










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Childhood overweight and obesity are a worldwide health issue and the incidence of the condition is increasing at alarming rate 1,2. Despite a growing evidence on the knowledge of the multifactorial nature of this condition, many questions regarding the specific consequences of the disease are still unanswered 2. For example, few have examined the structural and functional limitations of excess weight 3,4,5. These studies have predominantly been in adult samples and few data have been reported for pediatric populations. This is quite surprising since excess weight may limit functional performance by making daily life activities more difficult 2. In this context, previous studies have identified that fundamental movement skills (running, hopping, jumping, catching and throwing) skills are negatively influenced by overweight or obesity 6,7. More specifically, previous works 3,4 have examined the association between body mass index (BMI), physical activity and functional movement by employing the Functional Movement Screen(tm) (FMS) in children. The authors reported that poorer functional movement was associated with higher BMI and lower levels of physical activity in British children compared to normal weight children 3,4.
The movement patterns examined in the FMS place the athlete in positions where functional movement limitations and asymmetries may be identified 8. The FMS consists of seven tests, each scored between zero and three points with three representing the best possible score. The composite score, or total screen score, ranges from 0 to 21 points. The seven tests include the deep squat, hurdle step, inline lunge, shoulder mobility, active straight-leg raise, trunk stability push-up, and rotary stability tests. Descriptions of the tests and scoring criteria have been previously reported 8,9,10,11.
At school-age, sport practice should aim at enjoyment, health and personal development 12,13,14. However, as indicated by Maffulli 13, young athletes train harder and longer with the purpose of being competitive and winning, and as an undesired but inevitable consequence, sports-related injuries have increased significantly. The volume of injuries reported in this setting, along with the fact that many of the more significant sports-related injuries may lead to long-term physical impairment, warrants research into the possibility of utilizing pre-participation screening methods that are able to identify young athletes that are at a high risk of becoming injured 12. The functional movement patterns in youth have been associated to both athletic performance 15,16 and risk of injury 8,17 with controversial results.
A previous study 3 aimed to examine relations between functional movement patterns and weight status in British primary school children. Nevertheless, to the best of the authors' knowledge, no data have been published according to Spanish peers. The aim of this study was twofold: a) to examine relations between functional movement patterns and weight status in Spanish primary school children; and b) to determine the differences between sexes on the aforementioned relations.
MATERIALS AND METHODS
PARTICIPANTS
A group of 333 children, 164 girls and 169 boys (age range = 6-13 years; age = 9.68 ± 1.49 years; BMI = 18.54 ± 3.87 kg/m2) participated in this study. They were selected from different schools in southern Spain (Andalusia). The sample was selected by convenience in both urban and rural areas. Inclusion criteria included being free from physical and/or intellectual disabilities. Exclusion criteria included: a) the use of a mobility aid or prophylactic device (e.g., knee brace); b) a musculoskeletal impairment or injury or head injury (< 6 weeks) which was likely to affect their motor performance; and c) children diagnosed with any form of developmental disorder likely to influence motor performance were also excluded (i.e., developmental coordination disorder, dyspraxia, dyslexia, Asperger's syndrome and autism). Parents voluntarily signed an informed consent form for the participation of their children in this study. The study was completed in accordance with the norms of the Declaration of Helsinki (2013 version) 18) and following the directives of the European Union on Good Clinical Practice (111/3976/88 of July, 1990), as specified in the Spanish legal framework for human clinical research (Royal Decree 561/1993 on clinical essays). The study was approved by the Ethics Committee of the University of Jaen (Jaen, Spain).
PROCEDURES
Anthropometry
Body height (cm) was measured with a stadiometer (Seca® 222, Hamburg, Germany, precision = 1 mm) and body mass, with a weighing scale (Seca® 899, Hamburg, Germany, precision = 100 g). Waist circumference (WC) was measured using a Seca® Ergonomic Circumference Measuring Tape SE201 (Seca, Germany, precision = 1 mm). Children were assessed in bare feet and lightly clothed (in their Physical Education kit) and measurements were taken by accredited anthropometrists (levels II and III) by using the standard International Association for the Advancement of Kinanthropometry (ISAK) protocol for such measurements. Consequently, body mass index was determined as kg/m2. Children were classified as normal weight (NW, 67.2%, n = 221), overweight (OV, 22.2%, n = 73) or obese (OB, 10.6%, n = 35) according to IOTF criteria 19.
