










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAnales de Psicología
On-line version ISSN 1695-2294Print version ISSN 0212-9728
Anal. Psicol. vol.33 n.2 Murcia May. 2017
https://dx.doi.org/10.6018/analesps.33.2.232371
The Relationship of Sexism and Gender Ideology to Self-Concept and Self-Esteem in Persons with Spinal Cord Injury
Relaciones entre sexismo e ideología de género con autoconcepto y autoestima en personas con Lesión Medular
Manuela Torregrosa-Ruiz, María A. Molpeceres and José M. Tomás
Facultad de Psicologa. Universitat de Valencia (Spain)
ABSTRACT
The process of adapting to a physical disability is complex and multi-dimensional. It is influenced by many variables that affect adequate life adjustment and psychological wellbeing. This study addresses the specific effects of sexism and gender stereotypes on self-esteem and selfconcept in persons with spinal cord injury (SCI). The research design is cross-sectional and correlational. The sample comprises 127 persons, including 95 men and 32 women, with a long-term spinal injury. The results of the MANOVAs do not demonstrate statistically significant differences based on sex for the following variables: self-esteem, self-concept, traditional sexism and neosexism. The relationships among variables suggest that negative relationships exist between neosexism and family and emotional self-concept and self-esteem among men with SCI, though not among women with SCI. The discussion emphasizes the important role of intervention programs that strengthen gender equality in order to reduce sexism.
Key words: Gender; disability, spinal cord injury; self-esteem; self-concept; sexism; neosexism.
RESUMEN
El proceso de adaptación a una discapacidad física sobrevenida es complejo y multidimensional. En él influyen muchas variables que pueden condicionar un adecuado ajuste vital y conseguir bienestar psicológico. Este estudio aborda los efectos específicos del sexismo y los estereotipos de género en la autoestima y autoconcepto de las personas con lesión medular (LM). El diseño es transversal y correlacional. La muestra está constituida por 127 personas con lesión medular de larga evolución, 95 varones y 32 mujeres. Los resultados de los MANOVAS no muestran diferencias estadísticamente significativas en función del género en las siguientes variables: Autoestima, Autoconcepto, Sexismo Tradicional y Neosexismo. Las relaciones entre variables sugieren que existen relaciones negativas entre neosexismo, autoestima y autoconcepto emocional y familiar en varones con LM, pero no en mujeres con LM. La discusión plantea el relevante papel que pueden tener los programas de intervención que fomenten la igualdad de género para disminuir el sexismo.
Palabras clave: Género; discapacidad; lesión medular; autoestima; auto-concepto; sexismo; neosexismo.
Introduction
Spinal cord injury (SCI) is among the most serious disabilities a person can face, and significant efforts have been made to promote coping in order to foster adaptation to a new situation that has an impact on all areas of life, including physical, psychological and social aspects (Rueda & Aguado, 2003). This type of event has permanent consequences and is undoubtedly traumatic and difficult to face, as it causes major changes in a person's life and affects several variables that influence life adjustment and psychological wellbeing. Due to its seriousness and the breadth of the areas affected, SCI is the physical disability that has garnered the most attention, research and publications, particularly at the international level (Aguado & Alcedo, 1995). However, in Spain, relatively little research has been conducted on the needs of persons with SCI-particularly women-and possible gender differences that may exist (Aguado, Alcedo, García & Arias, 2010; Alcedo, Aguado, García & Arias, 2010).
According to the most recent sociological study conducted in Spain regarding the social and demographic realities of this demographic (Huete, Díaz, Ortega & Esclarín, 2012), SCI can occur in a multitude of forms. Nearly 1,000 Spaniards suffer a traumatic SCI each year, for a total affected population of over 30,000 (Fernández-Gómez de Aranda, 2008; Rodríguez & Vaquero, 2009), although it is difficult to calculate the prevalence of SCI, as there is a lack of real census data compiling current figures. SCI affects men and women alike, although the incidence rates are higher among men. Wyndaele & Wyndaele (2006) found an estimated gender proportion of 3.8 to 1, a proportion that was lower among those over 50 years of age, as the incidence of nontraumatic injuries increases with age.
SCI can cause drastic changes in quality of life. It implies adapting to a new situation that is complex and multidimensional, as it is affected by biological, psychological, social and environmental factors (Trieschmann, 1988).
Emphasis has been given in recent decades to the importance of self-concept and self-esteem as part of subjective wellbeing, and this has come to occupy a central role in explanations of human behavior (Tesser, Felson & Suls, 2000). Most authors associate the term 'self-concept' with the cognitive aspects of self-knowledge and use the term 'selfesteem' to signify the evaluative-affective aspects (Garaigor-dobil & Durá, 2006b). It is believed that "self-concept or self-image is the representation that each person has of themselves, the beliefs that a person has about their own psychological, physical, affective, social and intellectual characteristics" (Iniesta, Martínez & Mañas, 2014, pp. 441). Cardenal & Fierro (2003) explain that while self-concept and self-esteem are sometimes used interchangeably, the latter constitutes strictly the evaluative element of self-concept or self-knowledge. Meanwhile, many articles note the importance of both self-concept and self-esteem as protective elements in stressful situations. Thus, personal self-appraisal -in particular negative self-appraisal- can increase vulnerability to various illnesses and diseases and has serious repercussions on health, both physical and psychological.
Personal self-appraisal plays a particularly important role for persons with disabilities, as positive self-concept and selfesteem is vital for personal, social and professional development, areas that are frequently stymied because of the limitations faced by disabled persons. Low self-esteem has been strongly associated with depression in different studies and among different populations, as have many other psychological states, both positive and negative. However, despite the popularity of self-esteem as a psychological variable and its relevance for understanding processes of adaptation and adjustment after injury, literature on this topic is scant (Kalpakjian, Tate, Kisala & Tulsky, 2015).
Hence, as in the case of other disabilities, self-concept and self-esteem are critical variables for the study of SCI and are indicators of positive adjustment to the disability, wellbeing and improved mental health (Peter, Müller, Cieza & Geyh, 2012; van Leewen, Kraaijeveled, Lindeman & Post, 2012). Pérez & Garaigordobil (2007) indicate that the small number of studies that have been conducted regarding selfconcept and self-esteem among persons with motor disabilities have produced contradictory results. A number of studies show that self-concept and self-esteem among persons with disabilities are typically negative, (Boakye, Leigh & Skelly, 2012; Dijkers, 2005), although many other studies do not find differences when compared with persons without disabilities.
