










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
According to the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, American Psychiatric Association), binge eating disorder (BED) is characterized by eating much more than what most people would eat under similar circumstances over a relatively short period of time. Eating alone and loss of control over quantity and quality of food intake often happens in people with BED (1). Overeating appears despite the lack of physical sensation of hunger. BED episodes occur on average once a week for three months (2). The degree of the disorder is estimated depending on the number of episodes per week, namely: mild (1-3 episodes), moderate (4-7 episodes), severe (8-13 episodes), or extreme (> 14 episodes) (1).
In the development of BED biological, behavioral, psychosocial, environmental and family factors are involved (2). Among the biological factors affecting the development of BED stands out genetics. It has been proven that parents affected by obsessive-compulsive disorder introduce children to dietary restrictions to control their body weight, which affects the occurrence of BED in children (3). Also, reward system dysfunctions are an important trigger of BED. A group of neurotransmitters, which include serotonin and dopamine, stimulate the reward system. Disorders of the system can cause loss of self-control over eating, which leads to episodes of BED arising from the feeling of pleasure after a meal. In addition, neurotransmitters regulating food intake play an important role in the formation of compulsive overeating (4). In the case of impaired leptin release, an increased feeling of pleasure during a meal results in excessive consumption (5). It is also proven that the reduced consumption of energy over a longer period of time correlates with increased food intake during the stressful situation (6).
The effect of slimming diet on compulsive overeating is also undeniable. People using slimming diets are often characterized by dichotomous thinking. Initially they very strictly limit the intake of calories, which consequently leads to 'disinhibition' when they consume an excessive amount of food to compensate for previous dietary restrictions (7).
After an episode of overeating, a short sense of relief and accomplishment happens. At a later stage, remorse leads again to stringent restrictions on food. Thus forms a vicious circle of weight loss, where the person alternately uses strict diet and binge eating.
Personality factors may be determinants of compulsive overeating. Low self-esteem, lack of self-efficacy, the inability to cope with negative situations, anxiety or depression are significant causes of BED (2,8).
Stress is the body's non-specific response to factors adversely affecting the human body. The occurrence of stressors has a significant effect on food intake. According to Groesz stress exposure may lead to a stronger drive to eat and may be the factor that promotes excessive weight gain (9). Stress has also a negative impact on food choices. Consumption of high-fat snacks and fast food is positively associated with higher perceived stress. Ulrich-Lai and colleagues turned their attention to the consumption of food rich in fats and sugar among stress-eating people. The authors emphasize that a diet rich in highly processed foods correlates with increased risk of obesity and diet-related diseases, as well as an increased risk of depression by 55 % (10).
The inability to deal with difficult situations or the process of weight reduction may correlate with an increased risk of episodes of BED. In many cases, consuming food is escape from negative emotions or unpleasant situations.
This 'escape' evokes positive emotions, ie.: the feeling of safety or emotional bond with parents hence effectively relieves tension.
Since the problems of a dietary patient are often a consequence of stress, it seems that in the work of a dietician it is important to use tools that allow its evaluation. The Perceived Stress Scale was used in cross-sectional studies concerned with the eating behavior of Finns (11,12). To our knowledge there are not any papers using the Perceived Stress Scale among people with BED in nutrition counseling to assess the degree to which a patient perceives life as stressful. Thus, this study was focused on an analysis of BED cases in a dietician practice in relation to level of stress. Improved understanding on eating behavior and perceived stress might help to develop dietary counseling methods and improve their effectiveness among dietician patients.
The aim of the study was to check the stress level of patients attending diet consultations, and to find out the relationship between stress and the number of episodes of compulsive overeating. Moreover, according to the nutritional diary and the author's survey, respondent preferences regarding snacks during BED episodes and ways of coping with stress were also studied.
MATERIALS AND METHODS
PARTICIPANTS
One hundred people (60 women and 40 men) were taking part in the study. All the people were attending nutrition counseling in one nutrition company in Silesian Voivodeship in Poland, mainly for weight reduction (46 %) and diet consultation (35 %).
Men, more often than women (57.5 % and 38.3 %), aimed at losing weight, but this difference was proved to be nonstatistical (p = 0.167). Mean age of the study group was 39 (SD = 14.3) years. In a majority of respondents, BMI exceeded 25 kg/m2 — 85 % men and 28 % women were obese. Only 14 % of patients were underweight. A statistical correlation between gender of respondents, and their body weight was observed (p ≤ 0.000). The characteristics of patients are shown in table I.