Functional movement assessment
The Functional Movement Screen(tm) (FMS(tm)) is a pre-participation screening tool which evaluates the Fundamental Movement Patterns that underpin performance of all movement 9,10. The FMS consists of seven tests: deep squat, in-line lunge, hurdle step, shoulder mobility, stability push-up, rotational stability and active straight leg raise which challenge an individual's ability to perform basic movement patterns that reflect combinations of muscle strength, flexibility, range of motion, coordination, balance and proprioception 9,10. The FMS was administered by a trained rater using standardized procedures, instructions and scoring processes 9,10. Each participant was given three trials on each of the seven tests in accordance with recommended guidelines 9,10. Each trial was scored from 0 to 3 with higher scores reflecting better functional movement. In regard to the criteria for scoring on the FMS, a score of 3 is awarded for perfect execution of the movement; 2, for execution that demonstrates compensation and less than perfect form; 1, where there is inability to complete the movement pattern because of stiffness, loss of balance or another difficulty; and a score of 0 is awarded if there is pain when performing the movement. Comprehensive instructions for each movement are also provided elsewhere 9,10.
For each test, the highest score from the three trials was recorded and used for analysis. These scores were also summed to generate an overall composite FMS score with a maximum value of 21 and in accordance with recommended protocols 5,10. In the present study both the composite FMS score and individual scores for each component of the FMS were used. This is consistent with previous research with children 3. The composite FMS score provides a holistic evaluation of an individual's functional movement 9,10. However, individual scores for each of the FMS tests are needed to determine an individual's consistency of movement, to determine whether there is a specific movement dysfunction 9,10.
Although independent research examining the validity and reliability of the individual tests within the FMS is not available in children, some studies have previously used it in that population 3,5,15,16. Additionally, a previous work 5 with young people (18-40 y) determined an excellent inter-rater reliability (ICC) for the composite FMS score, and for individual test components of the FMS (Kappa). Likewise, in a study with school-age children 3 kappa values revealed excellent test re-test agreement for total composite score and individual FMS tests (kappa = 0.97 to 1).
Statistical analysis
Data were analyzed using SPSS v.21.0 for Windows (SPSS Inc, Chicago, USA) and the significance level was set at p < 0.05. Tests of normal distribution (Kolmogorov-Smirnov) were conducted on all data before analysis. Since data did not meet the requirements for parametric statistical analysis, non-parametric tests were used for analysis. A Spearman correlation analysis was conducted to determine the relationship between total FMS score and BMI. The between-group comparison according to the distribution of participants (for sex and weight status groups) was conducted through the Chi2 test (Χ2) with a post-hoc analysis (Bonferroni test). Differences in scores for each test and the total composite score between sex groups were assessed using the Mann-Whitney U test and any differences in scores for each test and the total composite score between NW, OV and OB children were examined using the Kruskal-Wallis test. Where any significant differences were found, post-hoc analysis employing the Mann-Whitney U test with Bonferroni correction was used to determine where these differences lay.
RESULTS
The Spearman correlation analysis reported a moderate and negative correlation between total FMS score and BMI (rho = -0.479, p < 0.001). It also reported a no significant relation between age and total FMS score (rho = 0.130; p = 0.104).
Table 1 shows the distribution of boys and girls between weight status groups. The Chi2 test showed no significant differences (p = 0.589, Χ2 = 1.058) between sexes according to the presence of sexes in BMI groups (NW, OV and OB groups).
Table I. Distribution of participants into weight status groups according to sex (n, %)
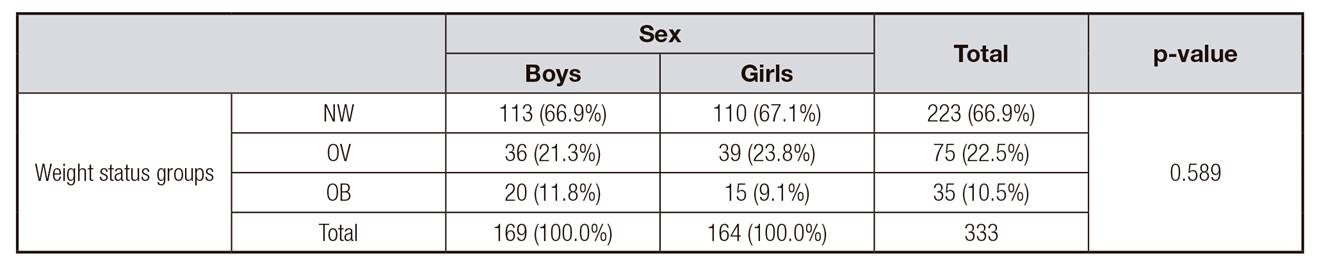
NW: normal weight group; OV:overweight group; OB:obese group.
