










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Vitamin B12 is a water-soluble molecule that is essential for the hematological and neurological systems. Vitamin B12 acts as a coenzyme of methyl-malonyl-Co-A mutase, which is involved in myelin synthesis as well as in lipid and carbohydrate metabolism and DNA synthesis (1).
It has been shown that autonomic dysfunction symptoms such as orthostatic hypotension can be observed before neurological and hematological findings. Effects of vitamin B12 defficiency on sympathetic and parasympathetic systems may cause heart rate variability and autonomic dysfunction. Heart rate variability spectral analyses have shown that sympathetic and parasympathetic activities are decreased in patients with B12 deficiency. Moreover, the interaction of vitamin B12 deficiency with the sympathetic system seems to be more profound than that of the parasympathetic system (1-6).
Prolonged QT dispersions, Tp-e intervals and Tp-e/QT ratios, and corrected measurements of these parameters, were found to be associated with ventricular arrhythmias (3,4). However, the association of vitamin B12 deficiency with repolarization disorders and arrhythmogenic susceptibility in adults is unclear. We believe that since vitamin B12 defficiency leads to demyelination and autonomic dysfunction, it may be more closely associated with arrhythmogenic susceptibility and repolarization defects when compared to other vitamin disorders. The aim of our study was to evaluate the relationship between vitamin B12 levels and repolarization parameters in healthy adults.
MATERIALS AND METHODS
STUDY POPULATION AND PROCEDURE
Electronic data of 745 patients who applied to our outpatient clinic with the complaint of atypical chest pain between August 2019 and March 2021 were analyzed retrospectively. Routine biochemistry and hemogram tests as well as mineral, vitamin B12 and hormone levels were evaluated. Echocardiographic and electrocardiographic measurements were analyzed from the electronic data system. Patients with coronary artery disease, structural heart defect, chronic heart failure, permanent pacemaker, atrial fibrillation or chronic arrhythmias were not included in the study. The subjects who use antiarrhythmic and/or any drug that may affect the QT interval, follow a vegetarian diet, have malnutrition, have a history of gastric or bowel resection, have a diagnosis of cobalamin absorption-metabolism-transport disorder and receive ongoing vitamin B12 replacement therapy, and those with missing laboratory tests, ECG and echocardiographic information were also excluded from the study. Finally, 214 healthy individuals over the age of 18 were included in our study. Our study was designed and conducted in accordance with the principles of the Declaration of Helsinki, after approval from the local ethics committee.
BLOOD SAMPLES
A vitamin B12 level below 200 pg/ml is considered deficiency (5,6). There are not enough publications in the literature evaluating the relationship between vitamin B12 level and ECG parameters and determining the cutoff value, and the main purpose of our study was to determine the effects of B12 level rather than B12 deficiency on ECG. For this reason, the 200 pg/ml limit was not accepted as the cut-off value. Instead, 25 % and 75 % percentiles of vitamin B12 levels were accepted as cut-off values, and the study population was divided into 3 groups. Group 1: vitamin B12 level < 253 pg/ml; Group 2: 436 > vitamin B12 level ≥ 253 pg/ml; Group 3: vitamin B12 level ≥ 436 pg/ml.
ELECTROCARDIOGRAPHY
After the patients had rested for 10 minutes in the supine position, ECG recordings were obtained by placing electrodes in standard anatomical points with a speed of 25 mm/s and a width of 10 mm/mV (Cardiofax GEM, model 9022 K, Nihon Kohden, Tokyo, Japan). ECGs were recorded in our local online imaging program in order to improve the accuracy and reliability of our measurements. Callipers and magnifying lenses were used in the evaluation of manual ECG measurements, which was performed by two experienced cardiologists. One of the ECG evaluators was blinded to the demographic data of the patients and had no conflicts of interest, and the other was one of the authors of the study. The interobserver coefficient of variation was 2.12 %. Baseline ECG measurements such as heart rate (HR), PR interval, QRS interval, QT interval were obtained manually, and Bazett's formula (cQT = QT√(R-R interval) was used in the calculation of the QTc interval. The Tpeak-Tend (Tp-e) interval was measured as the interval between the end point of the T wave obtained during the measurement of the QT interval and the projection of the T-wave peak on the isoelectric line (Fig. 1). The average of the values obtained separately from each derivation of the 12-lead ECG was used in the calculation. Dispersion was calculated as the difference between the maximum and minimum PR, QT, QTc, and Tp-e intervals. One measurement was taken from each derivation. However, when the image quality of a derivation was inadequate, at least two consecutive measurements were averaged in order to improve accuracy. ECGs were included in the study data if at least 8 of the 12 leads could be measured.