Meanwhile, the few studies that have been performed on self-concept and self-esteem among persons with SCI have also produced contradictory results (Burbano, 2015; Cobo Cuenca, Sampietro-Crespo, Virseda-Chamorro & Martín-Espinosa, 2015; Green, Pratt & Grigsby, 1984; Harper et al., 2014; Huang et al., 2014; Kennedy, Gorsuch & Marsh, 1995; Lourenco, Blanes, Salomé & Ferreira, 2014; Ortiz, 1991).
Depression is undoubtedly the most frequently studied indicator of adjustment to SCI (Craig et al., 2015; Dryden et al., 2005; Geyh et al., 2012; Killic, Dorstyn & Guiver, 2013; Peter et al., 2015), and in many cases, women with SCI present higher depressive symptomatology scores than men with SCI (Hartkopp, Bronnum-Hansen, Seidenschnur & Biering-Sorensen, 1998; Krause & Broderick, 2004; Krause, Broderick & Broyles, 2004; Kennedy et al., 1995). However, other studies show that young men score highest in terms of depressive behaviors (Laatsh & Shahani, 1996; Nichols et al., 2012), while studies such as Kalpakjian & Albright (2006) note the absence of gender differences in rates of depression. No general consensus thus exists in the literature regarding the relationship between gender and depression in persons with SCI, as few studies conduct differential analysis by gender (Alcedo et al., 2010; García, 2006).
Diener, Such, Lucas & Smith (1999) state that the relationship between self-esteem and wellbeing is not universal but rather mediated by culture. In this way, each person's system of values or aspirations influences their self-concept and self-esteem. Hence, gender as a cultural system provides cultural reference points that people recognize and assume. Colás & Villaciervo (2007) state that these representations are internalized by subjects in a given culture, structuring and configuring ways of interpreting and acting upon reality, and that internalized gender stereotypes affect the subject's selfconcept, cognitive processes, intellectual aptitude and performance in carrying out tasks. Stereotypes constitute the basis of the construction of gender identity and orient representations of reality and individual behavior (Jiménez, 2005).
In recent years, issues affecting women with disabilities have gained a certain amount of social visibility, despite scant scientific interest. Society has traditionally tended to isolate women, particularly disabled women (Ramiro, 2003). The situation they face is one of "double discrimination" for being female and disabled. The persistence of stereotypes and false beliefs related to the negative image projected by these women-compared with both women who are not disabled and disabled men-reinforces their exclusion from social activities, work and education (Aguado et al., 2010).
Sexism is closely related to gender inequality. Sexism can be defined as discriminatory behavior directed toward persons based on their belonging to a particular biological sex and expected characteristics and behaviors. According to Moya & Expósito (2001), sexism can be understood more broadly as prejudice against women. However, today we can differentiate between old and new forms of sexism. As stated by Moya (2004), traditional sexist attitudes have given way to new, less hostile modalities that are particularly prevalent in the workplace (neosexism) and in relationships (ambivalent sexism). Violent sexism is based on domination, competitiveness and hostility, while benevolent manifestations of sexism utilize protection instead of domination, the complementarity of genders instead of competitiveness and the positive recognition of women instead of hostility. However, despite these different profiles, the common denominator is the belief in the inequality of men and women.
Results of studies on the relationship between gender and sexism among non-disabled people do not show any consensus. While in many studies men score higher in terms of both hostile sexism as well as benevolent sexism and neosexism (Forbes, Collinworth, Jobe, Braun & Wise, 2007; Fowers & Fowers, 2010; Garaigordobil & Aliri, 2013; Garigordobil & Aliri, 2011a, 2011b; Garaigordobil & Maganto, 2013; Lameiras & Rodríguez, 2002; Lameiras & Rodríguez, 2003; Lameiras, Rodríguez, Calado, Foltz & Carrera, 2007; Russel & Trigg, 2004; Trivaglia, Overall & Sibley, 2009; Vaamonde, 2013), other studies do not find gender differences in terms of sexist beliefs (Chen, Fiske & Lee, 2009; Eastwick, Eagly, Glick, Johannesen-Schmidt, Fiske, Blum et al. 2006; Expósito, Moya & Glick., 1998; Glick, Lameiras, Rodríguez, Calado, Foltz & Gonzalez, 2006; Lameiras, Rodríguez & Gonzalez, 2004; Martínez, Paterna & Yago, 2010).
Several studies have analyzed the connections between sexism and self-concept or self-esteem, although the results indicate a different influence of sexism in men and women. With regard to neosexism, certain studies find worse selfconcept and self-esteem among men with higher scores (Garaigordobil & Durá 2006). Similarly, Angell (2005) finds that those who are less sexist have greater self-esteem. Regarding ambivalent sexism, certain studies find that no relationship exists between sexism and self-concept among women, while men with high sexism scores also have high self-concept (Garaigordobil & Aliri, 2011a; Garaigordobil & Aliri, 2013). Other studies state that women who display benevolent sexism have higher self-esteem (Lameiras & Rodríguez, 2003; Schmitt, Branscombe & Postmes, 2003). It has also been found that self-esteem can moderate the connection between perceived sexist events and psychological distress (Landry, 2007; Moradi & Subich, 2004) and protect against the effects of sexism (Collins, 2002). Overall, the results of the meta-analysis by Schmitt, Branscombe & García (2014) support the idea that perceived discrimination is important due to the adverse effects it has on psychological wellbeing.
Knowledge regarding the specific effects of sexism on self-concept and self-esteem on persons with SCI can illuminate and promote understanding of the psychological aspects involved in adjusting to this injury, and more specifically, its mediating role in coping and psychological wellbeing. Women with disabilities in general and with SCI in particular face certain stereotypes that are not empirically verified and that generate a negative social image of women with disabilities, suggesting that they are more vulnerable, more likely to be depressed and have low self-esteem, more anxious, reserved, etc., than men with disabilities (Arnau, 2005; Crawford & Ostrove, 2003).
This study is motivated by the scarcity and disparity of research regarding these variables and the poor trajectory and rigor of the existing analyses of these variables among persons with disabilities-specifically SCI. The main objective of this study is to analyze whether gender differences exist in the variables examined here and to explore the relationship between sexism and gender stereotypes and selfconcept and self-esteem in persons with SCI.
In light of the research described above, the following hypotheses are presented: 1) No gender differences exist in the psychological scales known as the Self-Esteem Scale (SES), the Self-Concept Scale (AF5), the Sex Role Ideology Scale (SRIS) and the Neosexism Scale (NS); and 2) Sexism is negatively correlated with self-esteem (SES) and self-concept (AF5) among both women and men, although the specific correlation pattern among the different dimensions of these variables may vary between the sexes.
Method
Procedure and participants
The research was conducted using a cross-sectional survey. Participants consisted of 127 persons with SCI. The selection criteria were i) suffers from chronic SCI and has completed at least one year of medical-functional rehabilitation, ii) has completed basic education, and iii) knows how to use the internet and social media (to guarantee correct completion of surveys).