Total FMS scores according to sex and weight status groups are presented in Table 2. Total FMS score was significantly different between children from NW, OV and OB groups (p = 0.001) either considering the whole group or the sex groups. Post-hoc testing showed that total FMS score was significantly lower (p < 0.05) with the increased BMI, with significant differences between all groups (NW-OV, NW-OB and OV-OB for the total sample and boys) and according to NW in girls. According to the between-sex comparison, significant differences (p = 0.046) were found in the NW group, with girls showing a greater score (+1.06 points) than boys. No significant between-sex differences were found for the whole group (p = 0.601) in the OV (p = 0.693) nor OB groups (p = 0.723).
Table II. Total FMS scores (mean, SD) for sex and weight status groups

NW: normal weight group; OV: overweight group; OB: obese group. The same letter indicates significant differences (p < 0.05) between BMI-based groups (within group comparison according to sex).
*Indicates differences between sexes (p < 0.05) (within group comparison according to weight status groups).
Percentages of score distributions for each individual FMS test between the weight status groups are shown in Figure 1. Significant differences between NW, OV and OB were found in deep squat (p = 0.002), hurdle step (p = 0.002), in-line lunge (p = 0.027), shoulder mobility (p = 0.005), straight leg-raise (p = 0.013) and push-up (p = 0.002) tests, while no significant differences were found in rotary stability (p = 0.119). NW children outperformed the OV group on the hurdle step (p = 0.040) and push-up (p = 0.032) tests, and both NW and OV groups outperformed their OB peers in six out of seven tests performed (all p < 0.05 or better). Of particular note, any participant scored 0 in the hurdle step test.
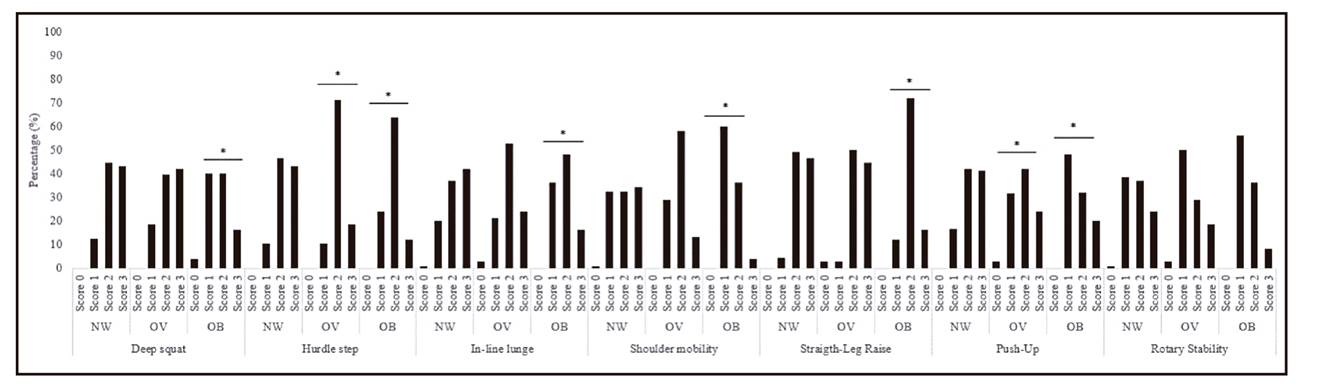
Figure 1. Percentages of score distributions for each individual FMS test between the weight status groups. NW: normal weight; OV: overweight; OB: obese. *Indicates significant differences (p < 0.05) according to normal weight group.