STATISTICAL ANALYSIS
The analysis was performed with the SPSS 22 (SPSS/IBM, Chicago, IL, USA) software. Continuous and categorical variables were given as mean ± standard deviation and percentages (%), respectively. Normal distribution of continuous variables was evaluated using the Kolmogorov-Smirnov test. The Chi-square test was used for categorical variables. One-way variance analysis or the independent samples t-test was used for the statistical analysis of the clinical data between the three groups. The Pearson's correlation coefficient was used for correlations and the Tukey test was used in the post-hoc analysis. A value of p < 0.05 was considered statistically significant.
RESULTS
A total of 214 subjects were included in the study. Their mean age was 58.09 ± 15.19 years, and 132 (61.68 %) were male. The demographic characteristics and laboratory findings of study participants are presented in table I. Considering the distribution of vitamin B12 levels and accepting 25 % and 75 % percentiles as the cut-off values, the participants were divided into 3 groups. Groups 1, 2 and 3 consisted of 52 (24 %), 108 (50 %) and 54 (25 %) subjects, respectively. There was no significant difference between groups in terms of demographic characteristics and laboratory findings, except for vitamin B12 levels.
Table I. Demographic data and laboratory results of study patients
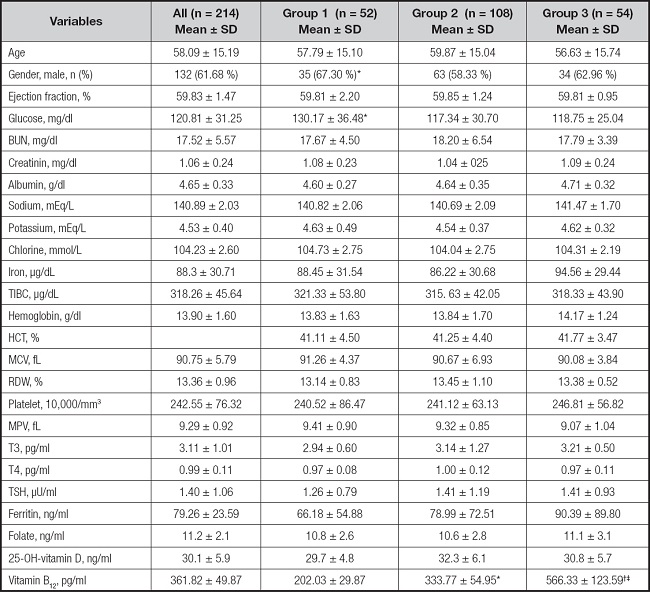
Group 1: vitamin B12 level < 253 pg/ml; Group 2: 436 > vitamin B12 level ≥ 253 pg/ml; Group 3: vitamin B12 level ≥ 436 pg/ml. SD: standard deviation; BUN: blood urea nitrogen; TIBC: total iron-binding capacity; HCT: hematocrit; MCV: mean corpuscular volume; T3: triiodothyronine; T4: thyroxine; TSH: thyroid stimulating hormone.
*Independent sample t-test between group 1 and group 2: p-value < 0.05.
†Independent sample t-test between group 1 and group 3: p-value < 0.05.
‡Independent sample t-test between group 2 and group 3: p-value < 0.05.
The electrocardiographic evaluation is presented in table II. It was observed that the Tp-e interval, Tp-e/QT and Tp-e/QTc ratios were significantly higher in Group 1 as compared to the other groups. An analysis of the dispersion data showed that QTd and QTcd were also significantly higher in Group 1 compared to the other groups. There was not a significant difference in terms of other ECG parameters between groups.