The first phase of recruitment of persons with SCI was carried out through SCI organizations and associations. In a second phase, to increase the number of participants, the study was shared through Facebook. All participants received information about the study and its objectives, as well as a guarantee of confidentiality and anonymity. The online survey was carried out using a platform known as Limesurvey in August and September of 2012.
The sample comprises 127 persons with SCI. Among the participants, 25.2% come from the province of Valencia, 11.8% from Barcelona, 9.4% from Alicante and 7.1% from the Baleares Islands. The remaining 46.4% are from other provinces throughout Spain. The majority-94 participants (or 74%)-resides in urban areas, and 74.8% are men, while 25.2% are women. Participants range from 20 to 72 years of age, with an average age of 40.5 years (SD= 9.78). The number of years since injury ranges from a minimum of one year to a maximum of 64 years, with an average of 17.07 years (DT=11.55). Most have complete SCI (67.7%), compared with incomplete SCI (32.3%), and more common among the latter category are paraplegics (78%) compared with tetraplegics (22%). No statistically significant relationship was found between type of injury and gender (χ2(1)=2.57, p=.109). Concerning etiology, there is a preponderance of traumatic injuries: 59.8% (N=76) are due to traffic accidents, 10.2% (N=13) to accidents in the workplace, 3.9% (N=5) to sports accidents and 9.4% (N=12) to other types of accidents. For the remaining 15.7% (N=20) of participants, SCI resulted from various illnesses, and in one case, from an unknown cause.
Instruments
To measure the variables of interest, an online questionnaire comprised of different components was created:
1) Socio-demographic questionnaire: Gathers personal information, basic socio-demographic information and information regarding the type and level of disability.
2) Self-Esteem Scale (Rosenberg, 1965). Evaluates general self-esteem using 10 items with four points Likert-type scale (from strongly agree to strongly disagree). The items with negative statements are inverted (3, 5, 8, 9, 10), and all items summed up to generate scores. The total score ranges from 10 to 40, with 10 indicating the lowest self-esteem and 40 the highest. Cronbach's alpha was 0.89.
3) Five-Factor Self-Concept Questionnaire (AF5) (García & Musitu, 2001). Composed of 30 items, this measures five self-concept dimensions: academic/work (subject's perception of the quality their performance in their role), social (perception of performance in social relations), emotional (perception of emotional state and responses to specific situations), family (perception of involvement, participation and integration in the family setting) and physical (perception of physical appearance and condition). Each dimension is measured using six items on a scale from 1 to 99, although the response scale was adapted to a Likert-type model with five response levels (from never to almost always). The alpha coefficients of the dimensions were as follows: academic, 0.82; social, 0.82; emotional, 0.78; family, 0.82; and physical, 0.81. The five AF5 dimensions are arranged such that the higher scores imply greater self-esteem.
4) Sex-Role Ideology Scale (SRIS), short version (Moya, Navas & Gómez, 1991; Lameiras & Rodríguez, 2002). A measure of traditional sexism that gauges beliefs regarding the roles, behaviors and relationships that men and women should have. Gender ideology is conceived of as a dimension where feminist-egalitarian ideology stands in opposition to traditional ideology. Traditional ideology emphasizes differences between the sexes and views women as weak and in need of protection. The short version comprises 12 items and was developed and validated for a Spanish-speaking population (Moya, Expósito & Ruiz, 2000); it uses a Likert-type scale with five response levels (from strongly disagree to strongly agree). Cronbach's alpha was 0.91. A higher value indicates a higher opinion of women, and hence, a more progressive and egalitarian view of gender roles between men and women.
5) Neosexism Scale (NS) (Tougas, Brown, Beaton & Joly, 1995; Spanish version by Moya & Expósito, 2001). The objective of the test is to measure neosexism, defined as a "manifestation of a current conflict between egalitarian values and residual negative feelings toward certain women" (Tougas et al., 1995, cited in Garaigordobil and Dura, 2006). It consists of 11 items with seven Likert-type response levels (1=totally disagree to 7=totally agree). The alpha coefficient was 0.75. Higher scores reveal more strongly sexist attitudes.
Data analysis
The data were analyzed using the statistics program SPSS v.19.0. The statistical process employed to prove or disprove the existence of differences based on sex in the different psychological variables was multivariate analysis of variance (MANOVA), in which the independent factor or variable was gender and the dependent variables were the average scores obtained in the scales. The normality of the distribution was previously confirmed using a non-parametric Kolmogorov-Smirnov test, and the homoscedasticity of the sample was determined using Levene's test. The level of significance was .05.
In what follows, Pearson correlations were carried out among all the psychological variables to determine the level of association between them based on sex and confirm whether the level of association between these variables demonstrates different patterns among men and women. Finally, the correlations between variables in men and women were contrasted to evaluate the possible moderating effects of sex.
Results
Differences based on sex
To explore whether significant gender-based differences in self-concept and self-esteem exist among the participants, multivariate analysis of variance (MANOVA) was conducted, the results of which demonstrate a lack of statistically significant gender-based differences in said variables: Wilks's Lambda = .918; F(6,114) = 1.961; p = .119; η2 = .082, (see Table 1). The relationships were not altered by adding time since injury as a covariable: Wilks's Lambda = .922; F(6,114) = 1.93; p = .199; η2 = .078.
This result indicates that our participants' self-esteem scores are independent of sex. The averages are provided in Table 2.
Regarding the components of self-concept, the results also do not demonstrate evidence of significant gender-based differences in any of the sub-scales. The statistical descriptions are provided in Table 2.
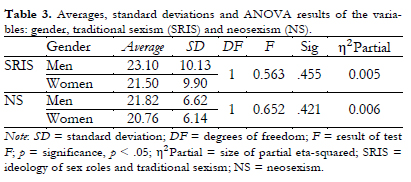
A second multivariate analysis of variance (MANOVA) was subsequently conducted using the Sex-Role Ideology Scale and Neosexism Scale as dependent variables and sex as an independent variable. Once again, no significant differences were found: Wilks's Lambda = .993, F(2,112) = 0.371; p = .691, η2 = 0.007 (see Table 1). The inclusion of the covariable of time since injury did not alter the results: Wilks's Lambda = 0.994; F(2,111) = 0.331; p = .715; η2 = 0.006. The statistical descriptions are provided in Table 3.
The relationship between self-esteem and sexism
To explore possible relationships between self-esteem and sexism, Pearson correlation coefficients between the variables were calculated in order to determine the level of association between them. It was determined that traditional sexism (SRIS) and neosexism (NS) demonstrated significant relationships with self-esteem and with various components of the self-concept scale (AF5), as shown in Table 4.
