










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAnales de Psicología
versión On-line ISSN 1695-2294versión impresa ISSN 0212-9728
Anal. Psicol. vol.29 no.1 Murcia ene. 2013
https://dx.doi.org/10.6018/analesps.29.1.132301
Development of a new instrument to assess AIDS-related attitudes among Spanish Youngsters
Desarrollo de un nuevo instrumento para evaluar las actitudes hacia el VIH/SIDA en adolescentes españoles
José P. Espada1, Rafael Ballester2, Tania B. Huedo-Medina3, Roberto Secades-Villa4, Mireia Orgilés1 y Manuela Martínez-Lorca5
1Universidad Miguel Hernández, Spain
2Universitat Jaume I, Spain
3University of Connecticut, USA
4Universidad de Oviedo, Spain
5Universidad de Castilla-La Mancha, Spain
This research was supported by the Foundation for AIDS Research and Prevention in Spain (Ref. FIPSE 360971/10).
ABSTRACT
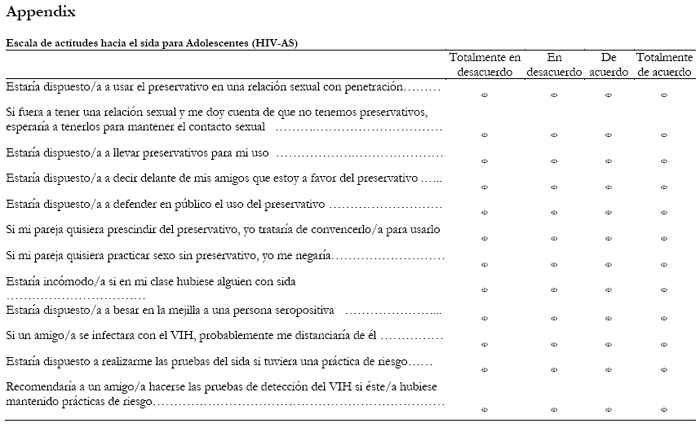
This paper aims to describe the psychometric properties of a new brief multidimensional scale to measure HIV/AIDS related attitudes for adolescents, the HIV Attitudes Scale (HIV-AS). Exploratory analysis aimed to find the theory-driven structure and to develop an empirically derived factor structure for HIV-AS, which was tested with a confirmatory factor analysis. Factorial invariance was studied across gender and age, and multigroup structural equation approach was used in order to compare the groups. Reliability, convergent and discnmmant validity were examined. The analyses were based on a sample of 1216 Spanish adolescents. The instrument consists of 12 items distributed across four major factors: 1) Attitudes towards safe sex when there are obstacles, 2) Attitudes towards the HIV test, 3) Attitudes towards condom use, and 4) Attitudes towards people living with the AIDS. The HIV-AS shows good validity and internal reliability and equivalent four-factor structure across gender and the three age groups studied. It can be consider as a capable and parsimonious self-report scale for assessing major aspects of HIV/AIDS-related attitudes for adolescents.
Key words: HIV/AIDS; attitudes; rating scale; psychometric properties; adolescence.
RESUMEN
El objetivo de este estudio es describir las propiedades psicométricas de una nueva escala multidimensional para evaluar las actitudes sobre el VIH/SIDA en adolescentes, la Escala de Actitudes hacia el VIH/SIDA (HIV-AS). Se realizó un análisis factorial exploratorio con el fin de obtener la estructura factorial del instrumento, que fue puesta a prueba con un análisis factorial confirmatorio. Se analizó la invarianza factorial en función del sexo y la edad mediante ecuaciones estructurales multigrupo. Se examinó la fiabilidad, validez convergente y discriminante. Los análisis se realizaron con una muestra formada por 1216 adolescentes españoles. El cuestionario quedó compuesto por 12 ítems distribuidos en cuatro factores: 1) Actitud hacia las conductas de protección cuando existen obstáculos, 2) Actitud hacia la prueba de detección del VIH, 3) Actitud hacia el uso de preservativo, y 4) Actitud hacia las personas con VIH/SIDA. El cuestionario HIV-AS muestra una alta validez y fiabilidad, y una estructura de cuatro factores equivalente en los tres grupos de edad analizados. Se considera que la escala puede ser empleada de forma parsimoniosa para evaluar aspectos relevantes de las actitudes hacia el VIH/SIDA en adolescentes.
