










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Home enteral nutrition (HEN) is a therapy for stable patients who need long-term care without the need of hospitalization 1. HEN is a model of care of growing importance, aimed at optimizing diet transition, improving patient's quality of life and reducing treatment-related costs compared with hospital care 2.
The use of HEN has increased worldwide. In Italy, the incidence (per million population per year) and the prevalence (per million population) of patients receiving HEN was 223.4 and 279.4, respectively, between 2001 and 2005 3. In Spain, from 1999 to 2010 the incidence of patients receiving HEN was three per million inhabitants 4. In Poland, the number of patients with HEN increased from 5.4 to 46.6 per million inhabitants in five years (2008-2013) 5. However, in Brazil, there are no data available on the characteristics of individuals treated with HEN provided by the Unified Health System, but this is not an impediment to conducting cross-sectional surveys and without intervention on the topic. A prevalence study conducted in Federal District, Brazil, in Zaban and Novaes 6 showed a prevalence of 175.64 cases per million inhabitants and an incidence of 147.98 cases per million inhabitants per year in 2005.
In Curitiba, Brazil, the Nutrition Assistance Program for People with Special Dietary Needs (PAN) began in 2006 with the objective of providing nutritional assistance and tools for nutritional care of HEN patients. The program is a milestone for the Brazilian Unified Health System and has been recognized internationally as a model for HEN care.
The knowledge of epidemiological data of patients receiving HEN is necessary for the development of effective and cost-effective public policies. Thus, the objective of this study was to determine the frequency and the situation of patients on HEN, in the capital city in the south of Brazil.
MATERIALS AND METHODS
We retrospectively analyzed the data of adult patients on HEN between January 2006 and December 2015, beneficiary of the PAN. The study was approved by the Ethics Committee of the Curitiba Secretary of Health and by the Ethics Committee of the Federal University of Paraná (49265615.1.0000.0102/2015).
Data were collected from the medical records in public health centers of the city. For the purposes of analysis, data were collected in the first and last home visits of all patients, adults and elderly, registered in the PAN. The outcomes were categorized as discharge, continuation in PAN or death.
Baseline diagnosis and associated diseases, previous HEN as well as HEN access were evaluated.
STATISTICAL ANALYSIS
The survival curves were evaluated using the Kaplan-Meier method, defined as the time interval between PAN inclusion and death. The follow-up time was defined as the median time intervals, and the variable of interest was death from any cause. "Survivors" were defined as those patients who were either withdrawn or discharged from the PAN. Life table analysis and Kaplan-Meier curves were performed to assess the duration of the HEN. The Cox proportional hazards analysis was used to assess which variables were correlated with survival. Statistical data were generated with the IBM SPSS Statistics 22.0 (Chicago, IL, USA). All statistical tests were two sided, and p < 0.05 was used to indicate statistical significance.
RESULTS
The study included 1,231 individuals on HEN. Curitiba's population was estimated to be 1,893,997 in 2015, distributed in a territorial area of 435,036 km² (population density of 4,027 inhabitants/km²). Most of the population are adults (87.3%) and women, and the most prevalent age group is 30-34 years old.
Figure 1 depicts the frequency of patients on HEN, including total number, the number of survivors and the number of deaths from 2006 to 2015. There was an exponential increase (425%) in HEN in the years studied, with a peak in 2013. The number of deaths was considerably higher compared to survivors from 2006 to 2013, although these rates were similar in 2015.

Figure 1. Frequency of patients (total number, number of survivors and number of deaths) on home enteral nutrition in a ten-year period in Curitiba, Brazil.
Mean age was 66.7 ± 17.6 years; 68.0% (n = 837) were elderly. The majority of the sample was male (n = 670; 54.4%). Nasogastric tube was the main route of administration (38.3%). Diet prescription by dietitians at the hospital was mostly tube feeding formula (50.6%), whereas at home, patients were mostly prescribed a blended diet (38.6%) (Table I).
Table I. Characteristics of the home enteral nutrition prescribed to patients (n = 1,231) in Curitiba, Brazil, from 2006 to 2015

*Missing data n = 3.
†Missing data n = 167.
‡Missing data n = 51.
§Missing data n = 5.
ǁMissing data n = 12.
¶Number of patients whose home enteral nutrition was performed by a caregiver; missing data n = 10.
The most prevalent diagnoses were neurological diseases (46.4%), especially stroke (28.8%) and Alzheimer disease (9.2); cancer (33.6%), especially head and neck (14.3%) and esophagus (8.9%); and trauma (7.1%) (Table II). Among comorbidities, there was a high prevalence of systemic arterial hypertension (586, 47.8%) and diabetes mellitus (243, 19.8%).
Table II. Prevalence of diseases (International Classification of Diseases, 10th revision, ICD-10) in patients (n = 1,231) on home enteral nutrition in Curitiba, Brazil, from 2006 to 2015

Neurological diseases were the most prevalent in every year of the study period, except in the year 2015, where cancer was the most prevalent. The other diseases showed a similar frequency throughout the years, except for kidney diseases that increased in the year 2015 (Fig. 2).

