










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Low birth weight (LBW, births under 2,500 g) is one of the most important health indicators as it affects the viability and healthy development of neonates1. LBW has been associated with a myriad adverse health outcomes across the life-span, including cardiovascular disease 2, premature mortality 3 and cognitive problems such as autism 4 and depression 5,among many others 6. In addition, the negative effect of foetal growth restriction could be maintained over generations 7 as a consequence of epigenetic mechanisms 8.
Even in high income countries, social inequalities in perinatal health persist 9,10,11,12. These differences can increase in times of economic recession as the result of a combination of personal, family and community factors through a decrease in material resources, a deterioration of environmental conditions, and an increase in psycho-social stress 13. Based on a global analysis, socioeconomic inequality within a country is more associated with differences in health indicators than is the absolute wealth or median income of that country 14.
After decades of economic growth, Spain has been one of the European countries most affected by the economic crisis, which started in the USA in August 2007, and affected Spain from 2008 with a growing spread of poverty and social inequality 15,16. To evaluate the negative impact of the economic recession of 2008 on perinatal health is challenging since, during the preceding decade of sustained economic growth, there was a general deterioration in neonatal indicators (except perinatal deaths) both in Spain and in most European countries. Such deterioration, which has been explained as a consequence of growing predominance of primipara mothers with an ever-increasing age at first maternity, an increase in multiple pregnancies as a result of the rise in assisted reproductive techniques (ART), and high rates of obstetric intervention 17. Specifically, over the two decades preceding the economic crisis, Spain had the greatest increase in LBW among the European countries 18, without a parallel increase in preterm births as was the case in other countries 19. However, recent studies of the Icelandic 20, Irish 21, Greek 22 and also Spanish 23,24 populations, associate the current economic crisis with a worsening of perinatal health indicators, which are independent of the described trends before the recession. The aim of this study is to evaluate if the current economic crisis is associated with increased inequalities in LBW according to the maternal socioeconomic profile.
MATERIAL AND METHODS
The data analysed come from the Spanish Vital Statistics which collects information on all neonates in Spain who are declared in the civil register via the Boletín Estadístico de Parto (Statistical Birth Bulletin, SBB). Since 1996, the SBB includes, in addition to weight at birth and gestational age of neonates, the nationality of the parents and, after review in 2007, new variables such as marital status (whether the mother and father live together), the education level of both parents and the type of delivery. Validation studies 25 have concluded that the data provided by the SBB is reliable when compared to hospital registers, albeit less so for certain categories of foreign mothers.
Compared with Spanish mothers, those coming from the three main migrant origin groups in Spain (i.e., Latin America, the Maghreb and Eastern Europe) have very different lifestyles and eating habits as well as their own reproductive patterns which associate with significant differences in pregnancy outcome 26,27. Furthermore, as in other high-income countries 16, delayed maternity in Spain is linked to a greater access to assisted delivery techniques and the resulting increase in multiple pregnancies, such that it is estimated that 70% of twin pregnancies are due to fertility treatment 28. The population analysed has therefore been limited to live single births to mothers born in Spain. The selected years analysed are 2007 (the year before the current economic crisis and the first for the new SBB register), 2009, 2011, 2013 and 2015 (the last year available). From an initial total of 2,264,271 new-borns in Spain for the selected years, the final analysed sample corresponds to 1,779,506 single births to Spanish mothers, which represents 78.6% of the initial sample and 97.5% of available data for Spanish mothers (Fig. 1).
