










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Adolescence is a nutritionally vulnerable period for many reasons, especially by increased needs due to growth and development, and changes in dietary patterns and behaviors related to lifestyle 1. Poor eating habits are considered as a major public health problem because of their relation to the manifestation of chronic diseases. Among children and adolescents, this problem is more serious because many erroneous food preferences are established during this period 2.
The eating habits of Brazilian adolescents have been characterized as inadequate due to a high consumption of processed foods, rich in saturated fats, added sugar and sodium, combined with a low consumption of fruits, vegetables, beans and dairy products 3. Consequently, there are increasing evidences linking micronutrient deficiencies to chronic diseases such as cardiovascular disease, cancer, diabetes and osteoporosis in adulthood 4,5.
The deficiency in fat-soluble vitamins may be a health problem not recognized in children and adolescents because these population groups are not routinely investigated 6, making the data on the status of these vitamins in adolescents scarce, especially in northeastern Brazil. Thus, this study aims to estimate the prevalence and the factors associated with the deficiency of vitamins A, D and E among adolescent students from northeastern Brazil.
METHODOLOGY
STUDY DESIGN AND SAMPLES
Cross-sectional study involving adolescents aged 12 to 19 of both genders, from March to April 2013, in a prospective cohort study conducted in 2007-2013 with teenagers recruited randomly by a multi-stage sampling process in public schools of Recife, northeastern Brazil. Adolescents who used pharmacological vitamin A, D, E or multivitamins in the last three months were excluded.
The sample size was based on an estimated prevalence (p) of α-tocopherol deficiency of 25%, a sampling error (d) of 5.5%, a confidence level of 95% (z) and an effect of design © of 2.1, considering that the sample selection was made by conglomerates. Using the formula n = (z2 x p x q x c)/d2, corrected for a finite population, it resulted in a minimum sample of 370 individuals. To correct possible losses, a percentage of 11% (100/[100-11]) was increased, resulting in a sample with 444 adolescents. The final working sample was 411 adolescent students.
METHODS AND EVALUATION TECHNIQUES
Data collection was conducted by applying a questionnaire addressing socioeconomic variables, lifestyle and the food intake of adolescents. The interviews aiming to obtain dietary data were performed by two experts and a Nutrition graduate student at the Federal University of Pernambuco. To ensure the accuracy and reliability of the data, all members of the research team received training and orientation on the procedures and the routine development of the study. Then, an anthropometric evaluation and a blood sampling were performed to analyze serum concentrations of retinol, β -carotene, α-tocopherol and 25-hydroxy vitamin D (25[OH]D).
SOCIOECONOMIC STATUS
The variables were obtained through interviews conducted at school and/or domicile, including questions about gender, age and socioeconomic classification. To determine the socioeconomic status (SES), the Brazilian Economic Classification Criteria, established by the Brazilian Association of Market Research Agencies (ABEP) 7, was employed. This instrument uses a point scale, obtained by adding the possession of household items and the degree of the head of household educational level, which classifies the population in the following economic classes: A1, A2, B1, B2, C1, C2, D, and E, in descending order, respectively initiated by the highest purchasing income. Thus, SES was classified according to the following scheme: high SES (classes A1, A2), middle SES (classes B1, B2), low SES (classes C1, C2) and lowest SES (classes D, E).
VARIABLES RELATED TO LIFESTYLE
The adolescents were classified according to physical activity level into little active/sedentary or sufficiently active, according to the criteria proposed by Pate et al. 8. Adolescents were classified as smokers by reporting smoking an amount equal to or higher than five cigarettes/day 9. Adolescents who declared drinking an amount of alcohol > 30 g/day for males and > 15 g/day for females were considered as positive to alcohol intake habit 10.
