










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The human immunodeficiency virus (HIV) remains one of the most serious global health threats of our time. In the beginning of the 1980s, people living with HIV/AIDS (PLWHA) were given a short life expectancy. However, with the introduction of combined antiretroviral therapy (cART), mortality rates for PLWHA have dramatically decreased (1).
Without question, the introduction of the cART regimen is one of the greatest achievements in public health over the past few decades, and has caused HIV to shift from a death sentence to a chronic infection (2). However, an increase in morbidity and mortality as a result of HIV/AIDS, due to cardiovascular disease, kidney- and liver-related diseases, cognitive decline, and osteoporosis, has been reported (3-5). Additional adverse effects from exposure to cART and HIV infection include metabolic disorders (e.g., dyslipidemia and increases in blood glucose) and morphologic changes (central lipohypertrophy and/or peripheral lipoatrophy). These characteristics are known as the “lipodystrophy syndrome of HIV” (6,7). These changes represent serious problems because lipodystrophy increases the risk of developing cardiovascular diseases, may cause social and psychological distress, and may contribute to discontinuation of HIV treatment (8) among other problems. Thus, earlier identification and adequate treatment for lipodystrophy characteristics may improve the overall health and well-being of PLWHA.
To date there is no methodological consensus for identifying lipodystrophy characteristics. A clinical evaluation is the most widely used method for identifying and diagnosing lipodystrophy characteristics (9). However, this method is subjective and cannot identify body composition changes in the initial stages of lipodystrophy. Also, imaging methods (e.g., magnetic resonance imaging, computed tomography, and dual energy X-ray absorptiometry) have been used to identify and monitor lipodystrophy characteristics (10,11). Although some researchers agree that diagnosing lipodystrophy with imaging methods is accurate, the high operational cost of imaging technologies is an important factor that limits their utilization in clinical settings and in studies with large numbers of participants. This lack of consensus regarding accurate, low-cost methods for identifying lipodystrophy characteristics remains unresolved in the field.
Anthropometric methods such as skinfold thickness and body circumferences are typically used to measure body composition (12,13). These methods are easy to use, present a low operational cost, and have been validated in various populations. However, there is no current literature on the utilization of these methods to identify lipodystrophy characteristics in PLWHA. Thus, our study proposes to fill this gap in the literature by developing a simplified method to identify lipodystrophy characteristics in Brazilians living with HIV/AIDS. In what follows, we propose anthropometric cutoff points for the identification of lipodystrophy characteristics in this population. We believe this information may assist health professionals in accurately identifying lipodystrophy characteristics at a low cost, and thus works towards decreasing the adverse health effects on body composition associated with cART.
MATERIAL AND METHODS
STUDY POPULATION
In this study we adopted a cross-sectional design and evaluated 106 individuals (mean age = 46.2 years). All of them were diagnosed with HIV/AIDS and were on treatment at the University Hospital of Ribeirao Preto School of Medicine, University of Sao Paulo, Brazil (HC-FMRP-USP/UETDI). The study was conducted from November 2013 to November 2014. During the period of the study, 1,298 people living with HIV/AIDS were receiving treatment at the HC-FMRP-USP/UETDI. To achieve a power range of 0.75 to 0.80 with a significance level of p < 0.05 for detecting differences between people living with HIV/AIDS, with and without lipodystrophy, a sample size of 100 to 112 patients was recommended. Accordingly, we reached out to 125 people living with HIV/AIDS at the HC-FMRP-USP/UETDI, and after their meeting inclusion and exclusion criteria we were able to collect complete data from 106 individuals. The inclusion criteria adopted for this study were: participants diagnosed with HIV/AIDS as adults, aged between 18 and 69 years, under cART treatment, with or without physical characteristics of lipodystrophy. Exclusion criteria included: being treated for opportunistic diseases or cancer, immune inflammatory diseases, wasting syndrome, rare metabolic disorders, use of ergogenic products that could cause body composition alterations, being pregnant or breast feeding, using prostheses, amputated, and engaged in an exercise program during the past 6 months or experiencing rapid weight loss over the past 6 months.