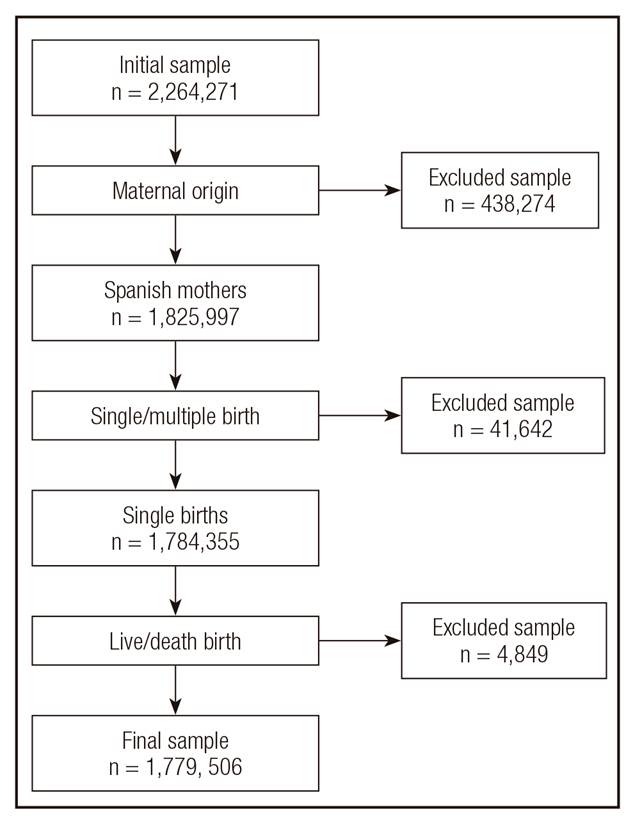
Figure 1. Inclusion/exclusion criteria of the analysed sample (years 2007, 2009, 2011, 2013, and 2015, data from SBB).
As mentioned above, there were temporal changes in available maternal-foetal variables. We recoded the original variables included in the SBB. Maternal occupation was recoded into the categories professionals, administrative employees, Service Sector workers, skilled workers, unskilled and Tertiary Sector workers, students and housewives. Maternal education level was recoded into university education, secondary education and primary education; maternal age into groups of mothers under 20, 20-24, 25-29, 30-34, 35-39 and 40 or over; marital status into married and living with a husband, living with a stable partner, living without a partner, including widows, divorcees and separated mothers; maternal place of residence into rural (less than 10,000 inhabitants) and urban; the number of live births into the categories of primipara and multipara mothers; weeks of gestation into preterm births (born at less than 37 weeks), term births (37-41 weeks), and post-term births (42 weeks or more); birth weight into low birth weight (LBW less than 2,500 g), normal birth weight (2,500-3,999 g) and macrosomia (equal to or over 4,000 g). The analysis also includes the original variable type of delivery (vaginal or caesarean section). For each of the variables indicated, a category of missing was established. In the case of variables of maternal occupation and education level, there is a sharp drop in the percentage of missing between 2009 and 2014, which was due to their non-inclusion in certain Autonomous Communities (political and administrative regions of Spain) for unknown reasons.
We analysed the data for a possible increase in social disparities, both in prevalence and relative risks (RR) of LBW, during the economic crisis. We assigned 2007 as the reference year the year before the beginning of the recession in Spain and its impact on the population. Poisson regressions were performed using LBW as the dependent variable, and maternal occupation and education level the independent ones. Given the increased risk of macrosomia reported in previous studies in relation to the economic crisis 23, normal weight was used as the reference category. The reference categories for maternal occupation and education level were for professional women and mothers with university studies respectively. The analyses were stratified by parity, since an interaction between both maternal occupation and education level on LBW was found. Three model specifications were compared for each parity category: model 1 presents unadjusted RR; model 2, RR adjusted only for gestational age (now included as a continuous variable) given the strong link between gestational age and birth weight 1; and model 3, RR adjusted for the remaining maternal-foetal variables, in addition to gestational age. To avoid unnecessary adjustment 28, model 3 only includes such maternal-foetal variables that significantly changed the association between LBW and occupation or education level. Education level and type of delivery were identified as adjustment variables for maternal occupation, while aside from gestational age no other maternal-foetal variable was identified for maternal education (so only models 1 and 2 were compared in Results for this second independent variable). Finally, a sensitivity analysis was carried out including and excluding the categories of missing information for both dependent variables. No significant differences were found and models without categories of missing are shown.
RESULTS
Table I shows temporal trends in the maternal-foetal variables analysed for the selected years. During the period analysed, Spanish women who became mothers did so at an increasingly older age (44.0% at 35 or over in 2015) and with a growing predominance of highly qualified professional (29.4% were professionals in 2015) and highly educated women (35.8% had university degrees that same year).
Table I. Temporal trends in maternal-foetal variables (live single births, Spanish mothers, years 2007, 2009, 2011, 2013, and 2015, data from SBB)


CS delivery, caesarean section delivery; LBW, low birth weight.
*Not available data.