Table II. Electrocardiographic results of study patients

Group 1: vitamin B12 level < 253 pg/ml; Group 2: 436 > vitamin B12 level ≥ 253 pg/ml; Group 3: vitamin B12 level ≥ 436 pg/ml. SD: standard deviation; Tp-e: T-wave peak and end point duration; QTc: QT corrected (by Bazett formula); QTd: QT dispersion (maximum and minimum QT-wave duration difference); QTc d: QTc dispersion (maximum and minimum QTc-wave duration difference).
*Independent sample t-test between group 1 and group 2: p-value < 0.05.
†Independent sample t-test between group 1 and group 3: p-value < 0.05.
‡Independent sample t-test between group 2 and group 3: p-value < 0.05.
The correlation analysis of the ECG parameters that significantly differ between groups and vitamin B12 levels is presented in table III. There was a moderately negative correlation between vitamin B12 level and Tp-e interval as well as QTcd. It was also observed that vitamin B12 level had a weak negative correlation with Tp-ec and Tp-e/QT ratios.
Table III. Correlation analysis results of vitamin B12 levels and electrocardiography findings
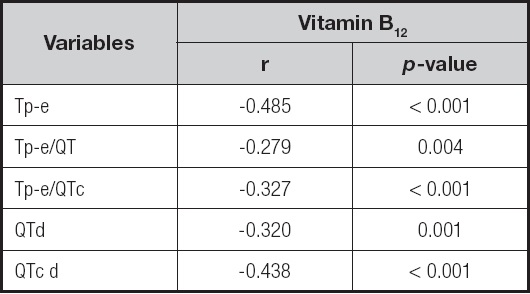
Tp-e: T-wave peak and end point duration; QTc: QT corrected (by Bazett formula); QTd: QT dispersion (maximum and minimum QT-wave duration difference); QTc d: QTc dispersion (maximum and minimum QTc-wave duration difference); Tp-e d: Tp-e dispersion (maximum and minimum Tp-e duration difference).
DISCUSSION
Our study results revealed that Tp-e interval, QT, QTc dispersions and Tp-e/QT, Tp-e/QTc ratios, which are predictors of arrhythmia, were significantly longer in healthy individuals with low vitamin B12 levels. Moreover, a moderate correlation was found between Tp-e and QTcd parameters and vitamin B12 level. To the best of our knowledge, it is the first study to investigate the association between vitamin B12 level and arrhythmogenic potential.
Vitamin B12 is found in animal products and food supplements. The leading causes of low vitamin B12 are insufficient intake of foods containing vitamin B12, cultural reasons, defficiency of intrinsic factor, and decreased intestinal absorption. Vitamin B12 defficiency is most commonly seen in the elderly population and vegetarians (7,8). In our study, the difference in the vitamin B12 levels of healty individuals may have been due to differences in their eating habbits and intestinal absorption.
Vitamin B12 deficiency affects the activity of the sympathetic and parasympathetic systems leading to heart rate variability and cardiac autonomic dysfunction. In addition, it causes endothelial dysfunction and subclinical atherosclerosis via its effects on cellular metabolic pathways that inhibit homocysteine metabolism, lipid peroxidation, and free radical formation (9,10).
The autonomic nervous system is the key regulator of the physiological functions of the cardiovascular system. It is well known that vitamin B12 deficiency causes impaired neuron myelination and thus cardiac autonomic dysfunction (11). In a study, hemodynamic and autonomic responses of patients with B12 deficiency were examined with the tilt-table test, and diminished baroreflex response along with serious decrease in blood pressure was observed in these patients (2). Oner et al. reported that vitamin B12 deficiency may cause sympathetic system baroreceptor dysfunction and postural orthostatic tachycardia syndrome in children (12). In addition, it has been shown in pediatric patients that B12 deficiency causes heart rate variability by affecting the sympathetic and parasympathetic systems. In another study, spectral analyses of heart rate variability showed a decrease in both sympathetic and parasympathetic activity, and the interaction with the sympathetic system was found to be more pronounced (1). Our study results are also consistent with the hypothesis that autonomic nervous system dysregulation and deterioration in metabolic pathways cause changes in cardiac electrical activity.