Palabras clave: VIH/SIDA; actitudes; cuestionarios; propiedades psicométricas; adolescencia.
Introduction
HIV/AIDS represents a major social and health problem worldwide, with 33 million people infected in the world and 79,369 in Spain at the end of 2009 (UNAIDS, 2010). Although rates have declined in recent years, new infections are rising dramatically in adolescents and young adults, with 45% of cases occurring in the age range between 15 and 29. Adolescence is characterized as a stage of life with heightened vulnerability for sexual risk behaviors associated to not consistent use of condom, as early sexual debut or substance use (Piña, Lozano, Vázquez, & Carrillo, 2010).
Theoretical models explaining sexual risk behaviors take attitudes into account as a relevant variable in the implementation of healthy behaviors. The theory of reasoned action (Ajzen & Fishbein, 1980) evaluates the role of attitudes, beliefs and subjective norms on behavioral intention, so that an individual perform a behavior when evaluating it as positive and believes that others, usually people and socially relevant groups, considered to be performed. Attitudes assumed by adolescents regarding their sexuality or to individuals diagnosed may be influenced by myths, social transmitted beliefs about HIV/AIDS (Vega & Lacoste, 1995) or the risk perception of sexual transmission (Lameiras, Rodríguez & Lafonte, 2002). Among Spanish students, Uribe, Valderrama, Sanabria, et al. (2009) found positive and neutral attitudes towards people diagnosed with HIV/AIDS, considering that they can live and develop normally within a society, which shows at least a good rejection and acceptance towards people diagnosed with the disease. Regarding to the attitudes and the use of protective methods, it appears that they may be mediated by gender. Muñoz-Silva, Sánchez-García, Martins, & Nunes (2009) found that girls had more favorable attitudes towards condom use, perceiving more benefits than costs compared with their male peers. However, this fact does not imply a higher frequency of condom use during sexual intercourse.
There is a lack of studies using reliable and valid instruments to assess the attitudes related to HIV and sexual risk behaviors among adolescents. This is a major need to be covered in order to better know the dimensions of adolescents' attitudes in this area, and to be able to conduct accurate assessment of risk factors and evaluate preventive programs. Both correlational studies and program evaluations often use non-standardized scales to measure attitudes. A frequent strategy is to develop ad hoc questionnaires where HIV/AIDS-related attitudes are measured using rating scales, so that high scores indicate positive attitudes toward the behavior. In other studies researchers develop and validate instruments to measure factors related to HIV/AIDS. Thus, Boileau, Rashed, Sylla, & Zunzunegui (2008) developed an instrument to measure many constructs factors related to HIV/AIDS, among which include attitudes toward condom use, to sexual experiences and to transactional sex. Other studies translate and adapt scales developed with foreign population, although this is an alternative with some limitations due to cultural differences (Zometa, Dedrick, Know, Westhoff, Siman, & Debaldo, 2007). Examples of adapted versions are the HIV/AIDS-65 Scale (Paniagua et al., 1997) adapted by Bermúdez, Buela-Casal & Uribe (2005) for Colombian population, and the longest version of the same scale, HIV/AIDS-164 Scale (Paniagua et al., 1994) adapted by Bermúdez, Buela-Casal & Sánchez (2003) for Spanish population. In both cases the questionnaire evaluated the knowledge about prevention and ways of transmission of HIV/AIDS, positive and negative attitudes, perceptions of susceptibility to the disease and efficacy toward condom use.
Although there are validated instruments measuring attitudes towards HIV/AIDS, there exist some limitations in their characteristics and applications. Any scale is specially designed for teenagers and some are designed for specific social or cultural group (Boileau et al., 2008). In other cases they assess only attitudes, but included in other variables the same scale as the knowledge, behavioral skills, self-efficacy, communication with parents and peers, subjective norms, intention to use condoms, patterns of contraceptive use, etc. (Boileau et al., 2008; Ito, Kalyanaraman, Ford, Brown, & Miller, 2008; Muñoz-Silva, Sánchez-García, Martins, et al., 2009). Other instruments include a large number of items (Boileau et al., 2008; Givaudan, Leenen, Van de Vijver, Poortinga, & Pick (2008), and above all, very few assessment tools have sufficient psychometric guarantees.