Although the majority of these women were married or had a stable partner, the proportion of women without a stable partner grew significantly (up to 17.9% in 2015). Primiparity remained stable at 51%, with a slight drop in 2015. The number of Caesarean sections remained above 25%, with a slight drop in 2015. The prevalence of preterm births fell steadily from 6.1% to 5.4% (the same as post-term births, from 2.6% to 1.4%), while LBW rose from 5.9% to 6.1% and macrosomic births remaining at around 5%.
Figure 2a and Figure 2b (Tables Ia and Ib in the Annex) show, by parity and year of birth the prevalence of LBW and the values for RR of having a new-born with LBW according to maternal occupation, with professional women the category of reference. Figure 3a and Figure 3b (Table IIa and Table IIb in the Annex) show the prevalence of LBW and RR by parity and year of birth according to level of maternal education, with mothers with university studies the category of reference.

Figure 2a. Prevalence, unadjusted and adjusted relative risk of LBW by maternal occupation and year of birth in primipara mothers. Model 1, unadjusted; model 2, adjusted for gestational age; model 3, adjusted for maternal education, type of birth, and gestational age (live single births, Spanish mothers, data from SBB).
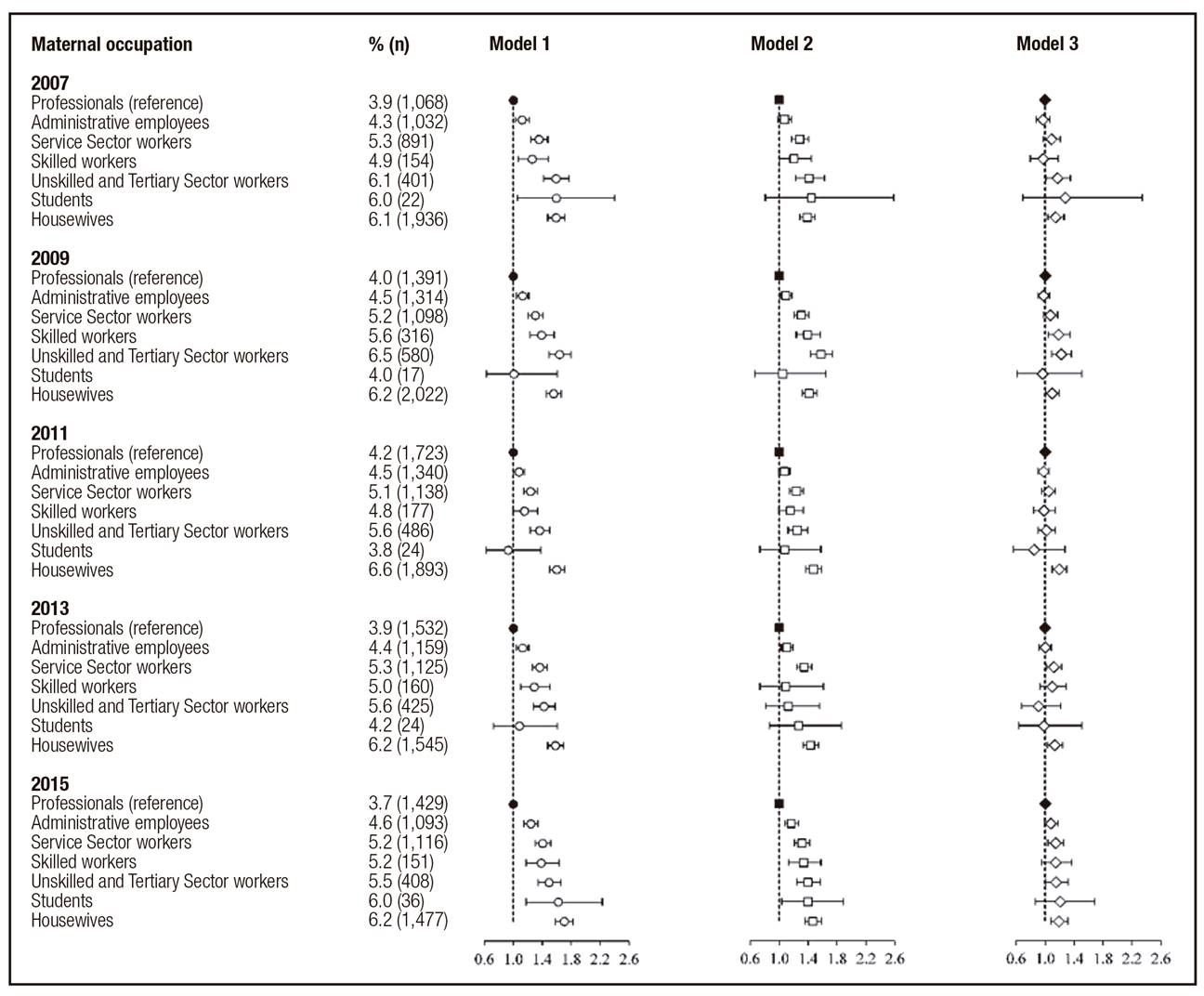
Figure 2b. Prevalence, unadjusted and adjusted relative risk of LBW by maternal occupation and year of birth in multipara mothers. Model 1, unadjusted; model 2, adjusted for gestational age; model 3, adjusted for maternal education, type of birth, and gestational age (live single births, Spanish mothers, data from SBB).