Our study was in agreement with the Helsinki declaration. All participants volunteered for the study, were informed about the scope of the study, and provided their written consent. The study was approved by the Ethics Review Board at University Hospital of Ribeirao Preto School of Medicine, University of Sao Paulo, Brazil, process number: 7082/2011.
PROCEDURES
We collected from medical records the following information; age (years), time from HIV diagnosis (years since the diagnosis), and time on cART (years since the beginning of treatment). The self-reported race/ethnicity of the participants in our sample was broadly consistent with those reported nationally by the Brazilian Institute of Geography and Statistics (14).
DIAGNOSIS OF LIPODYSTROPHY
People living with HIV/AIDS were classified as with or without lipodystrophy based on a clinical evaluation of lipodystrophy. In this method of diagnosis, the presence or absence of visceral fat accumulation in the trunk is not considered (9). Rather, the clinical evaluation is made by achieving a consensus about the loss of subcutaneous fat between the evaluator and the participant. A trained evaluator asked the participant whether she/he had experienced a reduction in peripheral subcutaneous fat in areas of the face, buttocks, arms, and legs after receiving a diagnosis of HIV infection and after beginning cART. A lipodystrophy diagnosis was made if the participant stated that she/he had lost fat in at least one of these areas, and if the evaluator, after a visual assessment of the participant, also perceived a reduction of fat in the same areas. However, if the visual assessment of the evaluator did not agree with the report made by the participant, lipodystrophy was not diagnosed (9). This clinical evaluation process is a commonly adopted method in Brazil both in research and clinical practice (10,15 16 17-18).
STUDY GROUPS
In order to propose cutoff points for identifying lipodystrophy characteristics, we studied people living with HIV/AIDS, with and without lipodystrophy. After a clinical evaluation considering only alterations in areas of the face, buttocks, arms, and legs, participants were assigned to either a lipodystrophy (LD) or a non-lipodystrophy (NLD) group. In this study we included 41 women (LD = 12 and NLD = 29) and 65 men (LD = 29 and NLD = 36).
MEASUREMENTS
“Original” measurements
In order to establish anthropometric cutoff points for identifying lipodystrophy characteristics we used anthropometric measurements, referred to in this manuscript as “original.” Skinfold thickness was measured in six regions: triceps, subscapular, suprailiac, abdomen (horizontal), thigh, and medial calf. The Prime caliper (Harpenden Scientific model) was used to measure each participant’s skinfolds. During the assessment of skinfold thickness, the fold is raised perpendicular to the surface of the body at the measurement site. The long axis of the fold is aligned in agreement with the instructions for each skinfold. The basic principle is that the long axis be parallel to the natural cleavage lines of the skin in the region of the measurement. The fold is kept elevated until the measurement has been completed. More details can be found in Harrison et al. (1988) (19), who present guidelines for carrying out these measures.
Body circumferences were measured at nineteen regions: shoulder (largest diameter), breast (fourth sternocostal joint), waist (smallest diameter), abdomen (umbilical scar), hip (largest diameter), right arm extended, right arm contracted, right forearm, right wrist, left arm extended, left arm contracted, left forearm, left wrist, right thigh (proximal), right medial calf (largest diameter), right ankle (smallest circumference from the ankle, nearest to the malleoli), left thigh (proximal), left medial calf (largest diameter), and left ankle (lower circumference from the ankle, nearest to the malleoli). A 2 m Sanny brand metal band with a latex device at the end was used, which was replaced every 20 participants evaluated. The guidelines for carrying out the measurements are those described by Callaway et al. (1988) (20).
Skinfold thickness and body circumference measurements were performed in triplicate, and the median value was recorded. If there was a variation greater than 5% between measures, a new series of measures was carried out.
“Phantom Z-score” values adjusted by the Phantom Strategy
In addition to using the “original” anthropometric measurements to establish anthropometric cutoff points for identifying lipodystrophy characteristics, we assessed body composition differences between the groups through body proportionality. The most commonly used method is the “Phantom Strategy,” an asexual and arbitrary human reference model for body proportionality with specific anthropometric characteristics for both men and women (21). The main application of the Phantom Strategy is quantifying possible differences expressed in body proportionality indicators between anthropometric measurements as assessed in the participant and in a human reference model for body proportionality.
