










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Nowadays, screen time (ST) has become increasingly common worldwide. Excessive screen time has been reported to be associated with poorer health outcomes in children, including an increased risk of obesity, a lower motor and cognitive development, worse psychosocial health (1,2), as well as unhealthy eating patterns (3). Thus, international guidelines advise not to spend more than 2 hours of recreational screen time (4).
In general, the evidence available suggests that sedentary behavior (and especially ST) has a stronger relationship with unhealthy habits (4). A gradient was observed across most health indicators, showing that a less sedentary behavior (particularly ST) was associated with better health indicator profiles; however, higher quality studies are needed to confirm this primarily observational evidence (1).
In addition, it has been suggested that a high quantity of ST hours could displace the time spent in physical activity, resulting in an increase in food intake during ST and/or a reduction in sleep hours (5). Unfortunately, it has recently been reported a general lack of compliance with the international guidelines on ST (4). Likewise, these worrying results have also been found in Spain (6,7), where a limitation of periodic data on sedentary behavior has been pointed out (6).
Regarding healthy eating patterns, the Mediterranean diet (MD) has been identified as one of the healthiest eating patterns in the world (8) due to its particular characteristics, such as a high consumption of vegetables, the use of olive oil, a moderate intake of dairy products, and maintenance of an active lifestyle (9). However, adherence to MD in the Mediterranean region seems to follow a negative trend over the past few years, mainly among children (10). This fact could result in impairment of their global health leading to a greater risk of cardiovascular disease, overweight, obesity, and metabolic syndrome (11).
On the other hand, the relationship between ST and adherence to MD has been analyzed in some previous studies, with most of them showing an inverse association (12,13). Nevertheless, there are no studies analyzing MD patterns according to compliance with ST guidelines in children. In line with this, the combination of higher ST and unhealthy eating habits could represent an additional problem for children’s health, increasing the risk of obesity, among others.
According to the evidence and lack of information about this association, the aim of this research was to explore the relationship between dietary pattern habits and compliance with ST guidelines in schoolchildren aged 6 to 13 years in the Region of Murcia (Spain).
MATERIALS AND METHODS
DESIGN AND PARTICIPANTS
A cross-sectional and associative study was performed in a total of 370 schoolchildren (44.9 % girls) aged 6-13 (8.7 ± 1.8) years, with similar socio-demographic characteristics, from six primary schools in the Region of Murcia (Spain). For this purpose, the sample was selected using a non-probability sampling method. However, although we used this type of sampling, all schoolchildren from the selected schools were invited to participate voluntarily. In order to participate in the study parents/legal guardians had to provide a signed consent form. These parents/legal guardians and their children were previously informed through an informative document about the purpose of the study and the nature of the tests that would be performed. As an exclusion criterion, we did not include those students who were exempt from participation in Physical Education.
This research was conducted in accordance with the Helsinki Declaration and with full respect for the human rights of those concerned.
PROCEDURES
Daily screen time
In order to determine daily ST, participants were asked to report the exact number of hours that they usually spent daily in ST (TV or videogames) by an ad hoc questionnaire. Moreover, two categories of ST were established (< 2 hours = low ST; ≥ 2 hours = high ST), according to the international guidelines for ST in children (4).
Dietary habits
In order to determine the dietary habits, the Mediterranean Diet Quality Index for children and teenagers (KIDMED) was used (14). This is a validated test in children and adolescents that is widely used in Spain (13,15). This index varies from 0 to 12 and is based on a 16-item test. Questions that present negative aspects in relation to MD are scored with a value of -1, and those with positive aspects with +1. The sum of all values from the administered test is categorized into three different levels: 1) > 8, optimal MD; 2) 4-7, improvement needed to adjust intake to Mediterranean patterns; 3) ≤ 3, very low diet quality (14).
Anthropometric measurements
Anthropometric measurements were performed during school hours by trained evaluators that used pre-calibrated steel callipers (Holtain, Crosswell, Crymych, UK). Skinfold measurements were taken at the biceps, triceps, subscapular level, and iliac crest. The log of the sum of skinfolds was used in order to compute body density (16). Likewise, the Siri formula was used to determine body fat (17). The body weight of the participants was determined using an electronic scale (Tanita BC-545, Tokyo, Japan). The height of the participants was determined using a portable height-measuring device (Leicester Tanita HR 001, Tokyo, Japan). Then, the body mass index (BMI) was computed as: [body weight (kg) / height2 (m)]. Waist circumference was measured with a precision of 0.1 cm at the level of the navel using a constant tension tape. All anthropometric measurements were performed according to the recommendations of the International Society for the Advancement of Kinanthropometry (ISAK), considering valid the average of three measurements.