Among primipara mothers (Fig. 2a), the prevalence of LBW rose in all maternal occupation categories between 2007 and 2015, being greater among women with less skilled work and highest among housewives (up to 9% in 2015). Among multipara mothers (Fig. 2b) the prevalence of LBW was again greater among women with less skilled work and highest among housewives, for this latter group always over 6%. This prevalence was less compared to primipara mothers and rose over the period 2009/2011 only to fall later. Disparities may be appreciated in LBW according to maternal occupation both in model 1 (unadjusted) and in model 2 (which includes only gestational age), both for primipara and multipara mothers. However, when adjustment variables are included (model 3), the RR of having a LBW newborn compared with professional mothers fell sharply, remaining significant only among housewives for all years (and for unskilled workers in 2013), and for all or most occupation categories (except students) in 2009, albeit with very low RR (around 1,0 and 1,1). A slight temporal rise can be seen in disparities in the risk of LBW among the reference category and housewives for primipara mothers in 2009 (RR = 1.20, 95% IC = 1.11-1.29) and for multipara mothers in 2011 (RR = 1.19, 95% IC = 1.10-1.30).
Regarding maternal education, the prevalence of LBW among primipara mothers increased over the period in all categories (Fig. 3a), with the highest prevalence among mothers with primary education (up to 9.6% in 2015). Among multipara mothers (Fig. 3b), LBW prevalence was again lower (maximum among housewives: 8.2% in 2015) and the increase was less evident during the economic crisis, although disparities between categories remained. After adjusting for gestational age (model 2), the RR fell compared with the unadjusted model, but remain significant. Both for primipara and multipara mothers and for all the years analysed the adjusted RR of being born with LBW were significantly higher among mothers with primary and secondary education than among those with university education. Adjusted RR for education categories were greater than for occupation categories, being greater among multipara mothers than primipara ones (the opposite to what happens with occupation). The tendency is also clearer towards a temporal increase in disparities in adjusted risk of being born with LBW according to maternal education in 2009, both for primipara (RR = 1.39, 95% IC = 1.30-1.49) and multipara (RR = 1.81, 95 % IC = 1.67-1.97) mothers.

Figure 3a. Prevalence, unadjusted and adjusted relative risk of LBW by maternal education and year of birth in primipara mothers. Model 1, unadjusted; model 2, adjusted for gestational age (live single births, Spanish mothers, data from SBB).

Figure 3b. Prevalence, unadjusted and adjusted relative risk of LBW by maternal education and year of birth in multipara mothers. Model 1, unadjusted; model 2, adjusted for gestational age (live single births, Spanish mothers, data from SBB).