From our knowledge, there are no measures that accomplish the following desirable characteristics: to be developed and validated with Spanish population, assessing exclusively attitudes towards HIV/AIDS, and specifically created and validated for adolescents. The review of the literature suggests that there are few studies providing instruments with sufficient psychometric guarantees to assess the attitudes among the Spanish population. The aim of this paper is to present the development of a new instrument to assess attitudes towards HIV/AIDS among Spanish adolescents, the HIV Attitudes Scale (HIV-AS), and its psychometric properties.
Method
Participants
The incidental sample consisted of 1216 high school students in five provinces in Spain: Alicante (n = 269, 22.1%), Castellon (n = 193, 15.9%), Madrid (n = 258, 21.2%), Oviedo (n = 223, 18.3%) and Murcia (n = 273, 22.5%). Six hundred and three (49.6%) were students of 10th grade, and 613 (50.4%) of 11th grade. Five hundred and twenty four were boys (43.1%) with a mean age of 15.87 (SD = 0.80) and 692 were girls (56.9%) with a mean age of 15.81 (SD = 0.76), divided into 445 adolescents of 15 or younger, 549 of 16 and 222 of 17 or older.
Measures
To design the questionnaire a preliminary version was developed based on the items related to attitudes about AIDS in adolescents proposed by a group of experts. The bank was composed of 32 items that were judged according to their relevance to understand adolescents' attitudes in a given particular topic.
Two self-report measures were used to find the concurrent validity of HIV-AS. The Multicomponent AIDS Phobia Scale (MAPS, Harrell & Wright, 1998), which comprises 20 items rated on a 6-point scale (from 0 "strongly disagree" to 5 "strongly agree"). It has a factorial structure of two components, fear of infection, which includes hypochondriac responses and excessive worry about the disease (α = .73) and fear of others / avoidance, including avoidance behavior and escape from AIDS-related stimuli (α = .77). The test-retest reliability after one week was .64 (Harrel & Wright, 1998).
A brief ad hoc questionnaire assessing risk behaviors composed by dichotomous and rating scale questions was also administered. For this study a rating scale assessing the frequency of condom use during the sexual intercourse from 0% to 100% was used to calculate the concurrent validity between HIV-AS scores and self-reported behaviors.
The score on the Self-Description Questionnaire II (SDQ-II, Marsh, Relich & Smith, 1983; Marsh, 1989) was used to calculate discriminant validity. It is a self-report made up of 76 items with a 5-point scale response format. The scale includes eleven factors, plus a general rate, which consist of different domains of self: self-education, appearance, physical activity, mathematical, relationship with parents, relationships, peer group, honesty, verbal, emotional stability and general self. The authors report adequate internal consistency of the instrument, α = .80 (Marsh, Ellis, Parada, Richards, & Heubeck, 2005).
Data Analysis
A principal component analysis was performed (oblique rotation with delta = -0.2) (Jennrich & Sampson, 1966), correlation analysis using the statistical program SPSS for Windows (version 15.0). Correlational intergroup analysis controlling Type I error rate was carried out with the Bonferroni procedure assuming two-tailed α. Confirmatory factor analysis using AMOS (version 7.0) was used for assessing the equivalence of the factor solution of the four HIV-AS factors and factorial invariance analysis to verify the factorial structure by age and gender (Abalo, Lévy, Rial et al., 2006) using the two types of basic empirical evidence: measurement invariance and structural invariance (Byrne, Shavelson, & Muthén, 1989; Vandenberg & Lance, 2000). Cronbach reliability coefficient to determine the internal consistency of the scale was obtained. The validity (concurrent and divergent) and test-retest reliability were assessed and Pearson correlation reported.