STATISTICAL ANALYSIS
Mean (M) and standard deviation (SD) values are reported for all quantitative variables, and frequencies and percentages (%) are presented for all qualitative variables. Data normality was verified using the Kolmogorov-Smirnov test with Lilliefors’ correction, and homogeneity of variances using Levene’s test. ST and KIDMED scores had skewed distributions and were transformed prior to the analyses. To aid interpretation, a two-step approach was used to transform continuous, non-normally distributed variables into normally distributed variables (18). Subsequently, the data were analyzed using Student’s t-test for two-group comparisons. Effect size was calculated by Cohen’s d (0.20, small; 0.50, medium; and 0.8, large effect) (19). Analyses of covariance (ANCOVA) were used to evaluate differences between mean KIDMED scores across groups of CRF (low and high CRF) and ST (low and high ST). With the sample of 370 children, the posteriori sample calculation indicated a power of analysis (for ANCOVA) of 98 % for correctly rejecting the null hypothesis. We included age and body fat percentage as covariates. Likewise, we established four different groups according to ST and sex in order to show the differences between them. Associations between qualitative variables were determined using Pearson’s chi-squared test. In addition, a multinomial logistic regression was carried out in order to predict the probability of having different dietary patterns depending on compliance with ST guidelines. The data analysis was performed using the software SPSS (IBM Corp, Armonk, NY, USA) for Windows (version 24.0). An alpha (α) value of 0.05 was established for statistical significance.
RESULTS
Data on age, anthropometric characteristics, daily ST, and MD of the sample according to sex are shown in table I. Regarding daily ST, boys scored higher than girls and, conversely, the prevalence of meeting ST guidelines was higher in girls. Nevertheless, no statistical significance was found in both cases. Concerning MD, girls scored greater than boys in KIDMED, as well as in the prevalence of high MD. However, as in the case of ST, no statistically significant differences were found.
Table I. Descriptive data of the sample stratified by sex

Data expressed as means (SD) or frequencies (%). BMI: body mass index; BF: body fat; ST: screen time; WC: waist circumference; WHtR: waistto-height ratio. aFrequency of participants with high adherence to MD. bFrequency of participants who meet screen time guidelines (< 2 hours).
As figure 1 shows, ANCOVA revealed higher KIDMED test scores in those who met the ST guidelines (p < 0.001). According to sex, statistically significant differences were shown between boys and girls in those who do not exceeded the recommended ST (p = 0.045). Regarding compliance with ST guidelines, statistically significant differences were found in girls who met them (p < 0.001).
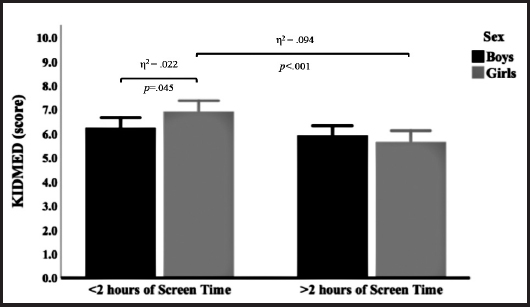
Figure 1. Adherence to the Mediterranean diet in schoolchildren according to the international guidelines on screen time, stratified by sex. Estimated means (bars) and 95 % CIs (error bars) represent values after adjustment for age and body fat percentage.
On the other hand, the prevalence of different MD factors included in the KIDMED questionnaire are presented in table II, according to compliance with ST guidelines and sex. In the case of boys, higher consumptions of vegetables were found in those who met the ST guidelines (p < 0.050), not so in the case of candies, with a higher intake in those who exceeded the ST guidelines (p = 0.048). Concerning girls, a higher intake of fruits, vegetables, nuts, and fish was shown in those who did not surpass ST recommendations (p < 0.050).
Table II. Prevalence of different dietary habits according to the international guidelines on screen time

Data expressed as frequencies (%). MSTG: meeting screen time guidelines; NMSTG: not meeting screen time guidelines. Italics indicates statistical significance (p < 0.050).
