalho EKB, Griz L, Fontenele T, Accioly LV, Melo AA, Amaral LMB, et al. Serum 25OHD changes following high rates of sun exposure in young subjects with pigmented skin living in the tropics. Clinical and experimental medical sciences 2013;1:363-71.
28. Richeter K, Breitner S, Webb AR, Huth C, Thorand B, Linseisen J, et al. Influence of external, intrinsic and individual behaviour variables on serum 25(OH)D in a German Survey. J Photochem Photobiol 2014;140:120-9.
29. Narchi H, Kochiyil J, Al Hamad S, Yasin J, Laleye L, Al Dhaheri A. Hypovitaminosis D in adolescent females - an analytical cohort study in the United Arab Emrates. Paediatr Int Child Health 2015;35:36-43.
30. McKibben RA, Zhao D, Lutsey PL, Schneider LC, Gallar E, Mosley TH, et al. Factors Associated With Change in 25-Hydroxyvitamin D Levels Over Longitudinal Follow-Up in the ARIC Study. J Clin Endocrinol Metab 2016;101:33-43.
31. Al-Jaroudi D, Al-Banyan RN, Aljohani NJ, Kaddour O, Al-Tannir M. Vitamin D deficiency among subfertile women: case control study. Gynecological Endocrinology 2015;11:1-4.
32. Anagnostis P, Karras S, Goulis DG. Vitamin D in human reproduction: a narrative review. Int J ClinPract 2013;67:225-35.
33. Codoñer-Franch P, Tavárez-Alonso S, Simó-Jordá R, Laporta-Martín P, Carratalá-Calvo A, Alonso-Iglesias E. Vitamin D status is linked to biomarkers of oxidative stress, inflammation, and endothelial activation in obese children. J Pediatr 2012;16:848-54.
34. Moore CE, Liu Y. Low serum 25-hydroxyvitamin D concentrations are associated with total adiposity of children in the United States: National Health and Examination Survey 2005 to 2006. Nutr Res 2016;36:72-9.
35. Hammami MM, Yusuf A. Differential effects of vitamin D2 and D3 supplements on 25-hydroxyvitamin D level are dose, sex, and time dependent: a randomized controlled trial. BMC Endocr Disord 2017;17:1-14.
36. Valint S. Vitamin D and obesity. Nutrients 2013;5:949-56.
37. Yao Y, Zhu L, He L, Duan Y, Liang W, Nie Z, et al. A meta-analysis of the relationship between vitamin D deficiency and obesity. Int J Clin Exp Med 2015;8:14977-84.
38. Au LE, Economos CD, Goodman E, Must A, Chomitz VR, Sacheck JM. Vitamin D intake and serum vitamin D in ethnically diverse urban schoolchildren. Public Health Nutr 2012;15:2047-53.
39. Martini LA, Verly-Jr E, Marchioni DM, Fisberg RM. Prevalence and correlates of calcium and vitamin D status adequacy in adolescents, adults, and elderly from the Health Survey-São Paulo. Nutrition 2013;29 845-50.
40. Maeda SS, Borba VZC, Camargo MBR, Silva DMW, Borges JLC, Bandeira F, et al. Recommendations of the Brazilian Society of Endocrinology and Metabology (SBEM) for the diagnosis and treatment of hypovitaminosis D. Arq Bras Endocrinol Metab 2014;58:411-33.
 Correspondence:
Correspondence:
Eduarda Pontes dos Santos Araújo.
Rua Bancário Antonio Macau, 61
59051-823 João Pessoa, Brazil
e-mail: eduarda.pontes00@gmail.com
Received: 08/03/2017
Accepted: 07/06/2017