The first step in application of the Phantom strategy is the adjustment of each anthropometric measurement to the corresponding “Phantom size,” and expressing the difference from the Phantom reference value in Z-scores. The adjusted anthropometric measurement, referred to in this manuscript as “Phantom Z-score,” indicates a score value of the difference between an anthropometric measurement and its reference model (21).
DATA QUALITY CONTROL
Data quality control was carried out in three steps. First, all the anthropometric measures listed above were collected by the same evaluator at three sequential measurements, and the median values were used. In addition, the measures were conducted in 6 patients at a time, and were then re-tested an hour later to confirm accuracy. Finally, the technical error of measurement (TEM) was calculated (22). TEM values were assessed for body circumferences (TEM ≤ 0.71 cm) and skinfold thickness (TEM ≤ 0.60 mm), ensuring the reliability of the measurements within established limits (22).
STATISTICS
Prior to conducting a data analysis, we checked the database and cleaned for errors of data entry and impossible/inconsistent values. The Shapiro Wilks test was used to examine the normality of the distribution among continuous variables. Data with normally distributed parameters are presented as mean and standard deviation by sex for all variables, with a 95% confidence interval. Data that displayed a skewed distribution are presented as median and interquartile range (p25 to p75). For comparison of differences in data between the LD and NLD groups we adopted Student’s t-test, and the Mann-Whitney U-test for normal and skewed distributions, respectively. The Cohen’s effect size was assessed to compare the lipodystrophy magnitude for age, time from HIV diagnosis, and time under cART, and for the anthropometric measurements between both groups. The effect size, known as “d,” was used to determine the significance level comparing the groups, ranging from small (0.20 ≤ d < 0.50), to moderate (0.50 ≤ d < 0.80), to large (d ≥ 0.80) (23).
After comparing age, time from HIV diagnosis, time under cART, and the anthropometric measurements between the LD and NLD groups, we selected only anthropometric measurements for calculating the cutoff points due to the purpose of our study. We elected for this study only anthropometric measurements for proposing cutoff points, which were considered statistically significant with p-values of < 0.01 and when the area under the curve (AUC) was greater than 70% following the Receiver Operator Characteristic (ROC) curve analysis. The accuracy requirement adopted in this study is due to the large number of anthropometric measurements assessed, and our goal of identifying any differences between the LD and NLD groups with a high level of accuracy. In addition, cutoff points were established for these anthropometric measurements by using the Youden index (24). The Youden index is a function that includes the sum of the highest values for sensitivity and specificity minus one. The Youden index ranges from 0 (zero) to 1 (one). Values close to 1 indicate a relatively large efficacy, and values close to 0 limited efficacy (24). The software used for data analysis was the SPSS 23.0 package.
RESULTS
Our sample was composed of white Brazilians (n = 67, 63.2%), pardo (brown) Brazilians (n = 20, 18.9%), black Brazilians (n = 10, 9.4%), and Asian Brazilians (n = 9, 8.5%). Table I lists a descriptive analysis by sex, age, time from diagnosis with HIV, and time of exposure to cART. These are important variables to consider because of the accelerated aging process associated with cART and its effects on body composition in people living with HIV/AIDS.
Table I shows a comparison between people clinically diagnosed with and without lipodystrophy (LD vs. NLD groups, respectively). The results show that age was not significantly different between LD and NLD for both men and women, with the majority of participants being in their 40s. Among men, the results showed a significant association of lipodystrophy with time from HIV diagnosis and use of cART. In comparison to those without lipodystrophy, men with lipodystrophy showed (p < 0.001) an average of six more years for their time from diagnosis with HIV (LD = 12.5 vs. NLD = 6.6 years) and use of cART (LD = 11 vs. NLD = 5 years). Even though there was no significant statistical difference between the LD and NLD groups among women, a similar trend between time from HIV diagnosis (LD = 11.3 vs. NLD = 7.6 years) and use of cART (LD = 9.2 vs. NLD = 5.5 years) was observed (p = 0.223 and p = 0.115, respectively).