Vitamin B12 acts in in cellular metabolic pathways that inhibit lipid peroxidation and free radical formation, and hence deficiency of vitamin B12 is associated with endothelial dysfunction and subclinical atherosclerosis (9,13). Çelik et al. reported that their study results on a pediatric group with vitamin B12 deficiency revealed a significant relationship between carotid intimamedia thickness and autonomic modulation of heart rate variability (HRV) (9). Moreover, vitamin B12 deficiency was found to be associated with left ventricular global and segmental myocardial deformation and reduced left ventricular ejection fraction in adults (14,15). It is well known that heart failure and atherosclerosis are predisposing factors for cardiac arrhythmias, especially ventricular tachycardia (16,17). In our study, we ruled out heart failure with echocardiography. Subclinical atherosclerosis may be the reason why the parameters associated with arrhythmia were different in our study population.
Several ECG parameters are accepted to be the indicators of predisposition to arrhythmia (18). Especially ventricular repolarization parameters are thought to play an important role in the formation of ventricular arrhythmias. Heterogeneity of repolarization, which is indicated by increased dispersion of repolarization, is a marker of ventricular arrhythmias. Most commonly used ventricular repolarization parameters are QT/QTc /QTd/QTcd intervals and T wave. Malignant arrhythmias are associated with an increase in the distribution of ventricular repolarization (19). A novel ECG parameter showing ventricular repolarization is the Tp-e interval. Even in patients with normal QTc, the Tp-e interval has been shown to be associated with ventricular arrhythmias and sudden death (20,21). On the other hand, body weight and heart rate are the major confounders for both QT and Tp-e intervals that make these indices less sensitive for predicting arrhythmias. Tp-e/QT ratios has also recently been used as a new electrocardiographic marker for ventricular repolarization (21), and it has been reported to be associated with malignant ventricular arrhythmias (22). Steadiness the of Tp-e/QTc ratio even in the dynamic variations of heart rate makes this parameter more useful compared to a single assessment of either Tp-e or QT intervals (23). In our study, as mentioned above, we examined almost all parameters that are strong indicators of ventricular repolarization and compared them between groups.
In a study by Solak et al, 64 children with B12 deficiency were compared with 64 healthy controls. They found that the QTc, QTcd, Tp-e, Tp-e/QTc and Tp-e /QTcd were longer in the patient group (24). In our study, repolarization parameters were also found to be prolonged in line with the study of Solak et al. The similarity of the results may be due to recruiment of healty individuals in both studies. Enrolment of subjects older than 18 years old and categorization of the study population considering vitamin B12 percentiles were the different points in our study. The stronger negative correlation between vitamin B12 levels and repolarization parameters in their study may be secondary to these methodological differences.
Ventricular arrhythmias are the most common cause of sudden cardiac death in healthy individuals. Especially Qt and Tp-e are the most recent ECG parameters that are thought to be associated with ventricular arrhythmias. Although the most common causes of ventricular arrhythmias are ischemia and heart failure, the etiopathogenesis of many sudden cardiac deaths still remains unclear (25,26). Considering that low vitamin B12 level is associated with autonomic dysfunction, subclinical atherosclerosis, heart rate variability, and myocardial deformation, it may also be associated with some of these unclarified ventricular arrhythmias.
STUDY LIMITATIONS
Our study has some limitations. The first is the limited number of the study population. Since the design of our study was retrospective, subsequent ECGs and long-term arrhythmic outcomes of the participants could not be evaluated. We could not present any information on whether vitamin B12 replacement or dietary recommendations whould have any impact on repolarization parameters. Further studies with appropriate designs are needed in this regard. On the other hand, our study provides valuable information about the effects of low vitamin B12 levels on arrhythmic parameters in asymptomatic healthy adults, and will pave the way for other studies on this topic.