DIETARY VARIABLES
Dietary intake was assessed by a semi-quantitative food frequency questionnaire for adolescents (FFQA), developed and validated by Slater et al. 11 and adapted for the usual food consumed in the area. The dietary intake was analyzed with the software DietSys, version 4.01 (National Cancer Institute, Bethesda, MD, USA), which uses as database the Chemical Composition Table of the United States Department of Agriculture (USDA). The results from the intake of vitamins A, D and E were compared with the values of dietary reference intakes (DRI) proposed by the Institute of Medicine 12.
ANTHROPOMETRIC VARIABLES
The anthropometric evaluation consisted in a double measurement of weight and height. The average resulting from the two measurements was used as the final result. For data consistency, the measurements that had differences of more than 100 g for weight and 0.5 cm for height were not considered. Weight and height measurements were performed according to the original technique recommended by Lohman et al. 13. The nutritional diagnosis of adolescents was defined based on body mass index (BMI) curves for age and gender according to the WHO reference data 14.
BIOCHEMICAL VARIABLES
Biochemical analyses were performed after collecting approximately 10 ml of blood by venipuncture at school or domicile after a 10-12-hour fasting. The flasks were packed in Styrofoam boxes containing recyclable ice, sealed and transported for sample processing at the LAPAC laboratory of clinical analysis within a maximum of two hours. The serum was separated from erythrocytes by centrifugation and stored in two 2 ml tubes. Immediately, one of the serum aliquots was used to analyze the concentration of 25(OH)D. Another serum aliquot (2 ml) was frozen and later sent to the Centre for Micronutrients Research (CIMICRON) of the Federal University of Paraiba (UFPB) to determine serum retinol, β-carotene and α-tocopherol concentrations.
RETINOL, β-CAROTENE AND α-TOCOPHEROL
The quantification of serum retinol, β -carotene and α -tocopherol levels followed the technical procedure described by Erhardt et al. 15. The cut-off points recommended by the WHO for retinol levels were used, adopting the classification: poor: < 0.35 µmol/l; low: 0.35-0.69 µmol/l; acceptable: 0.70-1.04 µmol/l; and normal: ≥ 1.05 µmol/l. Vitamin A deficiency was present when retinol levels were below 0.70 µmol/l. For α -tocopherol, the values ≥ 12 µmol/l were used as reference, while the values of β-carotene were considered appropriate in concentrations > 0.9 µmol/l.
25-HYDROXYVITAMIN D
25(OH)D levels were measured by high-performance liquid chromatography (HPLC). There is a vitamin D deficiency when the value of 25(OH)D is less than 52.5 nmol/l and insufficient when values are between 52.5 and 72.4 nmol/l.
DATA ANALYSIS
Data were double entered and verified with VALIDATE, a module of the Epi-Info(tm) software version 6.0 (WHO/CDC, Atlanta, GE), to verify the consistency of the typing process. The statistical analysis was performed using the Statistical Package for Social Sciences - SPSS, version 13.0 (SPSS Inc., Chicago, IL).
Continuous variables were tested for distribution normality by the Kolmogorov-Smirnov test (to evaluate the symmetry of the distribution curve of variables). Data from normally distributed variables were expressed as means and standard deviation. The variables with a non-Gaussian distribution were presented as medians and the respective interquartile intervals. In the description of proportions, the binomial distribution was approximated to the normal distribution with a 95% confidence interval.
In the univariate analysis, the strength of association was assessed by prevalence ratios, the respective confidence intervals and the Pearson's Chi-square test. For the comparison among continuous data from independent samples, the t-test or its nonparametric equivalent, Mann-Whitney U test, were used. In all statistical analyses, a 5% significance level was used to reject the null hypothesis.
ETHICAL ASPECTS
The study was approved by the Ethics Committee in Research with Human Beings of the Hospital Universitário Lauro Wanderley at the Federal University of Paraiba, Brazil (registration CEP/HULW no. 723/10), guided by ethical standards for research involving human beings as determined by the resolution no. 196/96 of the National Health Council.
Adolescents and their parents were previously informed of the research objectives and the adopted methods. With their consent, the person responsible signed an informed consent form. The return of the results of evaluations was guaranteed to adolescents and their parents, in addition to the confidentiality of data. The researchers were available for any questions regarding procedures, risks, benefits and other questions related to the study.