Figure 2 shows the percentage of score distributions for each individual FMS test between boys and girls. Girls obtained higher scores in the following tests: in-line lunge (p = 0.021), shoulder mobility (p = 0.008) and straight leg-raise (p = 0.024), whereas boys did it in the push-up (p = 0.044) test. No significant between-sex differences were found in the rest of tests (p ≥ 0.05).

DISCUSSION
This study aimed to examine the relationship between FMS scores and weight status in Spanish primary school children and to determine the differences between sexes. In this respect, the main findings of the current study were: a) BMI correlates moderately and inversely with FMS score in Spanish primary school children; b) OV and OB groups showed poorer functional movement compared to NW children; and c) girls outperform boys in movements requiring flexibility (hamstrings and shoulders) and balance, whilst boys outperform girls in tests where muscular strength is required (push-up).
The results of the present study are confirmatory of prior work 3. That work determined the association between weight status and FMS in a sample of 90, 7-10 years old British school children by concluding that overweight and obesity are significantly associated with poorer functional movement in children, and that girls outperform boys in functional movements. The relationship between functional movement (motor competence), physical activity and weight status is not a new assertion and the results reported here align with the conceptual model previously presented by Stodden et al. 20. In fact, some previous works 2,3,4,5 have considered this suggestion, but with British children 3,4, without examining the effect of weight status 5, or in adults 2. In this context, the current study confirms that FMS score was lower with the increased BMI in Spanish school-age children, regardless of sex, which might indicate the presence of maladaptive movement patterns in overweight and obese children. Additionally, these results highlight that OV and OB conditions cannot simply be equated in terms of FMS outcomes. This finding is consistent with a previous work 3 conducted with British people, so that the data reported here should be considered as extending current knowledge on other populations.
As for the second aim of this work, analyzing the differences between sexes, the results reported here partially agree with those reported by similar studies. In a population of young adults, Schneiders et al. 5 reported sex differences in the straight leg raise and trunk stability push-up. Focused on the use of the FMS in a pediatric population, Duncan et al. 3, in a sample of 7-10 years old British school children, concluded that girls outperform boys in functional movements requiring hamstring flexibility and balance whilst boys outperform girls in tests where muscular strength is required. This finding is totally consistent with our results, with girls obtaining higher scores in in-line lunge, shoulder mobility and straight leg-raise, whilst boys did it in push-up tests. Additionally, our study revealed no overall sex difference (in terms of total FMS score), however, between-sex differences were found in the NW group, with girls showing a greater score (+1.06 points) than boys (and no differences in OV and OB groups). In this respect, the study by Duncan et al. 3 reported no overall sex difference but did not inform about weight status groups comparisons. Likewise, the data presented by Duncan and Stanley 4 are in the same line, with no sex differences in total FMS scores of 10-11 years old children. As suggested by Duncan et al. 3, one potential explanation for the sex differences in particular functional movements reported in the present study has been children's physical activity socialization 21. Opportunities to practice functional movements related to strength performance tend to be higher in boys, whereas girls tend to participate more regularly in sports such as dance or gymnastics 22.
Finally, some limitations need to be considered. First, the influence of a potential confounding variable as age. The present sample did not have a sufficient balance of age groups across multiple weight status groups and that is why the authors decided not to incorporate it. Nevertheless, it is important to note that the correlation analysis showed no significant relation between age and FMS score. Further analysis needs to be addressed to get clearer conclusions. Second, other potential confounding variables such as level of physical activity, socio-economic status and ethnic group should be considered. Notwithstanding these limitations, the current study confirms the inverse relationship between functional movement and weight status, and it extends the finding from British population into Spanish primary school children by analyzing a large sample (333, 6-13 years old children).
CONCLUSIONS
To sum up, the results of this study build on prior studies on this topic by extending the findings from British primary school children into Spanish population (6-13 years old). The results of the present study confirm that total FMS score significantly and inversely correlates with BMI in a group of 333 school-age children. Presenting individual FMS scores alongside the total score, the data revealed that NW children outperformed the OV group on the hurdle step and push-up tests, and both NW and OV groups outperformed their OB peers in six out of seven tests performed. As for the differences between sexes, girls outperform boys in movements requiring flexibility (hamstrings and shoulders) and balance, whilst boys outperform girls in tests where muscular strength is required (push-up).
From a practical point of view, the data presented here support the need for interventions to improve functional movement in Spanish children generally but in those who are overweight and obese specifically.