Procedure
After the approval of an ethics committee in experimental research and once received the permissions by the parents, a group of 5 experts generated a set of items to assess various fields related to adolescents' attitudes toward HIV/AIDS. Only those which were rated with score equal or greater than 4 (score 4-5 in a 5-point range) were included. Therefore, the pilot version was composed by 26 items. We conducted a pilot application of the scale with a group of 25 students in order to verify the correct understanding of the items. After confirming that the wording was appropriate, 14 schools in different areas of Spain were randomly selected to participate in the study. The questionnaires were administered in the classroom and conducted by trained psychologists. The questionnaires were answered anonymously with a code only known by the students. After filling were delivered within a sealed envelope to preserve confidentiality.
Results
Exploratory Factor Analysis
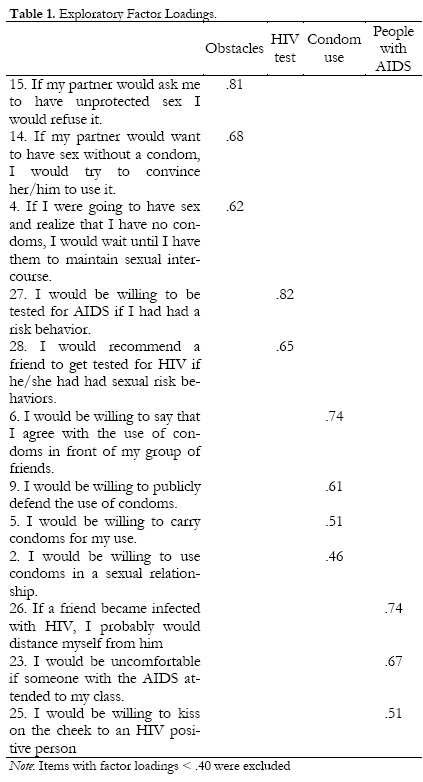
Initially, a series of exploratory analyses of principal components using oblique rotation with the total sample were made. The criteria for obtaining the factor solution were: a) retaining factors with eigenvalue equal to or greater than 1, b) assigning items with loads of .40 or greater to each factor, and c) including at least 3 items in each factor. We found four factors with eigenvalue greater than 1 (Kaiser criterion for retention of factors), which explained 64.63% of the variance. Fourteen items were removed because they had low saturation or because of high saturation on two factors.
A robust factor solution of four factors consisting of 12 items was established (the KMO index = 0.77 and Bartlett test was significant) (Table 1). Factor 1, Obstacles, includes the subject's attitude to condom use through situations were safe behaviors could be under negative influences as pressure of others or barriers to use the condom. This factor is made up of 3 items that explain 28.33% of the variance. Factor 2, Attitudes towards HIV test, includes the situations of doing or recommend the HIV-test to others after a risk behavior. It consists of 2 items that explain 13.35% of the variance. Factor 3, Attitudes towards condom use, evaluates the subject's predisposition to defend, use or have condoms ready to use. It is a 4-item component explaining 11.61% of the variance. Factor 4, Attitudes towards people living with AIDS, it is made up of 3 items including situations of support, discomfort and close relation with affected persons and it explains 10.33% of the variance.
Internal Consistency
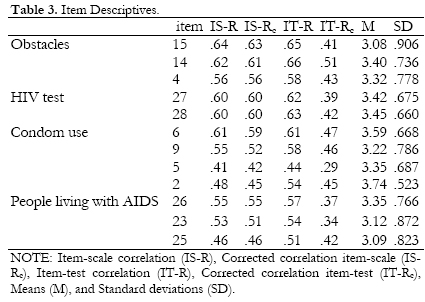
The coefficients of reliability (Cronbach's Alpha) for the questionnaire were .77. The values of Alpha coefficient for the factors were above .70 for all the subscales excepting People living with AIDS (.69) (see Table 2). In Table 3 are presented the item-subscale correlations which were acceptable in a range from .42 to .63. Only 1 item presented an item-test correlation of less than .30, indicating a good performance for most items.