METHODS
The study was conducted from March 2019 to January 2020. An anonymous author's questionnaire divided into three parts was used in the study. In the first part questions concerning sex, age (years), height (cm), weight (in kg) and slimming diet were included. The second part of the questionnaire included questions concerning the number of meals and snacks, feelings of hunger, the kind of snacks selected during an attack of hunger or overeating, and an assessment of satisfaction with their figure and methods taken to improve it. The third part concerned the ways of coping with stress. Respondents were also asked whether stress and mood affect the consumption of certain products.
The original intention for data collection was not research. Data were collected and stored in a dietary clinic and were used only by a trained dietitian during diet counseling. However, on the first page of the questionnaire was an informed consent and information that a secondary data analysis was planned. Only respondents who read the consent and signed it were included in the data analysis. The secondary analysis of the data was performed anonymously.
The frequency of compulsive overeating was measured by means of a nutritional diary kept by the patient, in which he wrote down everything that was eaten together with the accompanying emotions and situations. At the first visit a professional dietician instructed the patient on how to fill in the diary. The degree of the disorder was estimated depending on the number of episodes per week, namely: mild (1-3 episodes), moderate (4-7 episodes), severe (8-13 episodes), and extreme (> 14 episodes).
The Perceived Stress Scale (PSS-10) was used to measure the degree to which a person perceives life as stressful. The PSS-10 questionnaire consists of 10 questions concerning subjective feelings associated with the behavior, problems, events, and personal ways of coping with them in the last month. The possible answers were scored from 0 to 4, where “0” means never, and “4” very often. The total number of points is the overall result of the test. The higher the score, the higher the severity of stress. The results were interpreted in a standard ten scale (Sten score) based on standards set for the entire study population. This allowed a division of patients into 3 groups, characterised by low, medium and high level of perceived stress.
STATISTICAL ANALYSIS
The analysis was performed with the use of Statistica 13.1 (StatSoft, Poland) and Microsoft Excel. The normality of the distributions of quantitative variables was tested using the Shapiro-Wilk test. Student's t-test for independent samples was performed to compare two groups with normal distribution. Otherwise, the non-parametric Mann-Whitney U-test was used. The Kruskal-Wallis test (ANOVA) was used for comparing two or more independent samples. The relationship between two variables was verified by Pearson's chi-squared test. The level of significance was set at p = 0.05.
RESULTS
Compulsive overeating was measured by the number of episodes occurring in a week. In this study 52 respondents had mild BED manifested with a maximum of 3 episodes; 46 respondents had moderate BED, and severe BED (8-13 events per week) was diagnosed in 2 respondents. There was nobody with extreme BED. Moderate episodes of compulsive overeating were more common among men than women (55 % vs. 40 %); however, this difference was not confirmed statistically (p = 0.299) (Table II).

The number of overeating episodes depended on BMI. People with overweight and obesity more often had moderate BED. The number of episodes per week was smaller among patients with normal weight or underweight (p = 0.004) (Fig. 1).

During BED episodes the respondents most often chose sweets as snacks (58.2 %). Only 13 patients attending dietary consultations ate fruit during a BED episode. Salty snacks were chosen by 5.1 % of women and 10.7 % of men.
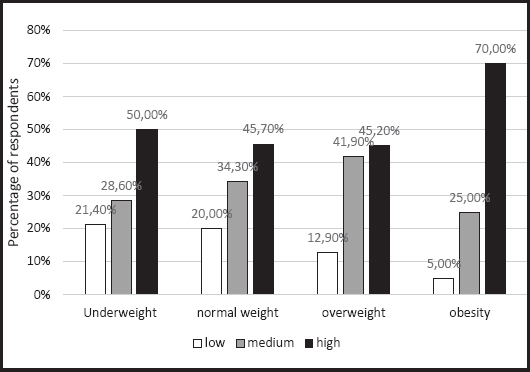
The PSS-10 scale was used to evaluate the stress experienced by respondents. The mean value was 6.65 and more than half of the surveyed subjects (51 %) were characterized by high intensity of stress. Only 15 % of respondents were characterized by low levels of stress. There was no statistically significant difference between the level of stress presented on the Sten scale in a group of men and women (p = 0.863). However, in the study a statistically significant relationship was observed between stress and BMI (p = 0.046). It has been shown that people with normal weight and underweight were characterized by lower levels of stress when compared to those with overweight or obesity. In all, 70 % of obese people were characterized by a high level of stress according to the PSS-10 (Fig. 2).
A statistically significant (p = 0.003) correlation was also observed between level of stress and frequency of BED episodes. Among people experiencing 4-7 BED episodes per week more than two-thirds (67.4 %) declared a high level of stress (Fig. 3).

In the present study, the relationship between stress levels and the strategy for dealing with it was also examined. The results indicated that people with high levels of stress ate more often than less stressed individuals (51 % vs. 6.7 %, p = 0.005). Moreover, high levels of stress most often were associated with snacking, especially sweets (p = 0.005). One third of people attending diet consultations reacted to stress with snacking, 19 % of people with walking, and 16 % with cigarette smoking. Men more often than women coped with everyday stress with snacking (42.5 % vs. 25 %, p = 0.196). Only 16.7 % of women and 10 % of men in case of stress decides to train in the gym.
It is also worth mentioning that 62 people admitted that they did not like their body image. Dissatisfaction with the body appearance correlated positively with level of stress and severity of BED (Table III).