Lastly, table III indicates the probability of having different MD patterns according to compliance with ST guidelines. For boys, those who did not meet the guidelines presented lower chances of eating vegetables regularly (OR = 0.50; CI95 % = 0.28-0.89) as well as more than once a day (OR = 0.43; CI95 % = 0.22-0.85). Thus, in girls who did not meet the guidelines a statistically significant lower probability of eating one piece of fruit (OR = 0.43; CI95 % = 0.19-0.99) as well as a second piece (OR = 0.22; CI95 % = 0.22-0.81) was observed. Similarly, an inferior probability was found for taking vegetables more than once a day (OR = 0.39; CI95 % = 0.19-0.80), fish (at least 2-3 times/week) (OR = 0.40; CI95 % = 0.20-0.78) and nuts (at least 2 or 3 times per week) (OR = 0.46; CI95 % = 0.24-0.87) in girls who did not meet the guidelines. Likewise, lower chances of eating sweet or candy daily were found in both sexes, with differences not being statistically significant.
Table III. Binary logistic regression analysis of different dietary habits according to the international guidelines on screen time
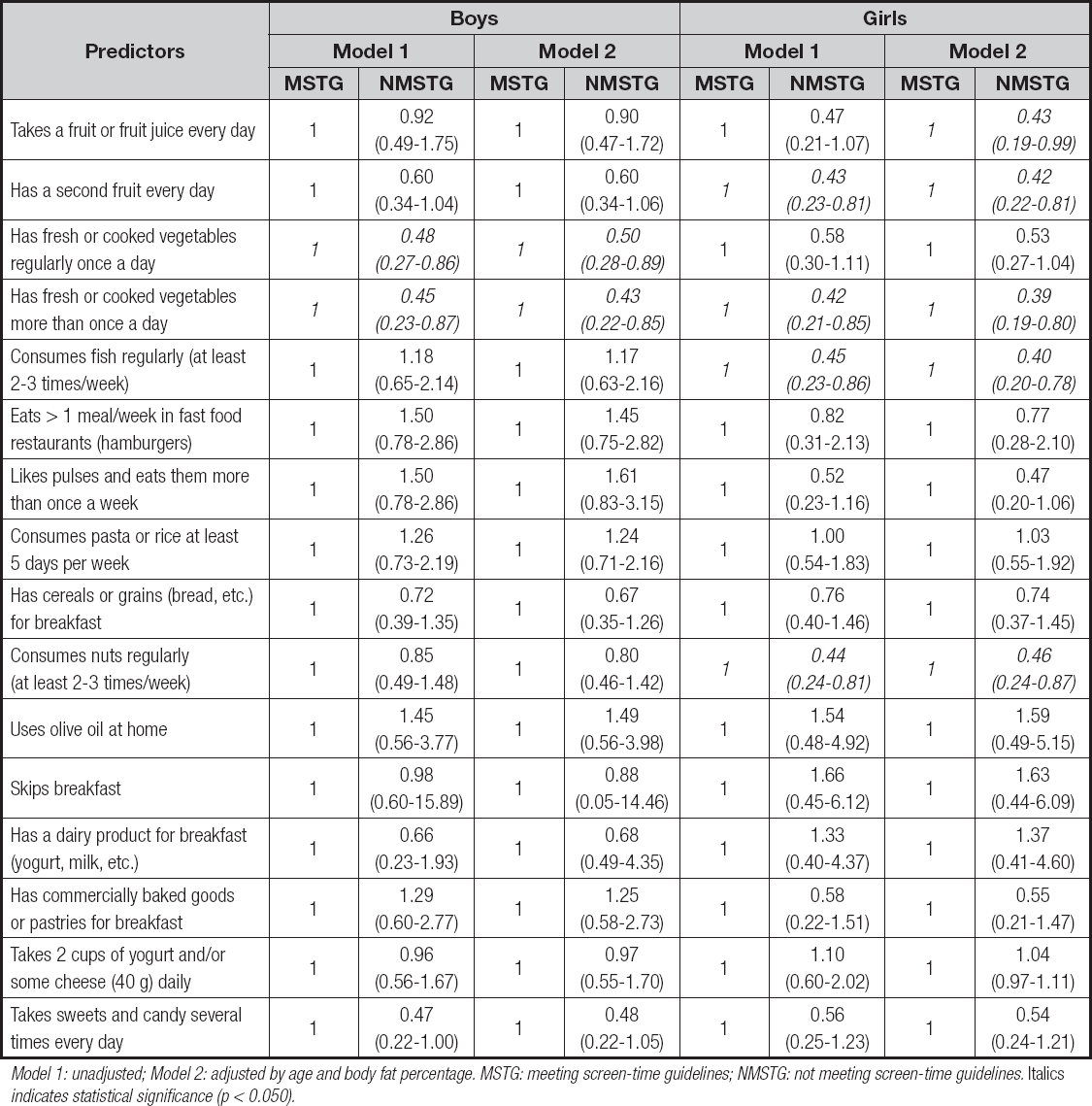
Model 1: unadjusted; Model 2: adjusted by age and body fat percentage. MSTG: meeting screen-time guidelines; NMSTG: not meeting screen-time guidelines. Italics indicates statistical significance (p < 0.050).