RESULTS
The study included 411 adolescents. However, there were some losses in the following variables: socioeconomic status (53) and smoking 1, due to lack of answers; BMI/age 3, due to inconsistencies between the two measurements; vitamin A 11 and E 11 intake, due to information inconsistencies; and serum retinol 14, β -carotene (87) and α-tocopherol 11 due to biological material insufficiency.
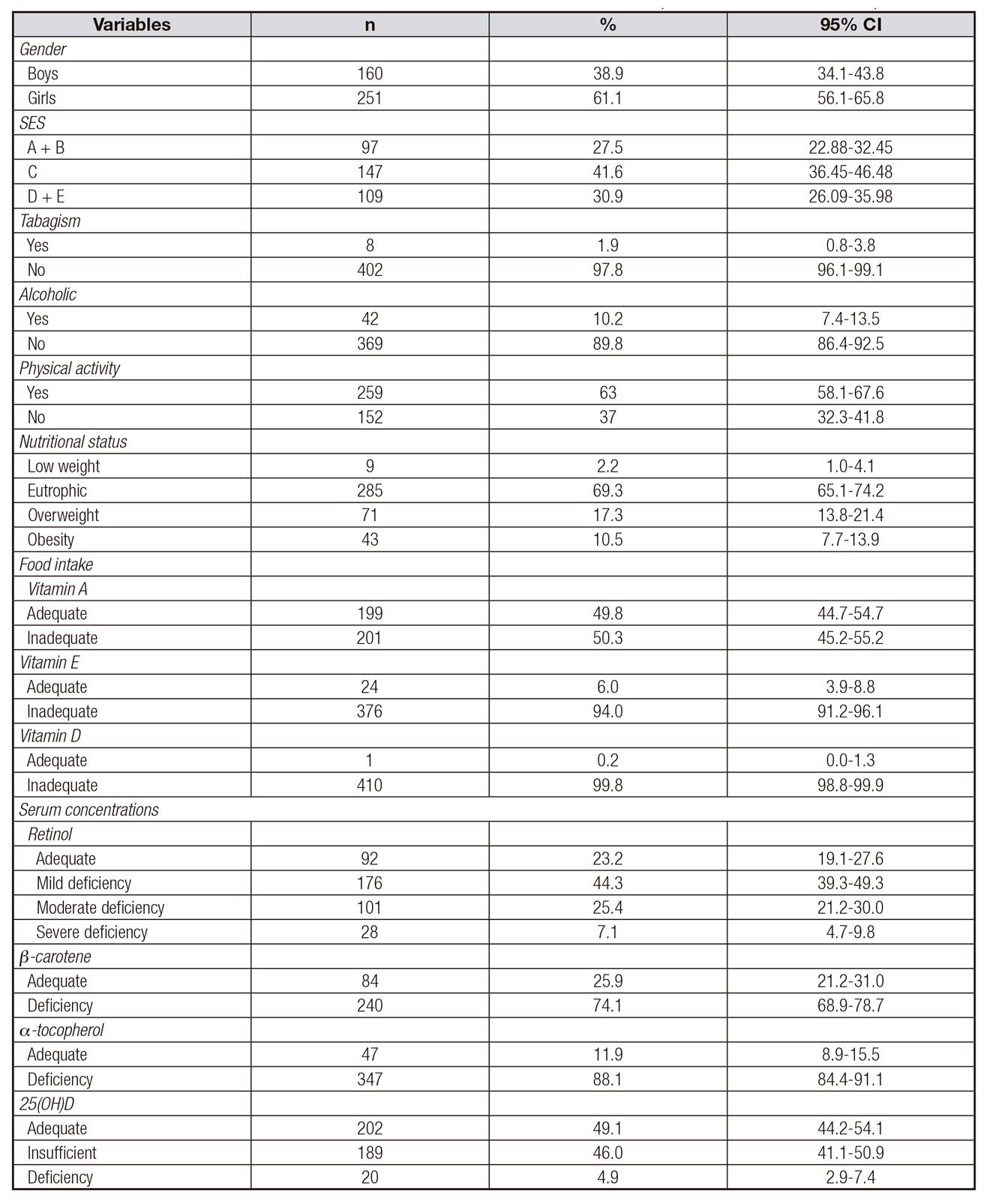
Most adolescents studied were females (61.1%; 95% CI 56.1-65.8). They had a median age of 15 years (IQ: 14-16 years), with a minimal variation of 12 and a maximum of 19 years. According to the socioeconomic status, it was observed that a higher percentage (41.6%; 95% CI 36.4-46.5) of the adolescents were in the socioeconomic class C. In relation to lifestyle, only 1.9% (95% CI 0.8-3.8) of the adolescents mentioned a smoking habit and 10.2% (95% CI 7.4-13.5) were alcoholic. Regarding nutritional status, it was observed that most adolescents (69.3%; 95% CI 65.1-74.2) were normal (Table 1). In assessing food intake, it was observed that the fat-soluble vitamin intake among adolescents was mostly insufficient. With respect to serum levels, a high percentage of retinol (76.8%), β -carotene (74.1%), α-tocopherol (88.1%) and 25(OH)D (50.9%) deficiency/insufficiency was observed.