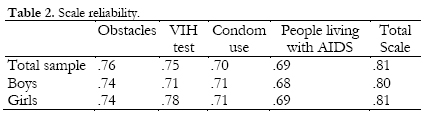
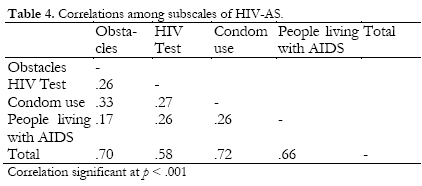
The coefficient of reliability is known to be affected by the variability of the group and the length of the test (Novick & Lewis, 1967). In the present study, is a quite homogeneous group (adolescents between 14 and 18 years) is valued and there are few items per dimension (three dimensions of two and three items). However, the reliability of the subscales are greater than .70, except for one factor, People living with AIDS, therefore the scale is reliable but the use of that subscale is not recommended outside the context of HIV-AS scale. Furthermore, this scale present lower correlations with the others, which indicates that attitudes related to behaviors are not so associated to attitudes towards people living with AIDS. Correlations among subscales of HIV-AS are presented in Table 4.
Concurrent Validity
To assess the concurrent validity of the scale the HIV-AS scores were correlated with the Multicomponent AIDS Phobia Scale (MAPS) due to the conceptual and practical relation between these concepts. The results show the statistically significant relation (p < .01) between the MAPS and the total score of HIV-AS (r = -.48), the factor Obstacles (r = -.19), HIV Test (r = -.23), Condom Use (r = -.31), and People living with HIV (r = -.60). This dimension also gets the lowest correlation with the MAPS scale. Also, the correlation with the percentage of condom use was calculated, finding significant correlations (p < .01) with the total score of HIV-AS (r = .30), Obstacles (r = .39) and Condom Use (r = .22), and HIV Test (r = .11; p < .05).
Test-retest Reliability
A subsample consisting of 832 adolescents completed self-report measures after a period of 10 weeks during which there was no intervention. One hundred and forty-two males and 215 female were between 14 and 15, 141 males and 220 were 16, 46 males and 68 females were between 17 and 18. The test-retest reliability (Pearson correlation coefficient) was r = .60 (p < .01) for the full scale. For the subscale Obstacles was r = .57 (p < .01), the subscale HIV Test was r = .26 (p < .01), the subscale Condom Use was r = .49 (p < .01), and the subscale People Living with HIV was r = .58 (p < .01).
Confirmatory Factor Analysis
Two alternative models were tested: 1) the model of four independent factors and 2) four-factor model allowing intercorrelations between them. Chi-square statistic indicates the degree of correspondence between the proposed model based on the theory and exploratory results with the empirical data. A well-fitting model should be statistically non-significant, however this test is very sensitive to large sample sizes, as it is in this case, that explains the significance of this test. Therefore, we include also the root mean square error of approximation (RMSE), which is a badness-of-fit measure and it was lower than .05 as it is recommended (Kline, 2005). Three different indices of adjustment were considered to measure the fit of the models, non-standard adjustment index (NNFI) (Bentler & Bonnett, 1980), the comparative fit index (CFI), and the goodness of fit statistic (GFI) (Bollen, 1989). Table 5 presents the value of those indices for the four-factor model allowing intercorrelations since this was the model which obtained the best fit, all values were greater than .90 as suggested by Hu & Bentler (1998).
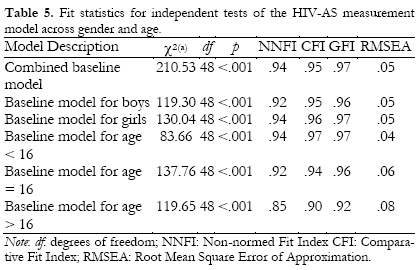
Factorial Invariance: Goodness of Fit Indices
In order to establish intergroup differences according to age and sex through a questionnaire, it is crucial to first establish that the factor structures are identical. For this purpose, factor invariance analysis to test whether the four-factor model for the 12 items of HIV-AS was equal for boys and girls. All factorial loads were limited to be equivalent for boys and girls, as were the correlations between the four factors of HIV-AS. The indicators of goodness of fit revealed that the multiple four-factor model fitted well for both genders. Also, it appeared that the four-factor model was equivalent for younger and older students. The sample was divided into three age groups: 15 or younger, 16 and 17 or older, without differentiating between gender because there was no significant difference in the number of boys vs. girls for each age group. The same indicators showed an appropriate fit in the three age groups (Table 6).