Figure 2. Descriptive time series of the most prevalent diagnoses of patients (n = 1,231) on home enteral nutrition in Curitiba, Brazil, between 2006 and 2015.
Of the 1,231 patients on HEN, 65.1% (n = 801) died, 21.0% achieved full oral nutrition, 5.9% continued on HEN, 5.3% moved to another city and in 2.9% the outcome was not reported. Figure 3 shows the Kaplan-Meier survival curves for all patients. Overall, the median survival was 180 days (95% CI: 163.6-193.4). A significant difference (p > 0.05) was found between the survival of patients with neurological diseases (median survival of 180 days), cancer (median survival of 210 days) and other diseases (median survival of 150 days).

Figure 3. Kaplan-Meier overall survival curve in patients on home enteral nutrition (n = 1,231) in Curitiba, Brazil, between 2006 and 2015.
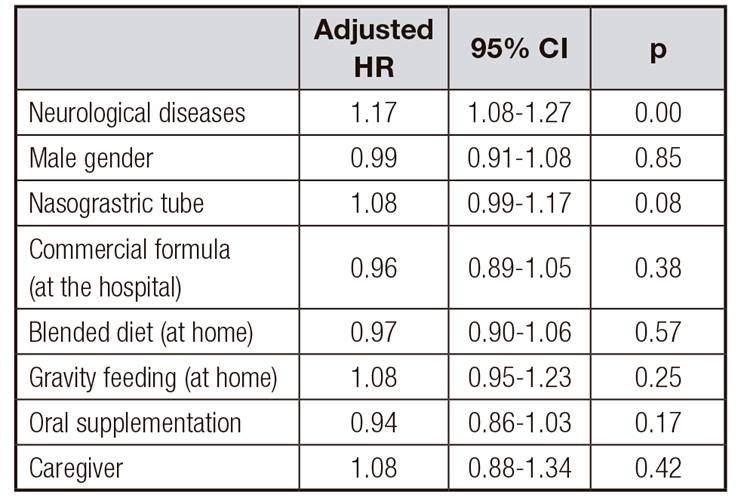
Cox proportional hazards model was employed, assuming duration of HEN as exposure time and 801 deaths as failure endpoint. This analysis showed that neurological disease was an independent risk factor for mortality in patients on HEN. However, gender, nasogastric tube, commercial formulas during hospitalization, blended diet at home, gravity feeding, oral supplementation and presence of a caregiver were not risk factors for mortality in HEN patients (Table III).
DISCUSSION
This study shows the frequency of patients on HEN in Curitiba, Brazil, from 2006 to 2015. The number of HEN patients considerably increased during this period; however, it was not possible to establish the prevalence of HEN patients, especially due to underregistration of cases, particularly of those with less severe conditions, and also because health records were not in electronic format, contributing to missing data.
In some countries, such as Poland, Great Britain, Spain and Italy, epidemiological data of HEN patients are annually recorded. However, data on HEN from Latin American populations are scarce in the literature. In Brazil, Zaban and Novaes 6 reported an increase in both incidence and prevalence of HEN patients over a five-year period in the Federal District.
Santarpia et al. 1 reported an increase from 355 patients on HEN in 2005 to 1,165 in 2012. Nevertheless, unlike our study, the authors considered not only patients on HEN, but also on parenteral and oral nutrition. Mundi et al. 9, in a prevalence study conducted in 2013 in the United States, showed a prevalence of 437.88 HEN patients per million population; in adults, this number was 248.85. The number of patients on HEN increased considerably from 1992 to 2013 (231.4%). In Spain, De Luis et al. 4 reported that the prevalence of HEN patients increased from 9.52 in 1999 to 30.0 in 2010 per 100,000 inhabitants. In Poland, the prevalence of HEN increased from 5.4 to 47.6/1,000,000 inhabitants from 2008 to 2013 5.
In our study, most of the patients were men (54.4%), similarly to other studies 4,5, but different to others 3,11,12.
In this study, the mean age of the sample was 66.7 years, like the study by De Luis et al. 4 (68.5 years), the study by Klek et al. 5 (61.4 years) and others 11,12. In our study, the elderly accounted for 68.0% of the sample. Wong et al. 2, in a systematic review, showed that most patients of HEN-related studies were elderly.
Although most patients were on long-term enteral nutrition support, the nasograstric tube was the main route of administration (38.3%). In seven years of follow-up, Morelo et al. 3 also demonstrated that nasograstric tube was the most predominant feeding route. A long period on nasogastric feeding can cause an exponential increase in the risk for complications (e.g., infection and mechanical complications) in the access site. On the other hand, European studies 5,11 have shown that gastrostomy tube and jejunostomy tube were more commonly used for long term enteral nutrition therapy 5,11. However, although both gastrostomy and jejunostomy are safe ways to provide food to patients, placement of these long-term access tubes requires surgery and is expensive in Brazil.