Table I. Descriptive analysis and differences test for the variables age, time of exposure to HIV and cART, by sex, and lipodystrophy diagnosis in 106 people living with HIV/AIDS
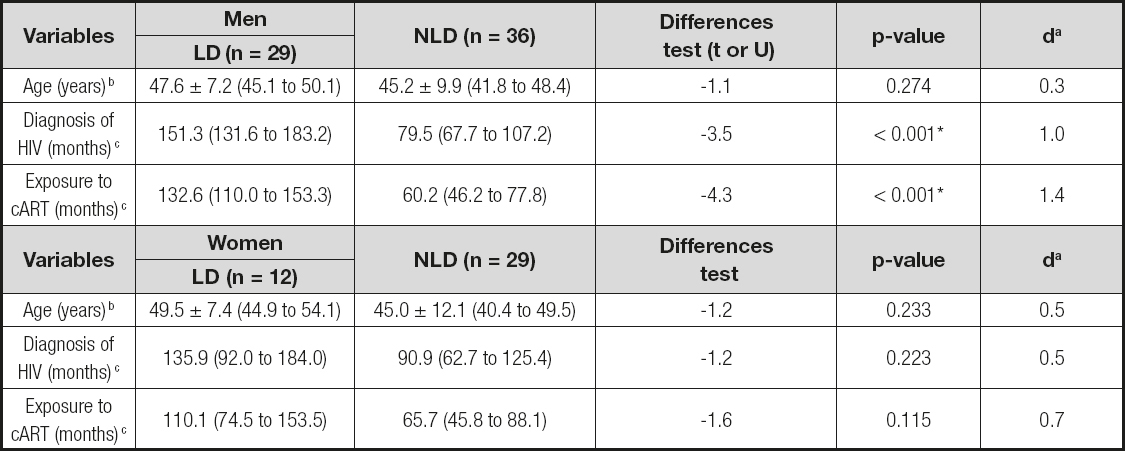
aResults of Cohen effect size test;
bValues expressed as mean ± standard deviation, confidence interval of 95%, and results of differences test by using Student’s t-test;
cValues expressed as median and interquartile range (p25th to p75th), and results of differences test by using Mann Whitney U-test.
*p < 0.01 considered significant based on Mann Whitney U-test.
HIV:Human Immunodeficiency Virus;
cART:Combined AntiRetroviral Therapy;
AIDS:Acquired ImmunoDeficiency Syndrome;
LD:LipoDystrophy group;
NLD:Non- LipoDystrophy group.
Tables II and III show anthropometric differences by sex for those with and without lipodystrophy, with results reported only for variables with p < 0.01 and AUC higher than 70%. Between-group analyses indicate that our proposed cutoff points tend to have greater sensitivity than specificity. This reflects a higher probability of identifying lipodystrophy characteristics using the proposed cutoff points when PLWHA have these anthropometric characteristics. In addition, the effect size for all anthropometric variables was either moderate or large (d ≥ 0.7). This leads us to believe that PLWHA will be accurately identified for lipodystrophy characteristics when their anthropometric measurements are lower than the cutoff points proposed. The further down the anthropometric values go in comparison to the cutoff points, the greater the probability of lipodystrophy. Table II shows a data analysis based on the “original” anthropometric measurements, which includes our proposed cutoff points for identifying lipodystrophy characteristics. Out of the 6 skinfold thickness regions and 19 body circumferences measured, we found significant accuracy (AUC > 70%; p < 0.01) in 3 skinfold thickness measurements for both sexes, and in 7 body circumferences for men and 4 for women.
Table II. Cutoff pointsa using original measurementsto identify lipodystrophy characteristics for 106 people living with HIV/AIDS, by sex

aResults only for variables with p < 0.01 and area under the curve (AUC) higher than 70%;
bResults of Cohen effect size test;
cArea under the curve in percentage value;
dConfidence interval of 95% from the area under the curve;
eValues expressed as mean ± standard deviation, 95% confidence interval, and results of differences test by using Student’s t-test;
fValues expressed as median and interquartile range (p25 to p75), and results of differences test by using Mann Whitney U-test; *p < 0.01 considered significant based on Student’s t-test; †p < 0.01 considered significant based on Mann Whitney U-test.
Abbreviations:HIV: Human Immunodeficiency Virus; AIDS: Acquired ImmunoDeficiency Syndrome; LD: LipoDystrophy group; NLD: Non LipoDystrophy group; cm: centimeters; mm: millimeters.