Table I. Characteristics of adolescent students from Recife, northeastern Brazil, 2013
SES: socioeconomic status
BMI: body mass index
WC: waist circumference
CI: confidence interval
25(OH)D: 25 hydroxyvitamin D. Criteria of socioeconomic status classification-2013: descending order (being A the household with the highest purchasing power). Adequate retinol > 0.7 µmol/l. Adequate β -caroteno: > 0.9 µmol/l. Adequate -tocopherol > 12 µmol/l. Adequate 25(OH)D: > 72.4 nmol/l. Adequate food intake: vitamin A > 900 mcg/day; vitamin E > 15 mg/day; vitamin D > 15 mcg/day. Lost: BMI/age by inconsistences between the two measurements, food intake of vitamin A and E for inconsistencies information, serum retinol, β -carotene and α -tocopherol by biological material failure.
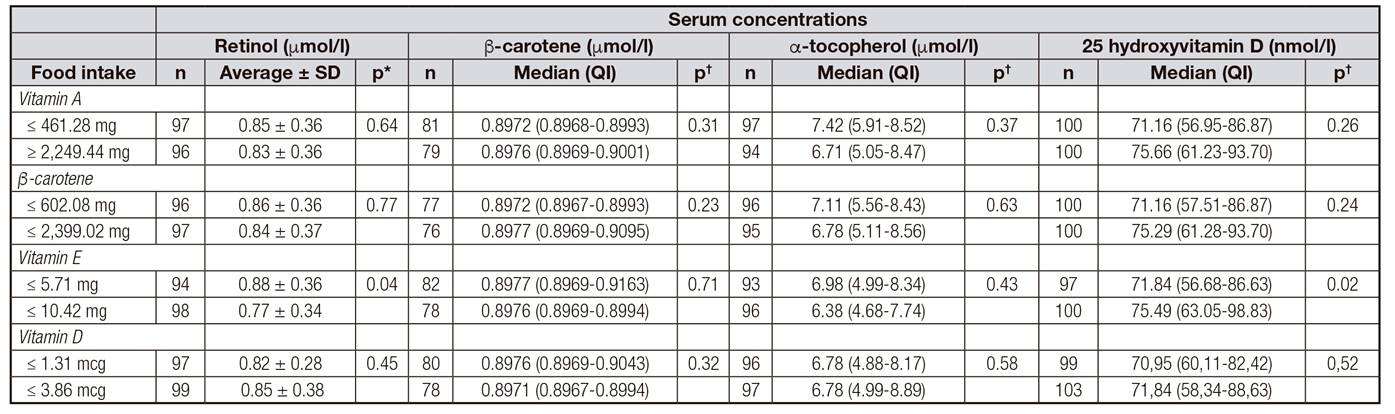
There was no significant difference between the consumption of vitamins A, D, E and β-carotene and serum levels of the respective fat-soluble vitamins, as shown in Table 2. However, children who ingested ≥ 10.42 mg/day of vitamin E had a significant decrease in serum concentrations of retinol and an increase in 25(OH)D.