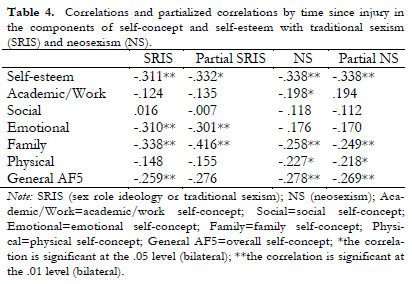
The correlation coefficients obtained demonstrate the existence of significant negative correlations between self-concept/self-esteem and traditional sexism/neosexism. Particularly significant are the relationships between self-esteem and the emotional and family components of self-concept. Therefore, the data suggest that persons with high selfconcept and self-esteem have less sexist beliefs and a more egalitarian gender role ideology.
To analyze these relationships more deeply, Pearson correlations were again calculated between scores on the SRIS and NS questionnaires and scores on the self-concept and self-esteem scales, this time dividing the sample in men and women, to determine whether the level of association between these variables demonstrates different patterns for men and women. The results of these correlations for men and women are shown in the first two columns of Table 5. It can be observed that, generally, relationships with the components of self-esteem are negative and greater among men.
To further interpret these results, a correlation contrast was performed using the Fisher z-transformed correlation coefficients obtained for men and women. The objective of this analysis was to evaluate the possible moderating effect of gender on the relationship between self-esteem and sexism. The results of the contrast test of the two independent correlations (in men and women) are shown in column three of Table 5. They demonstrate that just two contrasts make it possible to reject the null hypothesis and hence to affirm that the difference found in the correlations between men and women regarding the variables of self-esteem/self-concept and sexism/neosexism is not due to chance. This allows us to state that a relationship exists between the two variables for male participants, although not for female participants. Concretely, regarding the dimension of emotional self-concept (z= 2.169; p< .05) and family self-concept (z= 2.471; p< .05), neosexist men with SCI manifest poorer emotional and family self-concept than neosexist women.
In sum, these results suggest that sexism, and particularly neosexism, is negatively correlated with how individuals conceive of themselves at the emotional and family level, although it is men with SCI who demonstrate this finding. Among women, while significant correlations were found between the variables of self-concept/self-esteem and sexism, these correlations were weaker and less clear, perhaps because the sample of women with SCI participating in the study is much smaller than the sample of men.
Discussion
As mentioned above, this study attempts to investigate the specific effects of sexism on self-concept and self-esteem among persons with SCI, taking into account possible gender differences and delving into the psychological aspects involved in adjusting to a physical disability. These variables have not been widely studied in the context of disability.
Regarding the first hypothesis, which posited that no significant gender-based differences exist in the psychological scales, we can state that in terms of self-esteem/self-concept, our data does not show significant differences between men and women with SCI.
No agreement exists in the scientific literature regarding whether the variable of gender can be a factor in the development of low self-esteem/self-concept and depression among persons with SCI. Studies on this topic date back four decades. For example, Richardson & Tupper (1975) address the components of extraversion, neuroticism, depression and anxiety among men and women with SCI and conclude that women are more neurotic, depressive and anxious, while men score higher on obsession and generalized anxiety. Meanwhile, other authors such as Cook (1979) do not find differences between men and women with SCI in terms of depression, anxiety and denial of their situation when faced with SCI. Writing more recently, Kalpakjian and Albright (2006) and Aguado et al. (2010) do not support the widely disseminated and accepted hypothesis that women with SCI present more frequent and intense cases of depression than men with SCI.
Our results do not corroborate the implications of a great number of studies cited previously that find a greater predisposition toward low self-concept and self-esteem among women with SCI. The results of this study, on the other hand, are in accordance with the findings of Kennedy et al. (1995), which do not indicate any significant difference between men and women regarding self-esteem, body image and social relations, and Harper et al. (2014), which similarly finds no differences in self-esteem. Other studies carried out among disabled populations, such as Pérez & Garaigordobil (2007), analyze gender difference in terms of self-concept and self-esteem among persons with motor disabilities and similarly find no evidence of significant differences between men and women. This is consistent with other articles that find no differences among the general population (Garaigordobil, Durá & Pérez, 2005; Lameiras & Rodríguez, 2003).
Authors such as Kalpakjian et al. (2015) note that low self-esteem has frequently been linked to depression in various studies and among different populations and that there is evidence that self-esteem also plays a role in the wellbeing of persons with SCI. Thus, the literature review by Peter et al. (2012) regarding psychological resources in persons with SCI demonstrates a positive association between self-esteem and mental wellbeing, health, community participation, power, hope and efficient coping and suggests that self-esteem is often compromised after suffering SCI.
Regarding traditional sexism and neosexism, differences between men and women were absent as well. No articles were found analyzing these variables in persons with disabilities in general or SCI in particular, and hence, it is difficult to contrast the results. Our results demonstrate that men with SCI have slightly higher scores in terms of traditional sexism and neosexism than women but that none of these differences are statistically significant.
A recent study by Garaigordobil & Aliri (2013) among the general population finds significantly higher rates of hostile sexism among men of all age groups and higher rates of benevolent sexism until age 54, which is consistent with the findings of other researchers (Feather, 2004; Forbes et al., 2007; Fowers & Fowers, 2010; Garaigordobil & Aliri, 2011a, 2011b; Garaigordobil & Maganto, 2013; Glick & Fiske, 1996; Lameiras & Rodríguez, 2003; Lameiras et al., 2007; Masser & Abrams, 1999; Russel & Trigg, 2004; Travaglia et al., 2009; Vaamonde, 2013). However, the results of our investigation coincide with those of many other studies that also find no differences (Chen et al., 2009; Eastwick et al., 2006; Expósito et al., 1998; Glick, Lameiras & Rodríguez, 2002; Lameiras & Rodríguez, 2002; Lameiras et al., 2006; Martínez et al, 2010). The differences and contradictions in different studies of the general population could be connected to age differences in the samples, as many are conducted only among university students.
In sum, we can affirm that the differences in scores in the psychological variables analyzed are not influenced by the gender of the participants. These results confirm our first hypothesis and are consistent with findings obtained in other studies in which no gender-based differences were found in self-concept and self-esteem among persons with SCI (Kennedy et al. 1995; Pérez & Garaigordobil, 2007). Undoubtedly, the condition of being disabled continues to be stigmatized in our culture, and it is necessary to reflect on the double vulnerability of women with disabilities, who are frequently associated with negative meanings and stereotypes that generate exclusion, including lower self-esteem compared to male peers, stereotypes that constitute social barriers that limit women's full development.