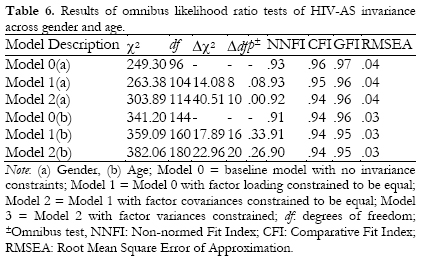
The chisquare values (with degrees of freedom), fit indices and change in CFI values for the factorial invariance models are presented in Table 5. The base model (uncon-strained) demonstrates generally good model fit. We conclude that model 1 (the factor loadings constrained to be equal) fits as well as Model 2 (the factor covariances constrained to be equal), however there is some significant worsening of model if covariances are constrained to be equal for gender suggesting some differences in terms of attitudes by gender. As a conclusion the findings show that adolescents males and females across the range of 15 to 18 interpreted HIV-AS items in an equivalent fashion.
Discussion
The aim of this study was to analyze the psychometric properties of a new scale to measure the attitudes towards HIV/AIDS among adolescents. The design and evaluation of preventive interventions requires the availability of appropriate instruments to obtain reliable data on the attitudes related to the risk behavior. To date there are no validated instruments to specifically and consciously asses the attitudes towards HIV/AIDS among Spanish adolescents. The results showed that the HIV-AS questionnaire is a reliable and valid instrument for measuring this construct.
The study tested the dimensionality of the questionnaire and according to the results, it seems appropriate to take the factorial structure of HIV-AS as multidimensional, as with other scales in Spanish (Uribe, 2005). The reliability of the questionnaire estimated by Cronbach's alpha coefficient is high.
The HIV-AS scale is brief as it is made up of 12 items, it is easy to correct, interpret, and has adequate psychometric properties compared with other scales that assess the same construct (Camargo & Bousfield, 2009). The factor analysis grouped the 12 items in four final factors that correspond to four areas that may be considered appropriate to assess different kind of attitudes that adolescents have about HIV/AIDS. The coefficients of reliability for each factor were high, indicating internal consistency of the items for he whole test. Factors that are evaluated with the questionnaire are shown as good predictors of the level of attitudes. This result is consistent to other studies, although a sample with different socio-cultural characteristics (Boileau et al., 2008).
The first factor, Attitude under the influence of obstacles, with 3 items, includes the subject's attitude to condom use when there is social pressure or difficulty to obtain condoms. Previous empirical research support the influence of obstacles on sexual risk behaviors (Antón & Espada, 2009; Robles, Piña y Moreno, 2006). The two items which compose the factor 2, Attitudes towards HIV test, includes the situations of doing or recommend the HIV-test to others after a risk behavior. Regarding the factor 3, Attitudes towards condom use, its four items evaluate the subject's predisposition to defend, use or have condoms ready to use, demonstrating a high degree of acceptance of the sexual relations, in order to prevent HIV/AIDS. Also, Boileau et al. (2008) obtained in the validation of their scale of attitudes toward condom use, one factor that refers to the preventive properties of condoms to prevent unwanted pregnancies and prevention of HIV/AIDS. Finally, the factor 4, Attitudes towards people living with AIDS, includes situations of support, discomfort and close relation with affected persons.
This study has several strengths and limitations. First, the study contributes to the scientific and applied work on health promotion with a new specific instrument to assess an important variable related to sexual risk behaviors among adolescents. Assessment of attitudes should be complemented with other variables involved in sexual risk behavior, as knowledge regarding HIV for which valid instrument for Spanish adolescents are available (Espada et al., 2009). The sample size and geographical dispersion provides also with a substantial validation of the study. Limitations include that the convergent validity with anxiety and attitudes to AIDS (MAPS and HIV-AS scales, respectively) was assessed; it was not high for all subscales of the HIV-AS. As for test-retest reliability, the values were acceptable except in the subscale of HIV Test, which has a value of .26. One possible explanation for this finding is that the test-retest coefficient is affected by the number of items, especially if they are very related, as is the case. This is the lowest number of subscale items and very interrelated. It can also be a reason of content because these items refer to an attitude that can easily change over time without ever having been an intervention in the middle but only by the fact that attitudes have been assessed, as indicated Wood, Kallgren, & Mueller (1985).