Table II. Association between dietary intake and serum concentrations of fat-soluble vitamins of adolescent students, northeastern Brazil, 2013
SD: standard deviation
QI: quartile interval.
*Student's t-test unpaired.
†Mann-Whitney U test.
Food intake: used comparison between first and last quartiles.
As shown in Table 3, males had higher concentrations of retinol (p = 0.03), α-tocopherol (p = 0.02) and 25(OH)D (p <0.001). In relation to lifestyle, a significant increase in retinol was observed in adolescents who reported smoking (p = 0.03) and higher concentrations of 25(OH)D (p = 0.02) in individuals who drank alcoholic drinks. With regard to nutritional state, concentrations of retinol and α-tocopherol were significantly higher in overweight adolescents, while the serum levels of β-carotene and 25(OH)D decreased with an increased adiposity.
Table III. Serum concentrations of retinol, β -carotene, α -tocopherol and 25-hydroxyvitamin D according to lifestyle and nutritional status of adolescent students from Recife, northeastern Brazil, in 2013

SD: standard deviation
QI: quartile interval
SES: socioeconomic status
BMI: body mass index
*Student's t-test unpaired.
†Mann-Whitney U test
‡ANOVA
§Kruskall-Williams
Criteria of socioeconomic status classification-2013: descending order (being A the household with the highest purchasing power)
When factors associated with deficiency of fat-soluble vitamins were evaluated, it was found that the accumulation of body fat represented an increased risk of β-carotene (PR = 1.14) and 25(OH)D (PR = 1.38) insufficiency, while overweight exerted an opposite effect on alpha-tocopherol (Table 4). It was also noted that gender was a risk factor for the change in blood concentrations of vitamins, as female adolescents had a higher risk of lower values of α-tocopherol (PR = 1.11), while boys had a higher risk of 25(OH)D (PR = 1.41) inadequacy. No significant association between retinol inadequacy and the variables studied was found.
Table IV. Factors associated with inadequate serum retinol, α -tocopherol, β -carotene and 25-hydroxyvitamin D of adolescent students from Recife, northeastern Brazil, 2013

SES: socioeconomic status
BMI: body mass index
PR: prevalence ratio
CI: confidence interval
QI: quartile interval
*Chi-square test
†ANOVA
‡Fisher's exact test
Criteria of socioeconomic status classification-2013: descending order (being A the household with the highest purchasing power). Adequate retinol > 0.7 µmol/l. Adequate β-caroteno: > 0.9 µmol/l. Adequate α-tocopherol > 12 µmol/l. Adequate 25(OH)D: > 72.4 nmol/l.
DISCUSSION
The deficit in the consumption of micronutrients is quite frequent among adolescents 16. This has gained prominence after evidence demonstrated an association between the reduction in intake of some micronutrients, such as vitamins A, D and E, and an increased risk of diabetes, cardiovascular disease and cancer 17,18.
In this sense, this study found quite alarming data, since more than 90% of adolescents had a low intake of vitamins D and E, while approximately 50% had an insufficient intake of vitamin A. These data follow the literature, since Peters et al. 19 revealed an inadequate vitamin D intake of around 85% among adolescents, while Veiga et al. 20, in a national study, found that approximately 99% of individuals between ten and 18 years had an inadequate intake of vitamin E. This is similar to the results obtained by Silva et al. 21, who, evaluating the intake of vitamin E of children and adolescents, found that the vitamin intake corresponded to 12% of daily needs. There are reports of deficient intake 22, optimal intake 20 and intake above the recommended for vitamin A 21.