In our study, it was shown that most dietitians prescribe commercial diets at hospital discharge of patients with HEN (50.6%). It is known that the use of commercial products in HEN reduces the frequency of hospitalization for infections and pneumonia of home patients 2. That would also reduce costs with HEN. Nevertheless, there is a low subsidy for these products, and the Brazilian Unified Health System provides limited funding and use strict criteria for dispensing these products. In this regard, patients with severe malnutrition, patients with cancer as primary diagnosis, and those with degenerative diseases are considered as a priority by the Unified Health System and the PAN. If, on the one hand, commercial formulas are the "diet of choice" for enteral nutrition support, on the other hand, a blenderized diet was prescribed to 38.6% of patients on HEN. Ginzburg et al. 12 warn that little attention has been paid to the lack of communication between the hospital setting and the community. Since most HEN patients have chronic diseases, homemade diet can be a cheaper alternative for the patients, their families and the health system as well 14. It is worth mentioning, however, that although homeblend feedings are a very convenient solution, the risk of tube clogging and underfeeding due to low protein/energy value of the diets should be considered. In the present study, there was no association of homemade diet with survival.
Neurological diseases, especially stroke (28.8%), were the most prevalent in our sample (46.4%). Dysphagia is usually the indication for HEN in these diseases. Similar prevalence of neurological diseases has been reported by other authors 3,4,5,10,13. Santarpia et al. 8 showed that neurological diseases increased 327% in adults and 287% in the elderly in a seven-year follow-up study. In a recent study, Orlandoni et al. 13 demonstrated that patients with dementia had better chances of survival than patients without dementia, with no statistical significance though.
We found a high prevalence of cancer (33.6%), mainly head and neck cancer (14.3%). The prevalence of cancer patients on HEN varies in the literature, ranging from 2.7%, as reported by Morelo et al. (3), to 34.1%, found by De Kuis et al. 4. In the study by Santarpia et al. 1, the incidence of cancer increased by 327% in adults and 359% in the elderly during the seven years of follow-up.
In our study, neurological patients had lower survival rates than cancer patients, maybe because of their poorer health status. Although this was a follow-up study, conclusions about the association of survival with nutritional status, complications or adherence to HEN cannot be drawn due to the lack of data. Ginzburg et al. 12, in Israel, reported a decrease in adherence to HEN and an increase in HEN complications and mortality over time.
Mean duration of HEN was 180 days in our study. In the study by Morelo et al. (3), the median duration of HEN was 296-307 days among neurological diseases patients, 258 days in stroke patients, 71 days in head and neck cancer patients and 97 days among patients with abdominal cancer. In a study by De Luis et al. (4) mean time on HEN was 159.9 days; 75 patients died and 691 survived. Age was significantly related to survival (HR 1.03; 95% CI 1.01-1.05, p < 0.05) and 49.4% progressed to oral nutrition by the end of the study.
Because this is one of the first studies in Brazil, especially in the southern region of the country, it would be interesting to perform a nationwide multicenter study. HEN is a rapidly expanding modality of health care, and public policies for such therapy should be implemented and routinely evaluated based on time series analysis. A nationwide multicentric study would also allow to describe the current situation of the Brazilian Unified System in terms of coverage and support for patients on HEN.
HEN aims to improve the quality of life of the patient, in addition to enabling recovery of health. In light of the high hospital system costs, HEN may be not only a cost-effective alternative, but also a way of individualizing and humanizing health care. Besides, HEN requires a closer integration of the multidisciplinary team, especially the dietitian, with the patient and the family. Re-evaluation and improvement of public policies for HEN in developing countries such as Brazil is needed.
In conclusion, our findings show a high frequency of patients on HEN, with a predominance of men, patients with neurological diseases and cancer. Survival rates varied according to the diagnosis, with an association of neurological diseases with poor survival.