In men, the optimum (high sensitivity and high specificity) cutoff points for identifying lipodystrophy characteristics were found when skinfold thickness measurements were ≤ 16.3 mm in the suprailiac, ≤ 21.4 mm in horizontal abdomen, and ≤ 9.2 mm in the thigh; and when body circumferences were ≤ 94.7 cm in the hip, ≤ 29.4 cm in the right arm extended, ≤ 16.6 cm in the right wrist, ≤ 29.2 cm in the left arm extended, ≤ 30.4 cm in the left arm contracted, ≤ 16.1 cm in left wrist, and ≤ 50.2 cm in the left thigh. In women, the optimum cutoff points for identifying lipodystrophy characteristics were reached when skinfold thickness measurements were ≤ 17.5 mm in the triceps, ≤ 22.5 mm in the thigh, and ≤ 8.6 mm in the medial calf; and when body circumferences were ≤ 53.6 cm in the right thigh, ≤ 34.1 cm in the right medial calf, ≤ 56.4 cm in the left thigh, and ≤ 32.4 cm in the left medial calf.
Table III shows the data analysis and cutoff points based on anthropometric measurements adjusted by Phantom Z-score values. We found significant accuracy (AUC > 70%; p < 0.01) in 4 skinfold thickness measurements for men and 3 for women, and in 8 body circumferences for men and 5 for women. Table III lists these cutoff point values. In comparison to our proposed cutoff points for lipodystrophy characteristics based on the “original” anthropometric measurements, the adjusted model has an additional body circumference item (Phantom Z-score for the right arm contracted for men, and Phantom Z-score for the right ankle for women), and an additional skinfold thickness score for men (Phantom Z-score for the triceps).
Table III. Cutoff pointsa using Phantom Z-score measurements to identify lipodystrophy characteristics for 106 people living with HIV/AIDS, by sex

aResults only for variables with p < 0.01 and area under the curve (AUC) higher than 70%;
bResults of Cohen effect size test;
cArea under the curve in percentage value;
dConfidence interval of 95% from the area under the curve;
eValues expressed as mean ± standard deviation, 95% confidence interval, and results of differences test by using Student’s t-test. *p < 0.01 considered significant based on Student’s t-test.
HIV:Human Immunodeficiency Virus;
AIDS:Acquired ImmunoDeficiency Syndrome;
LD:LipoDystrophy group;
NLD:Non LipoDystrophy group; cm: centimeters; mm: millimeters.
Our analysis found a similar effect size (d = 1.0 and d = 1.1) and accuracy (AUC% = 76.7% and AUC% = 78%) when using the “original” anthropometric measurements and the Phantom Z-score measurements, respectively. These results indicate that both methods have accurate cutoff points to identify lipodystrophy characteristics in people living with HIV/AIDS.
DISCUSSION
Simplified methods for identifying lipodystrophy characteristics in people living with HIV/AIDS will positively impact public health. With an accessible method, the adverse health effects of infection with HIV and its treatment (cART) can be monitored and treated outside the hospital setting. It will expand the care of people living with HIV/AIDS by multidisciplinary health professionals who work to decrease the comorbidities associated with lipodystrophy. In this manuscript we propose anthropometric cutoff points for identifying lipodystrophy characteristics. So far, to the best of our knowledge, the present study is the first to propose anthropometric cutoff points for identifying and monitoring lipodystrophy characteristics in people living with HIV/AIDS. Our study advances the field by proposing a simplified method that uses anthropometric measurements and that is enhanced by the “Phantom Strategy” of body proportionality.
The length of exposure to cART is an important variable to consider when studying the body composition of people living with HIV/AIDS. Some researchers have published on accelerated lipodystrophy when patients are exposed longer to cART (25,26). Tetteh et al. (2016) (25) followed people living with HIV/AIDS for one year and reported significant changes in metabolic and nutrition disorders, as well as in body composition, due to cART. In our study we confirmed a positive association of exposure to cART and a diagnosis of HIV with the development of lipodystrophy. When compared to men without lipodystrophy, men with lipodystrophy showed an average of six more years since the time of diagnosis of their HIV and their use of cART. Chitu-tisu et al. (2017) (26) compared people living with HIV/AIDS with those without HIV, and concluded that after an average of 5 years since diagnosis and using cART, people living with HIV/AIDS started showing significantly accelerated lipodystrophy. Alves et al. (2016) (27) documented the influence of time of exposure to cART on the diagnosis of HIV in women (27). However, our study could not confirm this association among women. Further research is needed to clarify this association in women. It seems that lipodystrophy affects women more than men based on the higher overall effect size observed in our study.