Reduced levels of fat-soluble vitamins in the bloodstream were also prevalent in this study, since adolescents have an inadequacy in more than 70% of the levels of β-carotene and α -tocopherol, approximately 50% of insufficiency in concentrations of 25(OH)D and 32.1% deficiency in retinol levels. Despite few reports with samples involving adolescents, the literature shows that the levels of 25(OH)D are, in fact, highly deficient 23, while retinol levels were insufficient in about 10-28% of adolescents 24,25, and the inadequacy of α-tocopherol is around 25% 26.
Although the literature demonstrates a relatively high frequency of these nutrients, this study showed higher values, reinforcing the importance of the development of more representative studies on populations in this age group.
It is important to note that adolescents are a group vulnerable to fat-soluble vitamin deficiency, and poor eating habits could exacerbate this deficiency. However, in this study, there was no significant difference between the consumption of vitamins A, D, E and their respective serum concentrations, which leads us to infer that, in addition to absolute values of consumed micronutrients, other factors could interfere with their blood concentrations.
The intake of vitamins below the recommended values for an extended period may be one of the main factors that could interfere with serum levels because the concentrations of fat-soluble vitamins remain consistent unless the individual consumes chronically inadequate amounts of these vitamins 27. In addition, the bioavailability of vitamins may also influence serum levels since the absorption of fat-soluble vitamins depends on the lipid components involved in the formation of the micelle and in pancreatic and biliary stimulus. It also depends on diet composition: certain lipids and other nutrients may negatively interfere with the absorption of vitamins 28.
In this study, adolescents who consumed higher amounts of vitamin E had a significant decrease in serum retinol concentrations, possibly because a high amount of vitamin E may inhibit the absorption of β-carotene or its conversion into retinol in the intestine 29. It was also noted that a higher intake of vitamin E seems to positively affect the increase of 25(OH)D. However, there are no reports elucidating this finding, which leads us to infer that vitamin E intake could positively affect the bioavailability of vitamin D. However, more studies are needed to evaluate and clarify the probable mechanism of interaction between these two vitamins. In addition, it is suggested that in evaluating the consumption of fat-soluble vitamins, the factors that may interfere in the bioavailability of these micronutrients be considered.
In the sample studied, boys had significantly higher values of retinol, α -tocopherol and 25(OH)D. Girls had a higher risk of deficiency of α -tocopherol, whereas boys had a higher risk of 25(OH)D inadequacy. This difference may be due to possible differences arising from the pubertal development of the genders. Hormonal factors might be responsible for these differences, since vitamins are highly active compounds associated with the activity of all regulatory chains of the gonadotropic pituitary function and participate in the synthesis of corticosteroids and sex hormones 30.
The lower concentration of β -carotene observed in adolescents from a higher socioeconomic level shows that purchasing power may interfere with diet choices, because, as the β-carotene is considered as a relevant indicator of fruit and vegetable intake 28, adolescents would possibly show a reduced consumption of these foods. This is because, unlike retinol, in which blood levels are more stable and maintained because of deposits, β-carotene concentrations are more variable, probably because of fluctuations in the carotenoid intake 31.
Regarding the variable lifestyle, adolescents who reported smoking had higher concentrations of retinol, and those who did not smoke had a higher risk of insufficiency 25(OH)D levels. In addition, this study also found that adolescents who drank alcohol had higher serum concentrations of vitamin D. However, it should be noted that the sample of adolescents who smoke and drink was very small, which shows the need for further research to investigate whether this association is true or if it was just one confounding factor of this study.
Studies demonstrated an inverse association between concentrations of fat-soluble vitamins and overweight in children and adolescents from both genders 32. Evidence suggests that a decrease in the concentration of fat-soluble vitamins in the plasma may occur in obesity due to a lower intake of these nutrients and/or to a greater deposition in the adipose tissue. By being soluble in fats, they are deposited in adipocytes and thus decrease bioavailability in individuals with adiposity excess 35. Thus, a higher adiposity is associated with increased levels of free radicals, leading to the reduction of the concentrations of antioxidant liposoluble vitamins in an attempt to reduce the oxidative stress resulting from overweight 34.