In conclusion, the scale HIV-AS is simple to administer and correct and can be used in schools and community contexts to quickly assess the attitudes related to HIV/AIDS in adolescents. It is therefore proposed as a useful tool in future research and to be used for the evaluation of prevention programs. Future research should examine applications of the scale for use with adults and vulnerable populations.
References
1. Abalo, J., Lévy, J. P., Rial, A., & Varela, J. (2006). Invarianza factorial con muestras múltiples. In J. P. Lévy & J. Varela (comp.), Modelización con estructuras de covarianzas en Ciencias Sociales. A Coruña: Netbiblio. [ Links ]
2. Ajzen, I. & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood Cliffs, New Jersey: Prentice-Hall. [ Links ]
3. Antón, F. A. y Espada, J. P. (2009). Consumo de sustancias y conductas sexuales de riesgo para la transmisión del VIH. Anales de Psicología, 25, 2, 344-350. [ Links ]
4. Bentler, P. M. & Bonnet, D. G. (1980). Significance test and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88, 588-606. [ Links ]
5. Bermúdez, M. P., Sánchez, A. I., & Buela-Casal, G. (2003). Adaptación castellana de la Escala VIH/sida-164. Revista Mexicana de Psicología, 20(1), 95-111. [ Links ]
6. Bermúdez, M. P., Buela-Casal, G., & Uribe, A. F. (2005). Adaptación al colombiano de la escala VIH-65. Granada: Universidad de Granada. [ Links ]
7. Boileau, C., Rashed, S., Sylla, M., & Zunzunegui, M. V. (2008). Monitoring HIV risk and evaluating interventions among young people in urban West Africa: Development and validation of an instrument. AIDS Education and Prevention, 20(3), 203-219. [ Links ]
8. Bollen, K. A. (1989). Structuralequations with latent variables. New York: Wiley. [ Links ]
9. Byrne, B. M., Shavelson, R. J., & Muthén, B. (1989). Testing for the equivalence of factor covariance and mean structures: The issue of partial measurement invariance. Psychological Bulletin, 105, 456-466. [ Links ]
10. Camargo, B. & Bousfield, A. (2009). Social representations, risk behaviors and AIDS. The Spanish Journal of Psychology, 12, 2, 565-575. [ Links ]
11. Espada, J. P., Huedo-Medina, T. B., Orgilés, M., Secades, R., Ballester, R. & Remor, E. (2009). Psychometric properties of the HIV/AIDS Knowledge Scale for Spanish adolescents (HIV-KS). Health and Addictions, 9, 149-164. [ Links ]
12. Givaudan, M., Leenen, I., Van de Vijver, F., Poortinga, Y., & Pick, S. (2008). Longitudinal study of a School based HIV/AIDS early prevention program for Mexican Adolescents. Psychology, Health and Medicine, 13(1), 98-110. [ Links ]
13. Harrel, J. P., & Wright, L. W. (1998). The development and validation of the Multicomponent AIDS Phobia Scale. Journal of Psychopathology and Behavioral Assessment, 20, 3, 201-216. [ Links ]
14. Hu, L. & Bentler, P. M. (1998). Fit indices in covariance structure modeling: sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424-453. [ Links ]
15. Ito, K., Kalyanaraman, S., Ford, C., Brown, J., & Miller, W. (2008). "Lefs talk about sex": Pilot study of an interactive CD-ROM to prevent HIV/STIS in female adolescents. AIDS Education and Prevention, 20(1), 78-89. [ Links ]
16. Jennrich, R. I. & Sampson, P. F. (1966). Rotation for simple loadings. Psychometrika, 31, 313-323. [ Links ]
17. Kline, R. B. (2005). Principles and practice of structural equation modeling (second ed.). New York: The Guilford Press. [ Links ]
18. Lameiras, M., Rodríguez, Y., & Dafonte, S. (2002). Evolución de la percepción de riesgo de la transmisión heterosexual del VIH en universitarios/as españoles/as. Psicothema, 14, 2, 255-261. [ Links ]