DISCUSSION
The aim of this research was to explore the association between dietary pattern habits and the meeting of ST guidelines in schoolchildren aged 6-13 years in the Region of Murcia (Spain). In line with the results obtained, it is advised that no statistically significant differences between sexes were shown according to daily ST and KIDMED score. However, children who met the ST guidelines presented a greater adherence to MD (only statistically significant in girls). Moreover, some healthy dietary patterns were associated with compliance with ST guidelines, such as vegetables (in both sexes) and fruits, fish and nuts (in girls).
Previous studies have pointed out the inverse relationship between ST and adherence to MD in children (13,15). Indeed, among the determinants of the abandonment of the Mediterranean dietary pattern in Spanish youngsters, spending more than 4 hours per day on ST was indicated as the most important factor (20). In the present study, it has been also shown a negative association between ST and adherence to MD (mainly in girls), in line with most of the studies carried out in different countries (12,13,21). At the same time, children who eat healthy meals seem to be more prone to be physically active and less sedentary than those who eat unhealthier meals (22). Nevertheless, it is not clear whether young people who spend more ST completely eat an overall poorer diet (23) or take foods during ST that contribute to a global diet of poorer quality (24).
With regard to healthy dietary patterns, a relationship between more ST and lower-quality diet was shown in our study, especially in girls. Our results agree with those of other authors, which have suggested an inverse relationship between healthy eating patterns and sedentary behavior (commonly measured as ST and mainly TV viewing and computer use) (25). This association is consistent with a systematic review in which television viewing was inversely related to fruit and vegetable intake, and directly related to consumption of energy-dense snacks and drinks, fast foods, total energy intake, and energy from fat in children (3).
In this direction, one study performed in Greece showed that those who did not meet the ST guidelines had greater chances of being frequent sweet consumers, in both sexes (26). At the same time, in line with our findings, a study among Danish schoolchildren revealed that increased TV viewing was linked to unhealthy eating behaviors (27). Likewise, another study among children and adolescents from the United States indicated that higher ST was related to a greater intake of unhealthy foods such as sugar-sweetened beverages, sweets, etc. (28). Moreover, it has been proposed that children exposed to increased TV viewing and advertising time were more susceptible to having unhealthier food patterns (29).
On the other hand, we found higher probabilities of having several healthy dietary patterns in those who met the ST guidelines, especially in the case of girls. Apparently, there are diverse potential reasons linked to this negative association between healthy eating patterns and ST: (i) ST, chiefly television viewing, is contrarily related to foods considered as healthy, like fruits and vegetables, and positively associated to higher intake of energy from high caloric beverages and snacks or junk food (28); (ii) it also appears that watching television and being exposed to food advertisements was positively linked to unhealthy food habits in children and adolescents (29,30). Hence, previous authors differ on how the type of sedentary behavior may have an impact on the consumption of unhealthy food. Therefore, computer usage and television viewing could have different influences; this is due to the fact that using a computer usually involves both hands, thus decreasing the possibility of using them for the consumption of food, which diminishes nutritional risk (31).
These findings would represent relevant implications in order to promote MD as a healthy dietary pattern for health promotion or as a prevention strategy among children. Thus, the need for applying a new concept of MD has been suggested, which emphasizes reducing ST (and sedentary behaviors) and paying adequate attention to eating time, family meals, or socialization with other people, which could help to reduce the negative relationship between MD and excess weight in children (13).
Despite several studies on this topic, to our knowledge this is the first study examining several Mediterranean patterns in relation to compliance with specific international ST guidelines for children. Likewise, another strength of this study is its adding to current knowledge regarding children, a relatively understudied population. Contrariwise, in this research we found some limitations. Firstly, due to the cross-sectional design of the present study it was not possible to conclude that the observed relationships reflect causal relationships. Additionally, self-reported measurements were used to assess ST in this study. Finally, another limitation that we found is related to the lack of information on socioeconomic status, sleeping hours, or individual developmental stage.
When comparing children who met ST guidelines, those who met the international recommendations for ST presented higher levels of adherence to MD. Likewise, some healthy eating patterns seem to be more frequently found among those who meet ST guidelines (especially in girls), such as consumption of fruits and vegetables.
From a health perspective, these results indicate the need to promote policies and interventions aimed at encouraging adherence to an active lifestyle that includes healthy eating habits (e. g., MD) among schoolchildren in order to decrease ST and try to improve their health.