Our findings indicate that our proposed anthropometric cutoff points are accurate for the identification of lipodystrophy characteristics in people living with HIV/AIDS. Our findings support the use of cutoff points that include 17 and 20 anthropometric measurements for “original anthropometric measurements” and “Phantom Z-score” values, respectively. The cutoff points proposed are especially important during the clinical evaluation of lipodystrophy when the patient and the evaluator are not in agreement, and when the evaluator has doubts about lipodystrophy severity. In the early stages of lipodystrophy cutoff points can serve as valuable tools to help health professionals confirm lipodystrophy characteristics among people living with HIV/AIDS. In addition, cutoff points can also be used to monitor body composition changes by comparing results in subsequent evaluations. Thus, an earlier identification and adequate treatment for lipodystrophy characteristics can prevent or delay the development of cardiovascular diseases, thereby leading to better overall health and well-being for people living with HIV/AIDS (28,29).
Whether to use cutoff points from the “original” measurements or from the Phantom Z-score values remains an open question. However, in practical terms, using the cutoff points based on the “original” measurements is the most simplified way and would require the least amount of time and effort.
Our study had some limitations worth noting. We acknowledge that there are other factors that may influence body composition that were not addressed in this study, including nutritional patterns, socio-economic status, heredity, and previous opportunistic diseases. Also, it is important to note that we did not include in this study HIV/AIDS patients that were in treatment for opportunistic diseases. So, caution is warranted when generalizing our proposed cutoff points for lipodystrophy characteristics to all HIV/AIDS patients. In addition, accelerated aging is commonly experienced by people living with HIV/AIDS. Both aging and HIV status have been shown to influence body composition; however, to date, there are no studies in the literature that explore the nature of the interaction between these two variables.
We did not use body mass index or waist circumference as inclusion criteria in our study. Instead, we chose to utilize clinical evaluation procedures to identify the presence or absence of lipodystrophy. In this approach the presence or absence of visceral fat accumulation in the trunk is not considered. However, when we analyzed the differences in body mass index and waist circumference between lipodystrophy and non-lipodystrophy groups, we found statistical differences at p < 0.01 only for body mass index. We found lower values for body mass index in the lipodystrophy group and no statistical significant difference in value for waist circumference among groups (data not shown). All cutoff points proposed for body circumferences are from upper and lower body segments, and not from the trunk. Thus, our cutoff points may fit better for identifying lipoatrophy characteristics in lipodystrophy.
We did not perform an external sample validation for our anthropometric cutoff points to confirm the accuracy of the cutoff points used to identify lipodystrophy characteristics in people living with HIV/AIDS. However, we decided to select and propose in this manuscript only anthropometric measurements, which after difference tests and ROC curve analyses better distinguish the lipodystrophy and non-lipodystrophy groups at p < 0.01 and AUC > 70%, respectively. The accuracy requirement adopted for selecting the anthropometric variables for proposing cutoff points may minimize the absence of an external sample validation. Our sample has a similar proportion of white, pardo, black, and Asian Brazilians as the national population (14). While there are demographic differences across Brazil’s regions, our study did not address the impact of these differences on the identified cutoff points. To the best of our knowledge there are no anthropometric cutoff points to identify lipodystrophy characteristics in people living with HIV/AIDS from other countries. Accordingly, our study may also have clinical value elsewhere, particularly for individuals from low- and middle-income countries. Future studies should continue investigating body composition alterations in people living with HIV/AIDS and confirm the broad use of our findings.
In summary, the findings presented here support the use of cutoff points that include 17 and 20 anthropometric measurements, namely “original anthropometric measurements” and “Phantom Z-score” values, respectively, as a simplified method for identifying lipodystrophy characteristics in people living with HIV/AIDS in Brazil, with similar race/ethnicity characteristics as in the national population. This information provides an important clinical tool for monitoring adverse health effects among people living with HIV/AIDS, and for the development of future care strategies for implementation by multidisciplinary teams working in this area.