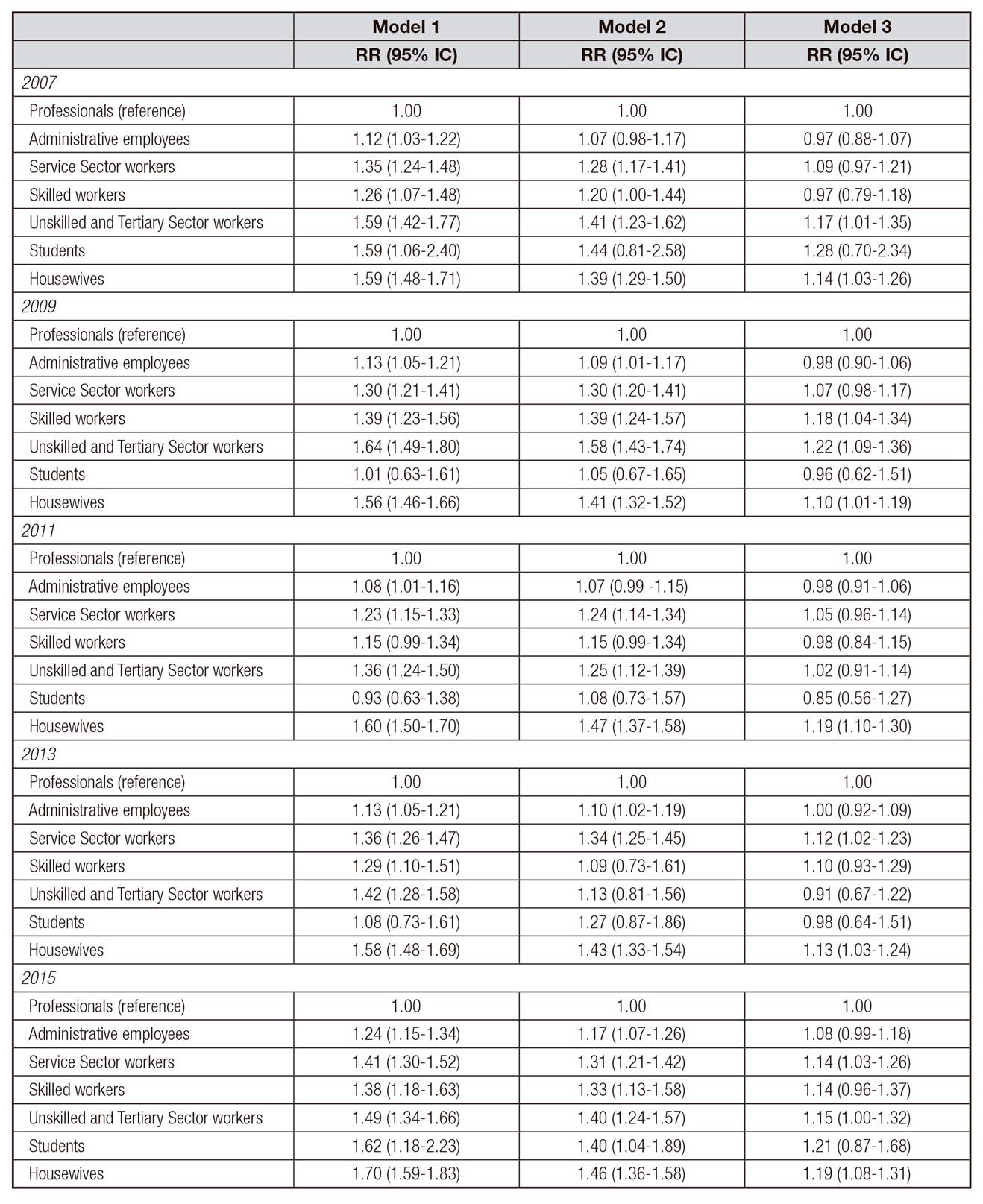
Annex. Table Ia. Relative risk and 95% confidence interval for LBW by maternal occupation in primipara mothers (live single births, Spanish mothers, years 2007, 2009, 2011, 2013, 2015, data from SBB)

RR, Relative risk; 95% IC, 95% confidence interval.
Model 1, unadjusted; model 2, adjusted for gestational age; model 3, adjusted for maternal education, type of delivery, and gestational age.
Annex. Table Ib. Relative risk and 95% confidence interval LBW by maternal occupation in multipara mothers (live single births, Spanish mothers, years 2007, 2009, 2011, 2013, 2015, data from SBB)
RR, Relative risk; 95% IC, 95% confidence interval.
Model 1, unadjusted; model 2, adjusted for gestational age; model 3, adjusted for maternal education, type of delivery, and gestational age.