Our second hypothesis proposed an inverse relationship between sexism and self-esteem/self-concept in persons with SCI but predicted that relationships between the different dimensions of these variables might differ between men and women. Findings in the literature tend to support a negative relationship between sexism and self-esteem/self-concept for women; for men, the relationship between self-esteem/self-concept and sexist beliefs is less clear. Although the direction of the relationships is not entirely clear in the research, it can be assumed a priori that greater sexism in adults with SCI can negatively affect self-esteem/self-concept for both men and women because SCI would make it more difficult for women to play their prescribed roles as caretakers in the domestic environment and for men to play productive roles in public spaces.
In the sample of women, negative correlations were found between the components of emotional and family self-concept and traditional sexism (SRIS). These results are not surprising, as they are in line with many studies performed among the general population that find that the acceptance of a subordinate role is negatively correlated with women's self-esteem. Meanwhile, the traditional female role is characterized above all by its focus on the private domestic sphere and intimate relationships. A plausible explanation for our results may be that the more women with SCI have internalized the ideology of the traditional caretaker role, the worse the perception they have of themselves in terms of their family and emotional lives, given that they feel they cannot fulfill the role associated with their gender in the domestic sphere. This perception can be conditioned by the circumstances of their physical disability that make it difficult to assume the role, as society often overlooks these women in feminine stereotypes (family caregivers, mothers, spouses, etc.). In any case, research on gender role identity and sexism among persons with disabilities is almost completely lacking.
Among men with SCI, significant negative correlations were found between self-esteem and traditional sexism, such that men who believe in more stereotyped and sexist gender roles have lower self-esteem, a relationship that was not found among women. Meanwhile, as is true for women, men with SCI demonstrate worse emotional and family selfconcept the more they subscribe to traditional gender ideology. However, unlike for women, several studies among the general population note a relationship between self-esteem and sexism in men that differs from what is found here among men with SCI. For example, our results partially contradict those of Garaigordobil & Aliri (2011) that suggest that among the general population, a weak correlation between sexism and self-concept is only found in men, among whom there is a slight positive correlation between ambivalent and benevolent sexism and self-concept. This could be because men with SCI perceive that they cannot fulfill their role in society because of their disability, as it makes it difficult for them to perform the roles traditionally associated with their gender: leader, provider, father, husband and sexual partner.
The results with regard to neosexism are also peculiar, given that significant negative relationships were found between this variable and self-esteem and family/emotional/physical self-concept in men with SCI, though not in women with SCI.
However, the contrast in correlations allows us to state that gender differences with regard to the pattern of correlations are only relevant for emotional and family self-concept and their relationship with neosexism. The issue of why traditional sexism has a negative relationship with self-esteem in persons with SCI of both genders while neosexism only appears to affect self-concept among men is an interesting question, and perhaps the answer can be found in the conceptual difference between traditional sexism and neosexism. Traditional sexism assigns roles based on gender: men and women carry out different roles simply because of their sex, and hence a woman who cannot fully exercise her role as a caregiver (even as she herself must be taken care of) or a man who has difficulties achieving full employment are, from this perspective, incomplete or inadequate. In contrast, neosexism, in accordance with what has been called forms of "symbolic prejudice" (Kinder & Sears, 1981), justifies the greater presence of men in public or professional life based on their greater motivation or individual capacity to perform those roles (Glick & Fiske, 1996; Moya & Expósito, 2001). Therefore, a neosexist man whose public or professional role is suddenly limited can interpret this as evidence of lesser personal abilities, while a neosexist woman could more easily justify this as the product of personal interests or inclinations of her gender.
There are several limitations of this study. First, the results are not easily generalizable, given that the sample is not representative, although it is heterogeneous and varied. Conducting studies with convenience samples is a limitation to consider. A larger sample with a greater representation of women with SCI is recommended. Further, the crosssectional design limits the interpretation of the results obtained. Finally, other factors that were not evaluated here could also mediate the relationship between sexism and self-esteem/self-concept among persons with SCI, which opens the door to future research.
In general, we can conclude that the results described in this article have implications for the design and implementation of intervention programs to combat sexist attitudes and strengthen gender equality among persons with SCI in order to improve their quality of life and wellbeing, given the influence these factors have on self-concept and self-esteem.
References
1. Aguado, A.L., Alcedo, M.A., García, L., & Arias, B. (2010). Personas con lesión medular: diferencias en variables psicológicas desde la perspectiva de género. Psicothema, 22, 659-663. [ Links ]