However, this study found that overweight adolescents had an increase in the concentrations of retinol and α-tocopherol and a decrease of β-carotene and 25(OH)D concentrations when compared to individuals with a normal weight. These findings differ from the literature, since there are reports of a decrease of vitamins D, E and β-carotene in the bloodstream in overweight individuals 35,36, whereas retinol presents conflicting data, since some authors have reported an increase in this vitamin with an increase in adiposity 35 and others show no association between retinol and obesity 25.
These differences could be attributed to the storage locations of fat-soluble vitamins in the human body, for about 80-90% of the retinol is stored in the liver, while carotenoids and vitamins D and E are ideally stored in the adipose tissue 37. That is, the concentration of retinol would depend primarily on liver reserves and would exert less influence to fluctuations of adipose tissue.
A possible explanation is that, due to the inflammatory process resulting from overweight, there would initially be a greater recruitment of antioxidant vitamins (A, E and carotenoids) in an attempt to neutralize the free radicals produced, thus increasing their concentration in the bloodstream. β -carotene, as well as having an antioxidant function and the possibility of being diverted for conversion to vitamin A in the liver, would likely decrease its concentrations. Another factor that could influence the decrease in the concentration of these vitamins would be the intensity and the duration of the inflammatory process. However, as this study did not use biochemical markers, it prevented us from confirming the degree of inflammation that adolescents have.
Regarding vitamin D, the reduced values in obese individuals could be due to a higher deposition in adipocytes and a lower recruitment of this vitamin. It has been speculated that a deficiency of this vitamin could trigger the accumulation of body fat, because, with the deposit of vitamin D in adipocytes, its lower bioavailability would trigger a cascade of reactions by the hypothalamus, which would result in an increased hunger feeling and a reduced expenditure of energy 38. In addition, a decrease in vitamin D levels would increase the parathyroid hormone, which in turn would cause an elevation in intracellular calcium levels in adipocytes, which could act on the increased expression of fatty acid synthase, a key enzyme to the regulation of lipid deposition as well as to the reduction of lipolysis 39.
Upon evaluating the concentration of fat-soluble vitamins in adolescents with weight excess, according to gender, boys showed an increase in the concentrations of retinol and α-tocopherol and a reduction of β-carotene and 25(OH)D concentrations as adiposity increased. In girls, only α-tocopherol was high with overweight. These variations may be caused by hormonal influences on the weight development process, but they may also be due to differences existing in different body fat deposition areas. Women deposit more fat in the femoral and gluteal region, and men deposit more fat in the central region, which configures a less inflammatory profile for females 40. Thus, the mobilization of vitamins to the bloodstream would be less intense in girls compared to boys with an increase in adiposity.
With regard to the limitations of the study, because it was a cross-sectional study, it was not possible to guarantee causal relations, and confounding variables may have affected the reported associations. In addition, biochemical markers monitoring the presence and intensity of oxidative stress were not used, which prevented us from evaluating the changes in concentrations of vitamins related to the inflammatory process in the presence of overweight/obesity.
Evaluated adolescents have a potential risk of inadequacy of fat-soluble vitamins, with a significant deficit both in consumption and serum levels. Although factors such as gender and overweight interfere with serum concentrations, the metabolic behavior of vitamins A, D, E and β -carotene appears to differ according to different situations. Thus, it is necessary to understand the biochemical pathways that each vitamin takes, particularly with respect to increased adiposity, especially because it is one of the most prevalent nutritional disorders among adolescents, and liposoluble vitamins appear to be negatively related to excess of weight.
These findings point to the fact that the consumption of vitamin E appears to influence the metabolism and bioavailability of vitamin D, but more studies are needed to elucidate this association. This study demonstrates that the behavior of vitamins A, D and E in adolescents needs more research in order to identify the status of these nutrients in this population group, so that specialized and focused strategies to reduce these deficiencies are adequately prepared.