Annex. Table IIa. Relative risk and 95% confidence interval for LBW by maternal education in primipara mothers (live single births, Spanish mothers, years 2007, 2009, 2011, 2013, 2015, data from SBB)
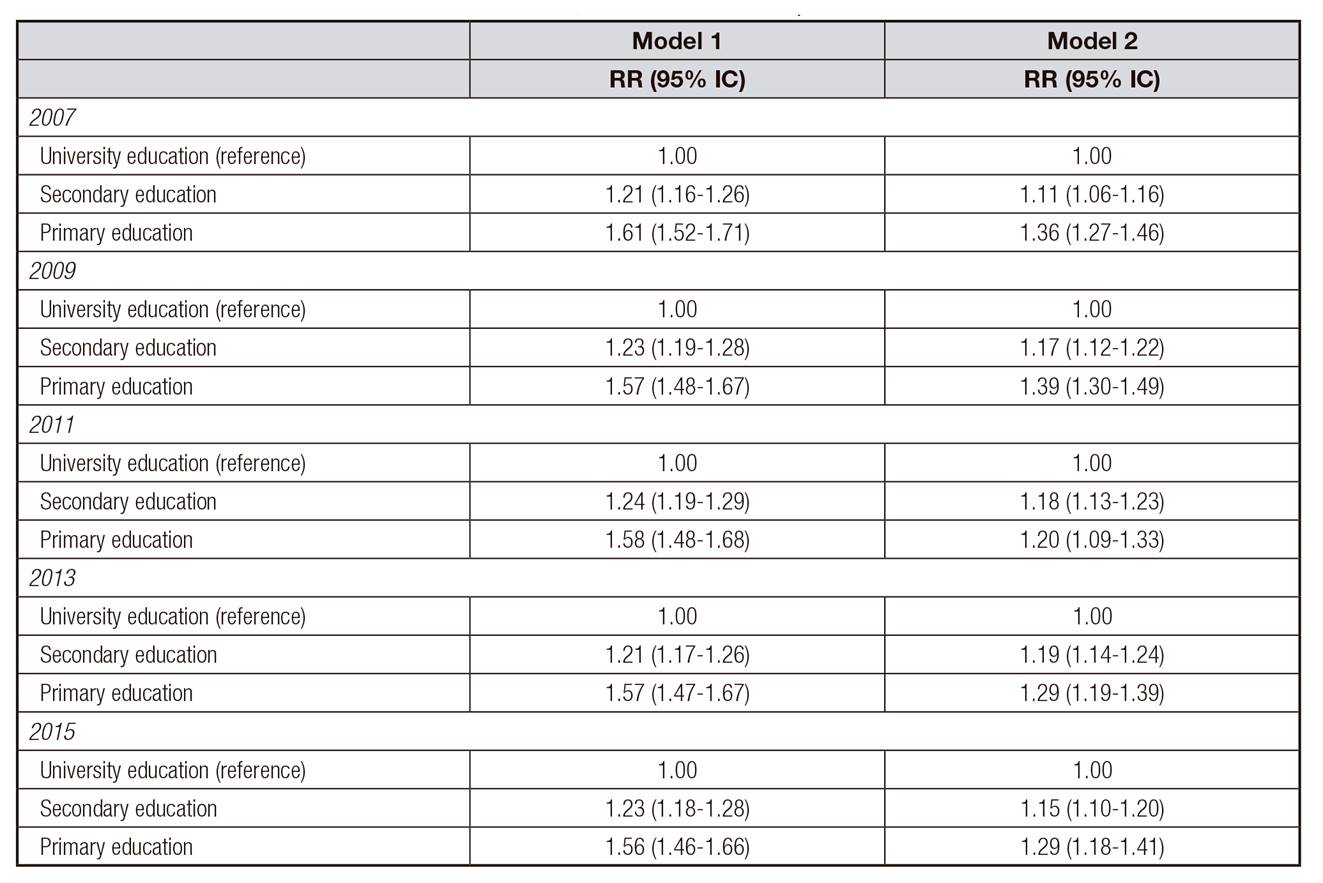
RR, Relative risk; 95% IC, 95% confidence interval.
Model 1, unadjusted; model 2, adjusted for gestational age.
Annex. Table IIb. Relative risk and 95% confidence interval for LBW by maternal education in multipara mothers (live single births, Spanish mothers, years 2007, 2009, 2011, 2013, 2015, data from SBB)


RR, Relative risk; 95% IC, 95% confidence interval.
Model 1, unadjusted; model 2, adjusted for gestational age.