2. Aguado, A.L., & Alcedo, M.A. (1995). Las personas con discapacidad física. In M.A. Verdugo (Ed.), Personas con discapacidad: Perspectivas psicopedagógicas y rehabilitadoras (pp. 145-184). Madrid: Siglo XXI de España Editores. [ Links ]
3. Alcedo, M.A., Aguado, A.L., Garcia, L., & Arias, B. (2010). Relación entre variables clínicas y psicológicas en mujeres con lesión medular. Universitas Psychologica, 9, 715-727. [ Links ]
4. Angell, M.L. (2005). Race, sex roles, and sexuality. Dissertation Abstracts International: Section B: The Sciences and Engineering, 65(8-B), 4335. [ Links ]
5. Arnau, S. (2005). La perspectiva de la Vida Independiente en las políticas de género y discapacidad. Materiales para confeccionar un Plan de Acción en materia de Mujer con Discapacidad 2005-2008, 1-12. Madrid: Comisión de Mujer del CERMI Estatal. [ Links ]
6. Boakye, M., Leigh, B.C, & Skelly, A.C. (2012). Quality of life in persons with spinal cord injury: comparisons with othen populations. Journal of Neurosurgery: Spine, 17, 29-37. DOI: 10.3171/2012.6.AOSPINE1252. [ Links ]
7. Burbano, M.G. (2015). Competition for health care in women spinal cord trauma. Enfermeria Global, 38, 90-101. [ Links ]
8. Cardenal, V., & Fierro, A.(2003). Componentes y correlatos del Autoconcepto en la escala de Piers-Hams. Estudios de Psicología, 24,101-11. DOI: 10.1174/021093903321329094. [ Links ]
9. Chen, Z., Fiske, S., & Lee, T. (2009). Ambivalent sexism and powereated gender-role ideology marriage. Sex Roles, 60, 765-778. DOI: 10.1007/s11199-009-9585-9. [ Links ]
10. Cobo-Cuenca, A.L., Sampietro-Crespo, A., Virseda-Chamorro. M., & Martín-Espinosa, N. (2015) Psychological impact sexual dysfunction in men with and without spinal cord injury. The Journal of sexual Medicine, 612, 436-444. DOI: 10.1111/jsm.12741. [ Links ]
11. Colás, P., & Villaciervo, P. (2007). La interiorización de los estereotipos de géneros en Jóvenes y Adolescentes. Revista de Investigación Educativa, 25, 35-58. [ Links ]
12. Collins, L.H. (2002). Self-esteem inoculation: Protecting girls from the effects of sexism. In L.H. Collins, M.R. Dunlap & J.C. Chrisler (Eds.), Charting a new course forfeminist psychology (pp. 139-166). Westport, CT,US: Praeger Publishers/Greenwood Publishing Group. [ Links ]
13. Cook, D. (1979). Pyschological adjuntment to spinal cord injury: Incidence of denial, depression and anxiety. Rehabilitation Psychological, 26, 97-104. [ Links ]
14. Craig, A, Nicholson-Perry, K., Guest, R.; Tran, Y., Dezarnaulds, A., Hales, A., Ephraums, C., & Middleton, J. (2015). Prospective Study of the Occurrence of Psychological Disorders and Cormobidities after Spinal Cord Injury. Archives Physical Medicine and Rehabilitation 96, 1426-1434. DOI: 10. 1016/j.apmr.2015.02.027. [ Links ]
15. Crawford, D., & Ostrove, J.M. (2003). Representations of Disability and the Interpersonal Relationships of Women with Disabilities. In M. E. Banks & E. Kaschak (Eds.), Women with Visible and Invisible Disabilities: Multiple Intersections, Multiple Issues, Multiple Therapies (pp. 179-194). Nueva York: The Haworth Press, Inc. DOI: 10.1300/J015v26n03_01. [ Links ]
16. Diener, E., Such, E.M., Lucas, R.E., & Smith, H.L. (1999). Subjective wellbeing: three decades of progress. Psychological Bulletin 125, 276-302. [ Links ]
17. Dijkers, M.R. (2005). Quality of life of individuals with spinal cord injury: a review of conceptualization, measurement and research findings. Journal of Rehabilitation Research and Development, 42, 87-110. [ Links ]
18. Dryden, D.M., Saunders, L.D., Rowe, B.H., Hay, L.A. Yiannakoulias, N., Svenson, L.W., Schopflocher, D.P., & Voaklander, D.C. (2005). Depression following Traumatic Spinal Cord Injury. Neuroepidemiology, 25, 55-61. DOI: 10.1159/000086284. [ Links ]
19. Eastwick, P. N., Eagly, A. H., Glyck, P., Johannesen-Schmidt, M.C, Fiske, S.T., Blum, A., et al. (2006). Is traditional gender ideology associated, with sex-typed mate preferences? A test in nine nations. Sex Roles, 54, 603-614. DOI: 10.1007/s11199-006-9027-x. [ Links ]
20. Expósito, F., Moya, M., & Glick, P. (1998). Sexismo ambivalente: medición y correlatos. Revista de Psicología Social, 13, 159-169. DOI: 10.1174/021347498760350641. [ Links ]
21. Feather, N. (2004). Value correlates of ambivlent attitudes toward gender relations. Personality and Social Psychology Bulletin, 30, 3-12. DOI: 10.1177/0146167203258825. [ Links ]
22. Fernández-Gómez de Aranda, M. (n.d). Lesión Medular sobrevenida: un nuevo enfoque. (Online). Retrieved from: http://www.euitt.upm.es/uploaded/eventos/LESIONES%20MEDULARES%20SOBREVENIDAS_Un%20nuevo%20enfoque.pdf. [ Links ]
23. Forbes, G., Collinworth, L., Jobe, R., Braun, K., & Wise L. (2007). Sexism, hostility toward women, and endorsement of beauty ideals and practices: Are beauty ideals associated with opressive beliefs? Sex Roles, 56, 265-273. DOI: 10.1007/s11199-006-9161-5. [ Links ]
24. Fowers, A. F., & Fowers, B.J. (2010). Social dominance and sexual selfschema moderators of sexist reactions to female subtypes. Sex Roles, 62, 468-480. DOI: 10.1007/s11199-009-9607-7. [ Links ]
25. Garaigordobil, M. (2013). Sexismo y Alexitimia: correlaciones y diferencias en función del género, la edad y el nivel de estudios. Anales de la Psicología, 29, 368-377. DOI: 10.6018/analesps.29.2.132261. [ Links ]
26. Garaigordobil, M., & Aliri, J. (2011 a). Sexismo hostil y benevolente: relaciones con autoconcepto, racismo y sensibilidad intercultural. Revista de Psicodidáctica, 16, 331-350. DOI: 10.1387/RevPsicodidact.998. [ Links ]
27. Garaigordobil, M., & Aliri, J. (2011 b). Conexión intergeneracional del Sexismo: influencia de variables familiares. Psicothema, 23(3), 382-387. [ Links ]
28. Garaigordobil, M., & Durá, A. (2006a). Neosexismo en adolescentes de 14 a 17 años: relaciones con autoconcepto-autoestima, personalidad, psicopatología, problemas de conducta y habilidades sociales. Clinica y Salud, 17, 127-149. [ Links ]
29. Garaigordobil, M., & Durá, A. (2006b). Relaciones de autoconcepto y la autoestima con sociabilidad, estabilidad emocional y responsabilidad en adolescentes de 14 a 17 años. Anales y Modificación de conducta, 32, 37-64. [ Links ]