A statistically significant (p = 0.008) relationship was observed between level of stress according to the Sten scale and satisfaction with body figure. Among people dissatisfied with their body image, more than half (58.1 %) showed a high level of perceived stress.
DISCUSSION
A professional dietician has to cope with many tasks in his work. He has to assess his patients' nutritional and health needs, counsel patients on healthy eating habits, and develop meal and nutrition plans. From our perspective a dietician may also deal with patients who require psychological education due to stress. That is why he or she needs a tool to measure it. According to Yeo Do Lee, the currently available tools used in diet counseling include simple questionnaires to diagnose the risk of nutritional deficiency and simple evaluation sheets concerning overweight status and dietary life patterns (13). Among patients with BED these nutritional tools might not be sufficient.
The relationship between stress, BED and BMI is quite obvious. Carson et al. concluded that women who reported higher levels of stress had higher BMI (14). Klatzkin et al. reported that obese BED women had higher dietary restraints and perceived stress than those in the normal-weight, non-BED group (15). However, the study group was quite small and only 9 women had BED. To the best of our knowledge, this was the first study dealing with a relationship between BED, stress, and BMI among patients in nutrition counseling.
In this study most of the respondents had 1-3 episodes a week. Pacanowski and co-workers was looking for the relationship between the problem of binge eating and maintaining the effects of weight loss treatment. They indicated that almost 20 % of respondents from a group of 391 people had BED; however, severity was mostly low. There was nobody with extreme episodes of compulsive overeating (16). Similarly in our study, there was also nobody with extreme episodes of BED and only 2 with heavy BED.
Burrows et al. confirmed statistically that the severity of BED was determined by sex and BMI. It has been observed that obese people had more often moderate BED than people with normal body weight (17). In our study, similar conclusions were formulated. Among obese people, moderate BED occurred more frequently than in the group of respondents with normal body weight.
Stress has a significant effect on food intake. On the one hand, stressful situations make more than 35-60 % of people consume more calories than necessary, while 25-40 % of people consume a reduced number of products (10). In the present study, most people attending diet consultations reacted to stress with snacking, mainly sweets. It should be emphasized that the study group consisted of patients of a diet clinic who should be aware of the negative consequences of snacking. Only 16.7 % of women and 10 % of men in case of stress decide to train in the gym. Only 13 people ate fruit during a BED episode. In another work, even 86.1 % of patients with high levels of stress were snacking sweets (18). According to Babicz-Zieliǹska et al., 82 % of people consumed meals under stress, despite a lack of the physical sensation of hunger. During stressful situations, respondents mostly consumed sweets (19).
The influence of stress on food consumption was also described in another paper. According to it, a group of obese or overweight Finns with high levels of stress were characterized by uncontrolled consumption of food in comparison to people with low levels of stress (11). Perceived stress was also measured with the use of the PSS-10 questionnaire. The ave-rage stress level of respondents was 26.5. In another paper of Elina Järvelä-Reijonen et al. (12), higher perceived stress was not associated with unfavorable features of eating behaviour In our study, the mean value of stress was slightly lower and amounted to 20.32 for the entire study population. It is hypothesized that this results from a different perception of stressors and accompanying emotions by individuals with BED compared to their healthy peers. Individuals with BED reported experiencing more negative stressors in the course of daily life and were less able to tolerate a negative mood, when compared to healthy controls. In addition, daily hassles were experienced as more stressful by individuals with BED than by a control group with a similar number of reported daily problems (20).
Dissatisfaction with the body image was correlated with level of stress and BED severity. All relationships presented in the work underline the importance of psychodietetics in practice. Many authors emphasize psychological support as a first-line treatment in all eating disorders, including BED (21,22). We do not know how much psychological support is needed in the case of BED patients. We suggest that one of the measures to reduce binge eating and improve the mental state of patients may be achieved through participation in a dietician-administered, cognitive-behavioral therapy. Moreover, the use of the stress assessment questionnaire during dietician practice will help to assess stress and show the best ways to cope with it. Knowing how to deal with stress is necessary not only to stay healthy, but also to keep a slim figure.
LIMITATIONS
Our findings should be interpreted in the context of the study's design and limitations. During the interpretation of the results of the study, the limited number of participants should be taken into account. All relationships demonstrated in the work were concerning patients of a diet clinic. It is probable that some variables especially stress level, could be different in other study groups. There are also potential biases resulting from the fact that our study was based on a self-administered questionnaire and nutritional diary. The nutritional diary was filled in by the patients themselves. Despite training by a dietician, it could well happen that an episode or snack was not recorded by the patient.
Lastly, it should be said that it is not possible to draw any conclusions about the cause and effect of the found relationship because of the cross-sectional nature of the study. However, the relation between BED and different adverse health consequences has been proven in other studies.
CONCLUSION
In the present study it was confirmed that stress significantly affects BED. Subjects were characterized by high levels of stress and snacking was the way of releasing tension. In particular, the majority of respondents during an episode of BED ate sweets. People with high levels of stress were characterized by excessive body weight, and they more often experienced episodes of binge eating compared to people with normal weight.
The severity of BED correlates with the stress levels obtained with the use of the standardized PSS-10 scale. It could be of great importance in a dietician's practice. The PSS-10 (Perceived Stress Scale) may be applied as a tool for the diagnosis of obese patients who may potentially experience BED episodes in order to prevent the development of this disorder. Complex training including proper eating habits and psychological consultations aimed at coping with stress levels will be more effective in the fight against obesity and eating disorders.