19. Marsh, H. W. (1989). Age and sex effects in multiple dimensions of self-concept: Preadolescence to early adulthood. Journal of Educational Psychology, 81, 417-430. [ Links ]
20. Marsh, H. W., Relich, J. D., & Smith, I. D. (1983). Self-concept: The construct validity of interpretations based upon the SDQ. Journal of Personality and Social Psychology, 45, 173-187. [ Links ]
21. Marsh, H. W., Ellis, A., Parada, R. H., Richards, G., & Heubeck, B. G. (2005). A Short version of the Self Description Questionnaire II: Operationalizing criteria for short-form evaluation with new applications of confirmatory factor analyses. Psychological Assessment, 17, 81-102. [ Links ]
22. Muñoz-Silva, A., Sánchez-García, M., Martins, A., & Nunes, C. (2009). Gender differences in HIV-Related sexual behavior among college students from Spain and Portugal. The Spanish Journal of Psychology, 12, 2, 485-495. [ Links ]
23. Novick, M. R., & Lewis, C. (1967). Coefficient alpha and the reliability of composite measurements. Psychometrika, 32(1), 1-13. [ Links ]
24. Paniagua, F. A., O'Boyle, M., Wagner, K. D., Ramírez, S. Z., Holmes, W. D., Nieto, J. F., & Smith, E. M. (1994). AIDS-Related items for developing an AIDS questionnaire for children and adolescents. Journal of Adolescent Research, 9, 311-339. [ Links ]
25. Paniagua, F. A., O'Boyle, M. D., & Wagner, K. D. (1997). Gender Differences on HIV /AIDS Related Issues Among Psychiatrically Hospitalized Adolescents. Journal of HIV/AHDS Prevention and Education for Adolescents and Children, 1 (3-4), 53-63. [ Links ]
26. Piña, J. A., Lozano, D. I., Vázquez, P. y Carrillo, I. C. (2010). Motivos y uso de preservativo en estudiantes universitarios de Ciudad Juárez (México). Anales de Psicología, 26,1, 18-26. [ Links ]
27. Robles, S., Piña, J. A. y Moreno, D. (2006). Determinantes del uso consistente del condón en mujeres que tienen sexo vaginal, oral o anal. Anales de Psicología, 22, 2, 200-204. [ Links ]
28. UNAIDS (2010). UNAIDS Report on the Global AIDS Epidemic. Downloaded December 15 2010 from http://www.unaids.org. [ Links ]
29. Uribe, A. F. (2005). Evaluación de los factores psicosociales de riesgo para la infección por el VIH / sida en adolescentes colombianos. Unpublished Doctoral Dissertation. Universidad de Granada. [ Links ]
30. Uribe, A. F., Valderrama, L., Sanabria, A. M., Orcasita, L., & Vergara, T. (2009). Descripción de los conocimientos, actitudes, susceptibilidad y autoeficacia frente al VIH/sida en un grupo de adolescentes colombianos. Pensamiento Psicológico, 5, 12, 29-44. [ Links ]
31. Vandenberg, R. J. & Lance, C. E. (2000). A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organizational Research Methods, 3, 4-70. [ Links ]
32. Vega, A. & Lacoste, J. A. (1995). Niños, adolescentesy sida: Problemática psicosocial e intervención educativa. Valencia: Promolibro [ Links ]
33. Wood, W., Kallgren, C. A., & Mueller, R. (1985). Access to attitude-relevant information in memory as a determinant of persuasion: The role of message attributes. Journal of Experimental Social Psychology, 21, 73-85. [ Links ]
34. Zometa, C. S., Dedrick, R., Know, M. D., Westhoff, W., Siman, R., & Debaldo, A. (2007). Translation, cross-cultural adaptation and validation of an HIV/AIDS knowledge and attitudinal instrument. AIDS Education and Prevention, 19(3), 231-244. [ Links ]
![]() Correspondence:
Correspondence:
José P. Espada,
Departamento de Psicología de la Salud,
Miguel Hernández University,
Avda. de la Universidad, s/n
03202. Elche, Alicante, (Spain).
E-mail: jpespada@umh.es
Artículo recibido: 4-7-2011
revisado: 20-02-2012
aceptado: 27-02-2012