30. Garaigordobil, M., Durá, A., & Pérez, J.I. (2005). Psychopathological symptoms, behavioural problems and self-concept/self-esteem: A study of adolescents aged 14 to 17 years old. Annuary of Clinical and Health Psychology, 1, 53-63. [ Links ]
31. Garaigordibil, M., & Maganto, C. (2013). Sexismo t trastornos de la conducta alimentaria: Diferencias de género, cambios con la edad y relaciones entre ambos constructos. Revista de Psicopatología y Psicología Clínica, 18, 183-192. DOI: 10.5944/rppc.vol18.num3.2013.12919. [ Links ]
32. García, L. (2006). La perspectiva de género en el proceso de adaptación a la lesión medular,(Tesis doctoral), Departamento de Psicologia, Universidad de Oviedo, Oviedo, España. [ Links ]
33. García, F., & Musitu, G. (2001). Autoconcepto Forma 5. AF5. Madrid: TEA. [ Links ]
34. Geyh, S., Nick, E., Stirnimann, D., Ehrat, S., Müller, R., & Michel, F. (2012). Biopsychosocial outcomes individuals with and without spinal cord injury: a Swiss comparative study. Spinal Cord, 50, 614-622. DOI: 10.1038/sc.2012.21. [ Links ]
35. Glick, P., & Fiske, S.T.. (1996). The Ambivalent Sexism Inventory: Differentiating hostile and benevolent sexism. Journal of Personality and Social Psychology, 70, 491-512. DOI: 10.1037/0022-3514.70.3.491. [ Links ]
36. Glick, P., Lameiras, M., & Rodríguez, Y. (2002). Education and Catholic religiosity as predictors of hostile and benevolent sexism toward women and men. Sex Roles, 47, 433-441. DOI: 10.1023/A:1021696209949. [ Links ]
37. Green, B.C., Pratt, C.C., & Grigsby, T.E. (1984). Self-concept among persons with long-term spinal cord injury. Archives of Physical Medicine and Rehabilitation, 65, 751-754. [ Links ]
38. Harper, L.A., Coleman, J.A., Perrin, P.B., Olivera, S.L., Perdomo, J.L., Arango, J.A., & Arango-Lasprilla, J.C. (2014). Comparison of mental health between individuals with spinal cord injury and able-bodied controls in Neiva, Colombia. Journal of Rehabilitation Research of Development 5, 127-136. DOI: 10.1682/JRRD.2013.04.0000. [ Links ]
39. Hartkopp, A., Bronnum-Hansen, H., Seidenschnur, A., & Biering-Sorenson, F. (1998). Suicide in a spinal cord injured population: its relation to functional status. Archives of Psysical Medicine and Rehabilitation, 79, 1356-1361. [ Links ]
40. Huang, C.Y., Chen, W.K., Lu, C.Y., Tsai, C.C., Lai, H.L., Lin, H.Y., Guo, S.E., Wu, L.M., & Chen, C.I. (2015). Mediating effects of social support and self-concept on depressive symptoms in adults with spinal cord injury. Spinal Cord 53, 413-416. DOI: 10.1038/56.2014.158. [ Links ]
41. Huete, A., Díaz, E., Ortega, E., & Esclarín, A. (2012). Análisis sobre la Lesión Medular en España. Federación Nacional de ASPAYM. Toledo: Intersocial. [ Links ]
42. Iniesta, A., Martínez, A., & Mañas, C. (2014). Autoestima y Diversidad Funcional. International Journal of Development and Educational Psychology, 2, 439-446. DOI:10.17060/ijodaep.2014.n1.v2.459. [ Links ]
43. Jiménez, R. (2005). El aprendizaje cultural de género desde la teoría sociocultural. (Tesis doctoral). Departamento de Métodos de Investigación y diagnóstico de Educación, Universidad de Sevilla, Sevilla. [ Links ]
44. Kalpakjian, C.Z., & Albright K.J. (2006). An examination of depression through the lens of spinal cord injury. Comparative prevalence rates and severity in women and men. Women's Health Issues, 16, 380-388. http://dx.doi.org/10.1016/j.whi.2006.08.005. [ Links ]
45. Kalpakjian C.Z., Tate D.G., Kisala P.A., & Tulsky D.S. (2015). Measuring self-esteem after spinal cord injury: Development, validation and psychometric characteristics of the SCI-QOL Self-esteem item bank and short form. Journal of Spinal Cord Medicine, 38, 377-385. DOI: 10.1179/2045772315Y.0000000014. [ Links ]
46. Kennedy, P., Gorsuch, N., & Marsh, N. (1995). Childhood onset of spinal cord injury, self-esteem and self perception. British Journal of Clinical Psychology, 34, 581-588. DOI: 10.1111/j.2044-8260.1995.tb01492.x. [ Links ]
47. Killic, S.A., Dorstyn, D.S., & Guiver, N.G. (2013). Examining factors that contribute to the process of resilience following spinal cord injury. Spinal Cord 51, 553-557. DOI: 10.1038/sc.2013.25. [ Links ]
48. Kinder, D. R., & Sears, D. O. (1981). Prejudice and politics: Symbolic racism versus racial threats to the good life. Journal of Personality and Social Psychology, 40, 414-431. DOI: 10.1037/0022-3514.40.3.414. [ Links ]
49. Krause, J.S., & Broderick, L.E. (2004). Outcomes after spinal cord injury: comparisons as a function of gender and race and ethnicity. Archives of physical medicine and rehabilitation, 85, 355-362. DOI: 10.1016/S0003-9993(03)00615-4. [ Links ]
50. Krause, J.S. Broderick, L.E., & Broyles, J. (2004). Subjective well-being among African-Americans with spinal cord injury: an exploratory study between men and women. Neurorehabilitation, 19, 81-89. [ Links ]
51. Laatsh, L., & Shahani, B. (1996). The relationship betwween age, gender and psychological distres rehabilitation impatients. Disability & Rehabilitation: An International Multidisciplinary Journal, 18, 604-608. DOI: 10.3109/09638289609166321. [ Links ]
52. Lameiras, M., & Rodríguez, Y. (2002). Evaluación del sexismo moderno en adolescentes. Revista de Psicologia Social: International Journal of Social Psychology, 17, 119-127. DOI: 10.1174/021347402320007555. [ Links ]
53. Lameiras, M., & Rodríguez, Y. (2003). Evaluación del sexismo ambivalente en estudiantes gallegos/as. Acción Psicológica, 2, 131-136. DOI: 10.5944/ap.2.2.526. [ Links ]
54. Lameiras, M., Rodríguez, Y., & González, M. (2004). Evolution of hostil sexism and benevolent sexism in a Spanish sample. Social Indicators Research, 66, 197-211. DOI: 10.1023/B:SOCI.0000003553.30419.f1. [ Links ]
55. Lameiras, M., Rodríguez, Y., Calado, M., Foltz, M.., & Carrera, M.V. (2007). Expressive-instrumental traits and sexist attitudes among Spanish university professors. Social Indicators Research, 80, 583-599. DOI: 10.1007/s11205-006-0008-9. [ Links ]
56. Lameiras, M., Rodríguez, Y., Calado, M., Foltz, M., & González, M. (2006). Sexism, Vocational Goals, and Motivation as Predictors of Men's and Women's Career Choice. Sex Roles, 55, 267-272. DOI: 10.1007/s11199-006-9079-y. [ Links ]