CONCLUSION
This study shows that during the years of economic crisis in Spain there has been an increase in the prevalence of LBW, and a persistence and increase of social inequalities in LBW (according to adjusted RR). At the same time, a change can be observed in the profile of women having children during this period, with a greater contribution of highly qualified professional women and those with high levels of education. Given that these social categories are linked to good birth outcomes, it is possible that the persistence of social inequalities reported in this study hides or underestimates the negative effect of the crisis on pregnancy on the prevalence and risk of LBW. Our study also shows that differences in birth weight are more clearly connected with the maternal education level than with maternal occupation. The limitations of this study include the fact that the analysis carried out was limited to the information compiled by the SBB, which does not include variables which are relevant for evaluating gestation conditions and pregnancy outcome, such as maternal health, anthropometry, eating habits, weight gain during gestation, and stress levels. On the other hand, the SBB provides data at the national level which allow a sound and reliable evaluation of temporal trends in maternal profile, obstetric practices, and perinatal health associated to demographic, social and economic changes in the country.
The results confirm the persistence of the social inequalities in perinatal health described before the crisis 29,30, as well as the negative effect of the crisis 23,24 over a wider period (2007-2015) than that observed previously. At the same time, our results show how the economic crisis may have deepened some tendencies previously seen in the profile of Spanish mothers 31, intensifying the presence of women with better socio-economic positions, or in other words, limiting the reproductive opportunities for the most socio-economically vulnerable women. In fact, the decrease of fertility in the country since 2008 was one of the more immediate consequences of the economic crisis, a decrease to which Spanish women with a lower socio-economic status, along immigrant residents are primarily contributing.
Spanish primipara mothers are increasingly older, and with greater marital stability 31. Delayed maternity has been associated with a worsening of perinatal indicators, with increasing access to ART (and consequently an increased rate of multiple pregnancies), and with increasing obstetric interventionism 32. Analyses of the Spanish population for the period of the current economic crisis 24 confirm that the delay in the age at first maternity is a significant adjusted factor for delayed foetal growth, but with a very limited clinical impact. This could be due to the fact that delayed maternity is linked to greater material resources and level of education, greater marital stability, and better maternal care, which, ultimately, all favour better perinatal indicators 33.
Despite these trends in the socio-economic profile of Spanish, we must underline that the results show that the prevalence of LBW increased for all socio-economic categories of mothers during the economic crisis, in a sustained way among primipara mothers, but only during the worst years of the recession (2009 and 2011) among multipara mothers. Thus, for example, among primipara mothers the prevalence of LBW increased among housewives by 18.4% between 2007 and 2015, but also increased by 10.7% among professionals, and even increased more among women with university education than among those with primary studies (10.7% compared with 7.8%, respectively). These findings point to the general impact of the economic crisis on gestation -as has been described in other European countries 34- through increased maternal stress, a hypothesis explored in Varea et al. (2016) 24. Clearly, following a period of economic prosperity, the Spanish population have experienced an unexpected and prolonged period of psychological uncertainty since 2008, which has affected almost all social sectors, independently of an immediate or major drop in their living conditions 35. Future population analyses of wider temporal series will allow an evaluation of the impact of the economic crisis on perinatal health indicators, independent of those derived from previous trends in the maternal profile and the increase in obstetric intervention 23,31.
The results also show that disparities in the risk of having a new-born with LBW are more clearly linked to differences in the maternal education than to occupation, as well as their increase during the economic crisis. After adjusting for education, type of delivery and gestational age, the RR of having a new-born with LBW among occupation categories as compared with professional mothers lost significance or were very low (RR ≈ 1.1, for housewives and the other categories during the worst years of the economic crisis). On the other hand, adjusted (only for gestational age) RR of having a new-born with LBW for women with primary or secondary education remained significant for both categories and all years, as compared to university graduates. Our analysis found that maximum disparities in LBW were by education level among multipara mothers, with RR between 1.6 and 1.8. Among multipara mothers, the educational gradient represents the extremes of the spectrum of multiple births, with well-qualified women, with good economic resources and marital stability predominantly having two live births as opposed to mothers with a low level of education and limited resources, who became mothers at a young age and had families with three or more births (data not included). As has been described in other European countries 36, these mothers are those taking responsibility for managing very limited family budgets and for coping with the deterioration of the domestic economy during the recession.
To sum up, the results of this study confirm that maternal education highlights the social inequalities and their possible impact on pregnancy and birth outcome better than maternal occupation 33. Education, in part, determines occupational level, but education also favours healthy maternal habits, including earlier and better prenatal care, appropriate weight gain during pregnancy, reduced parity, and greater marital stability 37,38. A higher level of maternal education is considered the clearest vehicle for the positive intergenerational transmission of human capital and for the intergenerational reduction of social inequalities 39.