57. Landry, L.J. (2007). Sexism and women's mental healt: The moderating roles of level and stabilty of self-esteem. Dissertation Abstracts International: Section B: The Sciences and Engineering, 68(4-B) 2713. [ Links ]
58. Lourenco, L., Blanes, L., Salomé, G.M., & Ferreira, L.M. (2014). Quality of life and self-esteem in patients with paraplegia and pressure ulcers: A controlled cross-sectional study. Journal of wound care, 23, 331-337. DOI: 10.12968/jowc.2014.23.6.331. [ Links ]
59. Martínez, C., Paterna, C., & Yago, C. (2010). Justifications and Comparisons in the Division of Household labor. The relevance of Gender Ideology. The Spanish journal of Psychology, 13, 220-231. DOI: 10.1017/S1138741600003802. [ Links ]
60. Masser, B., & Abrams, D. (1999). Contemporany Sexism. The relationship among hostility benevolence and neosexism. Psychology of Women Quarterly, 23, 503-573. DOI: 10.1111/j.1471-6402.1999.tb00378.x. [ Links ]
61. Moradi, B., & Subick, L.M. (2004). Examining the Moderating Role of Self-Esteem in the Link Between Experiences of Percived Sexist Events and Psychological Distress. Journal of Counseling Psychology, 51, 50-56. DOI: 10.1037/0022-0167.51.1.50. [ Links ]
62. Moya, M. (2004). Actitudes sexistas y nuevas formas de sexismo. In E. Barberà & I. Martínez-Benlloch (Eds.): Psicología y género (pp. 271-294). Madrid: Pearson Prentice Hall. [ Links ]
63. Moya, M., & Expósito, F. (2001). Nuevas formas, viejos intereses: neosexismo en varones españoles. Psicothema, 13, 643-649. [ Links ]
64. Moya, M., Expósito, F., & Ruiz. J. (2000). Close relationships gender and career salience. Sex Roles, 42, 825-846. DOI: 10.1023/A:1007094232453. [ Links ]
65. Moya, M., Navas, L., & Gómez, B. (1991). Escala sobre la ideología del rol sexual. Libro de Comunicaciones del III Congreso Nacional de Psicología Social (Vol.1), pp. 554-566. Santiago de Compostela. [ Links ]
66. Nicholls, E., Lehan, T. Plaza, S.L., Deng, V., Romero, J.L., Pizarro, J.A., & Arango-Lasprilla, C. (2012). Factors influencing acceptance of disability individuals with spinal cord injury in Neiva, Colombia, South America. Disabilty and rehabilitation, 34, 1082-1088. DOI: 10.3109/09638288.2011.631684. [ Links ]
67. Ortiz, P. (1991). Estudio sobre el autoconcepto enparapléjicos varones adultos. (Tesis doctoral), Universidad Complutense de Madrid, Madrid. [ Links ]
68. Pérez, J.I., & Garaigordobil, M. (2007). Discapacidad Motriz: autoconcepto, autoestima y síntomas psicopatológicos. Estudios de Psicología, 28, 343-357. DOI: 10.1174/021093907782506434. [ Links ]
69. Peter, C., Müller, R., Cieza, A., & Geyh, S. (2012). Psychological resources in spinal cord injury: a systematic literatura review. Spinal Cord, 50, 188-201. DOI: 10.1038/sc.2011.125. [ Links ]
70. Peter, C., Müller, R., Post, M.W., van Leevwen, C.M., Werner, C.S., & Geyh, S. (2015). Swiss spinal cord injury cohort study Group. Rehabilitation Psychology, 60, 67-80. DOI: 10.1037/rep.0000021. [ Links ]
71. Ramiro, P. (2003). Mujer y Discapacidad: Doble discriminación. Foro de Debate con la Ciudadanía sobre los Derechos Humanos. Gasteiz (Bilbao). [ Links ]
72. Richardson, A., & Tupper, A. (1975). Prognostic factors in the rehabilitation of patient with spinal problems. Postgraduate Medical Journal, 51, 161-165. DOI: 10.1136/pgmj.51.593.161. [ Links ]
73. Rodríguez, G., & Vaquero, J. (2009). Traumatismo raquimedular. Madrid: Díaz de Santos: Fundación Mapfre, Instituto de Prevención, Salud y Medio Ambiente, D.L. [ Links ]
74. Rosenberg, M. (1965). Society and the Adolescent Self Image. Princeton NJ: University Press. [ Links ]
75. Rueda, M.B., & Aguado, A.L. (2003). Estrategias de aprontamiento y proceso de adaptación a la Lesión Medular. Madrid: IMSERSO. [ Links ]
76. Russel, B., & Trigg, K. (2004). Tolerance of Sexual Harassment: An Examination of Gender Differences Ambivalent Sexism, Social Dominance and Gender Roles. Sex Roles, 50, 565-573. DOI: 10.1023/B:SERS.0000023075.32252.fd. [ Links ]
77. Schmitt, M. T., Branscombe, N. R., & Postmes, T. (2003). Women's emotional responses to the pervasiveness of gender discrimination. European Journal of Social Psychology, 33, 297-312. DOI: 10.1002/ejsp.147. [ Links ]
78. Schmitt, M.T., Branscombe, N.R., Postmes, T., & García, A. (2014). The consequences of perceived discrimination for psychological well-being: a meta-analytic review. Psychological Bulletin, 140, 921-948. DOI: 10.1037/a0035754. [ Links ]
79. Tesser, A., Felson, R., & Suls, M. (2000). Psychological perspectives on self and identuty. Washington, DC: American Psychological Association. DOI: 10.1037/10357-000. [ Links ]
80. Tougas, F., Brown, R., Beaton, A., & Joly, S. (1995). Neosexism: Plus ça change, plus c'est pareil. Personality and Social Psychology, 21, 842-849. DOI: 10.1177/0146167295218007. [ Links ]
81. Travaglia, I., Overall, N., & Sibley, C. (2009). Benevolent and hostile sexism preferences for romantic partners. Personality and Individual Differences, 47, 599-604. DOI: 10.1016/j.paid.2009.05.015. [ Links ]
82. Trieschmann, R. B. (1988). Spinal Cord Injures: The Psychological, Social and Vocational Rehabilitation. Nueva York: Demos Publications. [ Links ]
83. Vaamonde, J. D. (2013). El sexismo en el lugar de trabajo a la luz de los valores personales y de las percepciones de justicia organizacional (en línea). Tesis de posgrado. Universidad Nacional de La Plata. Facultad de Psicología. En Memoria Académica. Disponible en: http://www.memoria.fahce.unlp.edu.ar/tesis/te.903/te.903.pdf. [ Links ]
84. Van Leewen, C.M., Kraaijeveled, S., Lindeman, E., & Post, M.W. (2012). Associations between psychological factors and quality of life ratings in persons with spinal cord injury: a systematic review. Spinal Cord, 50, 174-187. DOI: 10.1038/sc.2011.120. [ Links ]
85. Wyndaele, M., & Wyndaele, J.J. (2006). Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey?. Spinal Cord, 44, 508-523. DOI: 10.1038/sj.sc.3101893. [ Links ]
![]() Correspondence:
Correspondence:
Manuela Torregrosa Ruiz.
Universitat de Valencia.
Facultad de Psicología.
Avda. Blasco de Ibañez, 21.
46010 Valencia (Spain).
E-mail: manuela.torregrosa.ruiz@gmail.com
Article received: 14-07-2015;
Revised: 26-01-2016;
Accepted: 07-03-2016

